
Abstract
Purpose:
To evaluate the long-term outcome of visual internal urethrotomy (VIU) after perineal anastomotic urethroplasty for posttraumatic pediatric posterior urethral strictures.
Patients and Methods:
Data of 22 boys who had undergone internal urethrotomy for recurrent stricture after perineal anastomotic urethroplasty for posttraumatic posterior urethral strictures between 1998 and 2008 were analyzed retrospectively regarding patient age, interval between anastomotic urethroplasty and internal urethrotomy, stricture length, surgical technique, and postoperative complications. VIU was performed in patients in whom a guidewire could be passed beyond the stricture segment. The eventual surgical success was defined as asymptomatic voiding without clinical evidence of residual stricture (good flow rate and absence of residual urine).
Results:
The mean (range) age of patients was 12.2 (3–17) years. All patients had a road traffic accident with associated pelvic fracture. The perineal approach for anastomotic urethroplasty was adopted in all. The estimated stricture length was 0.5 cm or less in 15 patients and was 0.5 to 1 cm in 7 patients. The interval between anastomotic urethroplasty and internal urethrotomy was early—after 12 weeks or less—in 13 children or late—beyond 12 weeks—in the remaining 9. The overall mean interval was 18 (5–63) weeks. In all patients, a guidewire could be passed through the strictured area. One VIU was performed in 17 patients, 2 VIU in 3 patients, while 3 VIU were performed in 2 patients. There was no extravasation reported. The mean follow-up duration was 98 (38–210) months. VIU was successful in 20 of 22 (90%) patients. All patients voided with no symptoms and were continent.
Conclusions:
VIU offers high success rate and can be sufficient in recurrent strictures of less than 1 cm length after anastomotic urethroplasty in children whenever a guidewire can be passed through the stricture area.
Introduction
Endoscopic visual internal urethrotomy (VIU) was reported in the setting of de novo strictures in different pediatric cohorts by various investigators with a reported success rate reaching 86%. 3 –7 Interestingly, repeated urethrotomies could be needed, which can further affect anastomotic urethroplasty when needed. 3,4,7 To our knowledge, there are very limited data on surgical outcome of VIU in treating patients with recurrent strictures after perineal anastomotic urethroplasty for posttraumatic posterior urethral strictures in the pediatric age group; thus, the current study was undertaken to report the outcome in such a cohort.
Patients and Methods
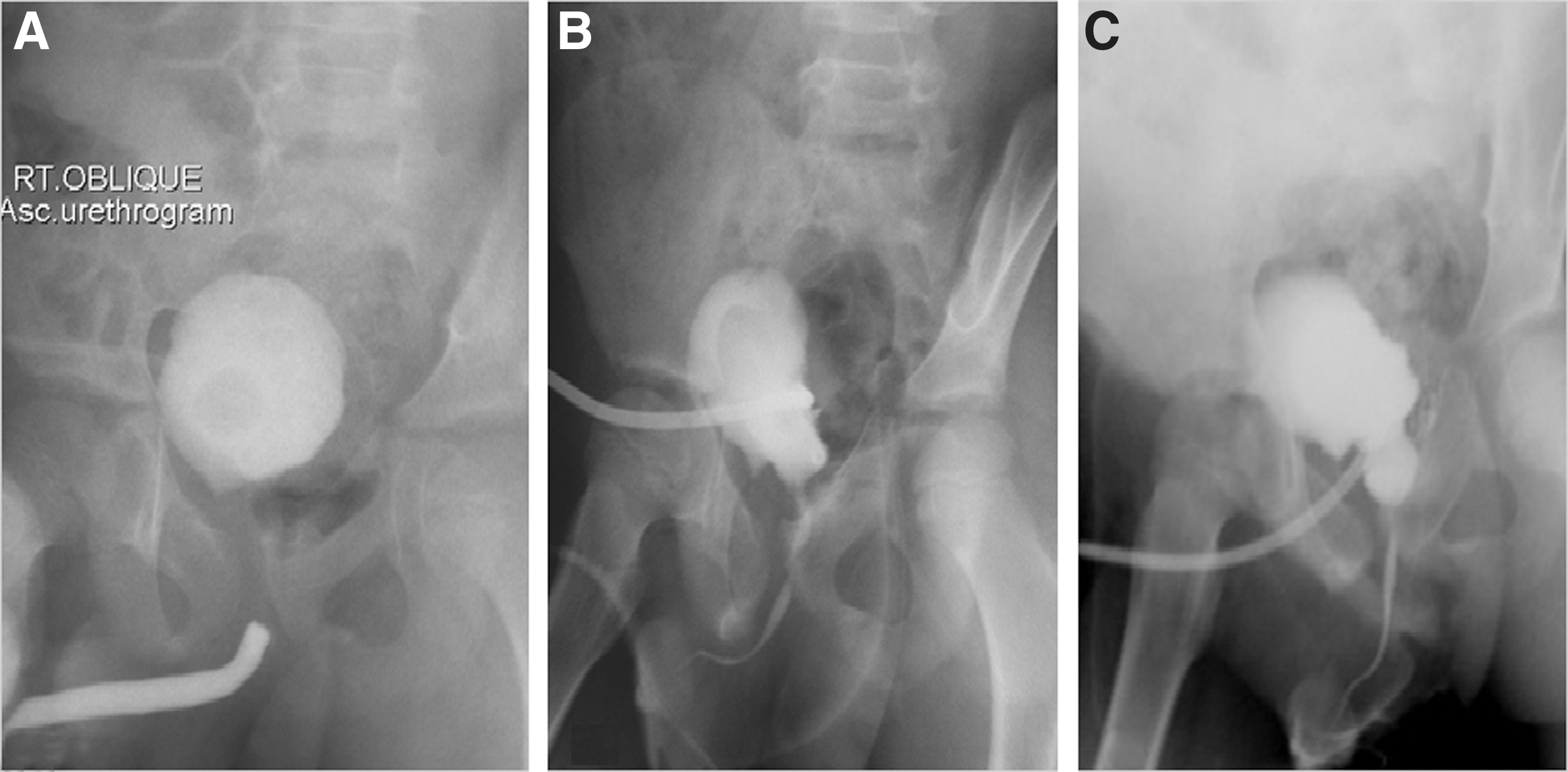
The computerized surgical records of 95 anastomotic urethroplasties performed at our institute between 1998 and 2008 were reviewed. We identified 77 boys with a history of anastomotic urethroplasty at our center, and 18 boys were referred from nearby centers. The study group includes 22 children (<18 years old) who underwent internal urethrotomy after transperineal anastomotic urethroplasty for posttraumatic stricture disease. Failure was diagnosed in 9 boys for whom urethroplasties were performed at our center and in 13 who were referred patients. Patients