
Abstract
Purpose:
To assess the surgical efficacy and potential advantages of laparoendoscopic single-site adrenalectomy (LESS-AD) compared with conventional laparoscopic adrenalectomy (CL-AD) based on published literature.
Methods:
An online systematic search in electronic databasesM including Pubmed, Embase, and the Cochrane Library, as well as manual bibliography searches were performed. All studies that compared LESS-AD with CL-AD were included. The outcome measures were the patient demographics, tumor size, blood loss, operative time, time to resumption of oral intake, hospital stay, postoperative pain, cosmesis satisfaction score, rates of complication, conversion, and transfusion. A meta-analysis of the results was conducted.
Results:
A total of 443 patients were included: 171 patients in the LESS-AD group and 272 patients in the CL-AD group (nine studies). There was no significant difference between the two groups in any of the demographic parameters expect for lesion size (age: P=0.24; sex: P=0.35; body mass index: P=0.79; laterality: P=0.76; size: P=0.002). There was no significant difference in estimated blood loss, time to oral intake resumption, and length of stay between the two groups. The LESS-AD patients had a significantly lower postoperative visual analog pain score compared with the CL-AD group, but a longer operative time was noted. Both groups had a comparable cosmetic satisfaction score. The two groups had a comparable rate of complication, conversion, and transfusion.
Conclusions:
In early experience, LESS-AD appears to be a safe and feasible alternative to its conventional laparoscopic counterpart with decreased postoperative pain noted, albeit with a longer operative time. As a promising and emerging minimally invasive technique, however, the current evidence has not verified other potential advantages (ie, cosmesis, recovery time, convalescence, port-related complications, etc.) of LESS-AD.
Introduction
Laparoendoscopic single-site (LESS) surgery has been conceived as a natural evolution to a further reduction of surgical trauma and has been steadily gaining momentum during the past 5 years. 1,2 The population has a favorable perception of scarless surgery, even in the case of increased procedural risks of complications, in spite of cure and surgical safety being the main concerns. 3
Who would benefit from LESS most? Undoubtedly, young patients with a low body mass index (BMI) for benign indications, if there is no need to lengthen the surgical incision to extract a mass. Proof by facts, the procedure of LESS adrenalectomy (LESS-AD) is one of the most performed LESS procedures in urologic surgery. 4 In the last few years, several comparative studies of LESS-AD and conventional laparoscopic adrenalectomy (CL-AD) have been undertaken with a tendency to quicker recovery, better pain control, and improved cosmesis in the LESS group, but most are small series with conflicting results. 5 –8 Unfortunately, no prospective, randomized controlled trials (RCTs) comparing the two techniques have been performed.
Most urologists remain confused about the real advantages of LESS-AD, except the improved cosmesis. To clear up the confusion, we conducted a meta-analysis of all available comparative studies to assess the surgical efficacy and potential advantages of LESS-AD compared with CL-AD in the treatment of patients with small adrenal masses.
Methods
Literature search
The systematic review was conducted according to the Cochrane review guidelines. A systematic literature search in electronic database including Pubmed, Embase and the Cochrane Library was performed using the terms laparoendoscopic, single-site, single port, single incision, single access, and adrenalectomy. In addition, a full manual search from the list of each relevant article was also conducted. Article language was restricted to English. All relevant studies comparing LESS-AD and CL-AD were included for further screening. The searching strategy is shown in Table 1. The search was conducted on September 20, 2012.
Study selection
All available relevant RCTs (quasirandomized studies, such as those allocating by using alternate days of the admission date, were also included) and retrospective comparative studies (cohort or case-control studies) that compared LESS-AD with CL-AD in all age groups were included. Editorials, letters to the editor, review articles, case reports, and animal experimental studies were excluded. When multiple reports describing the same population were published, the most recent or complete report was used.
Two independent reviewers (LW and ZW) completed this process, and all disagreements were resolved by consensus of all authors.
Study quality assessment
The level of evidence was rated for each included study according to the criteria provided by the Center for Evidence-Based Medicine in Oxford, UK. 9 The methodologic quality of RCTs was scored with the Jadad composite scale, which is a five-point scale. 10,11 A score of two or less indicates low-quality while three or more, high-quality. 10,12 The methodologic quality of non-RCTs was assessed with the Newcastle-Ottawa Scale (NOS), 13 which is a “star system” containing eight items. It categorized three broad perspectives: The selection of the study groups, the comparability of the groups, and the ascertainment of the outcome. The NOS ranges between zero and nine stars. This procedure was independently performed by two reviewers (LW and ZW) with disagreement resolved by consensus.
Data extraction and outcomes of interest
Two independent reviewers (LW and ZW) reviewed the full texts of the included studies. The main outcome was to assess the preoperative, perioperative, and postoperative results between the two procedures. The following data were extracted from each eligible study: Authors, journal and publication year, patient