were followed up after anastomotic urethroplasty strictly at regular intervals and evaluated subjectively by symptomatology. Uroflowmetry was routinely used in older cooperative children. When recurrent stricture was suspected (recurrent obstructive symptoms, poor flow rates, or a large amount of postvoid residual urine), retrograde urethrography was performed (Fig. 1) Medical records of the cohort were reviewed regarding age, interval between anastomotic urethroplasty and internal urethrotomy, stricture length, surgical technique, and postoperative complications.
In all children, urethroscopy using pediatric cystoscopes was performed with the patient under anesthesia to delineate further urethral anatomy and stricture characteristics. VIU was performed in patients in whom a guidewire could be passed beyond the stricture segment. The procedure was performed under general anesthesia in all patients. Antibiotic prophylaxis was administered with an intravenous injection of third-generation cephalosporins 25 mg/kg. A cold knife urethrotome was used to incise the stricture in all patients. An incision was made at the 12 o'clock position along its entire length and depth in all patients. A Foley catheter remained for 1 week after surgery. Catheter size ranged from 8F to 14F according to the child's age. Regular self-catheterization was not used by any child. Success was defined as asymptomatic voiding without clinical evidence of residual stricture (good flow rate and absence of residual urine).
Results
All boys had been in a road traffic accident with associated pelvic fracture. The perineal approach for anastomotic urethroplasty was adopted in all. The mean (range) age of patients was 12.2 (3–17) years. The estimated stricture length was 0.5 cm or less in 15 patients and was 0.5 to 1 cm in 7 patients. The interval between anastomotic urethroplasty and internal urethrotomy was early—after 12 weeks or less—in 13 children or late—beyond 12 weeks—in the remaining 9. The overall mean interval was 18 (5–63) weeks. In all patients, a guidewire could be passed through the strictured area. The strictures were situated in the bulbomembranous part of the urethra in all patients. After a mean follow-up duration of 98 (38–210) months, of the 22 patients, 5 (23%) had recurrent stricture after primary urethrotomy and the remaining 17 (77%) had no evidence of recurrent disease and needed no subsequent procedures.
For the five patients with initial failure, repeated VIU was performed. After a second urethrotomy, another three patients (13%) had no symptoms. Therefore, the overall success rate after the second urethrotomy was 90%. After 12 weeks, a third urethrotomy was not successful in the remaining two patients, and they required open urethroplasty. Postoperatively, there was no extravasation reported, but hematuria developed in one patient; it was treated conservatively with success. Ultimately, VIU was successful in 20 of 22 (90%) patients. All patients voided with no symptoms and were continent. In postpubertal boys, all had normal straight erections with normal forward ejaculation. Chordee, urethral shortening, or urethral diverticula were not reported in any patient during follow-up.
Discussion
Pediatric urethral stricture disease represents an uncommon and devastating urologic pathology. The standard treatment of such pathology is excision of the scarred segment and restoration of urethral continuity by end-to-end anastomosis. 8 Resection reanastomosis of the posterior urethra in children has generally given favorable results in most of the published series. 9 –12
The unsuccessful results that have been described after urethroplasty include narrowing of the urethral anastomosis, obstruction at the anastomotic site, and distal retraction of the bulbar urethra from the site of anastomosis. 13 Diagnostic tools for detection of stricture recurrence include symptoms, urethrography, urethroscopy, and uroflowmetry. Morey and associates 14 reported that the American Urological Association Symptom Score is an accurate and cost-effective tool for assessment and correlates well with radiographic evidence of stricture recurrence. Retrograde or voiding urethrography can help in the diagnosis of recurrent strictures, and urethroscopy will provide the entire anatomy of the reconstructed urethra and visualize the site of anastomosis together with detection of the adjacent fibrosis. Uroflowmetry has been described and used as a noninvasive tool to evaluate the postoperative result after urethral reconstruction. Nonetheless, Erickson and colleagues 15 found that the flow rate does not appear to be a reliable tool to evaluate stricture recurrence, because 16% of men without recurrence had a maximal flow rate of <15 mL/s and 30% of men with recurrence had a flow rate >15 mL/s.
We agree with Meeks and coworkers 16 in their systematic review of stricture recurrence after urethroplasty when they found that the most common diagnostic tests for recurrence were uroflowmetry (56%) and retrograde urethrography (51%), and so in the current study, diagnosis of recurrent stricture was achieved subjectively by patient symptoms and objectively with uroflowmetry in older children and retrograde urethrography in all children. We reserved urethroscopy if urethrography demonstrated the presence of urethral narrowing to give the chance for performing VIU if the guidewire passed the strictured segment in the same session.
VIU has been reported for de novo strictures in different series; Frank and colleagues 4 reported their experience in 36 children with nonhypospadiac urethral stricture. In their study, 16 children were treated with visual urethrotomy, which was successful in 12 after a maximum of two urethrotomies, while Hsiao and associates 5 reported a success rate of 50% in a group of 40 patients treated with VIU with a minimum follow-up of 12 months. Another study by Noe 3 reported the long-term follow-up of 31 children with urethral strictures who were treated with VIU. Four children had a failed procedure and required urethroplasty, yielding an overall success rate of 87%.
Studies of the long-term success rate of VIU for management of pediatric urethral strictures have had conflicting results. In this context, in an earlier article, Hafez and coworkers 7 reported long-term results of 31 children after VIU. The success rate after initial urethrotomy was 35.5% (11 of 31 patients). A second urethrotomy improved the success rate to 58.1%.
The data describing the outcome of VIU in the setting of recurrent strictures after anastomotic urethroplasty are scarce. Hosseini and Safarinejad 2 reported early vs delayed VIU in 20 children after urethroplasty, and they concluded that the stricture-free rate was 66.6% after early and 33.3% after delayed internal urethrotomy after 5 years of follow-up. In the current study, we reported the long-term outcome after VIU in 22 children for whom anastomotic urethroplasties were performed. The length of stricture in all children was less than 1 cm. One VIU was performed in 17 patients, 2 VIU in 3 patients, while 3 VIU were performed in 2 patients. The procedure was successful in 20 of 22 (90%) patients. Others have reported successful endoscopic management of recurrent anastomotic strictures, and they attribute this success to the short stricture and a decrease in periurethral fibrosis after excision of the fibrotic segment during urethroplasty. 13,17
To our knowledge, we present the largest and longest follow-up report about surgical outcome of VIU after perineal anastomotic urethroplasty for posttraumatic pediatric posterior urethral strictures. We believe that this series may serve as a guide to consider VIU before performing a second urethroplasty in such a cohort, but on the other hand, we acknowledge the main limitation to our study is the retrospective nature of the study with small numbers. Additional future multicenter studies are needed to clarify the subject of recurrent strictures in children.
Conclusions
VIU offers a high success rate and can be a sufficient and complementary procedure in recurrent strictures of less than 1 cm length after anastomotic urethroplasty in children whenever a guidewire can be passed through the strictured area.
Footnotes
Disclosure Statement
No competing financial interests exist.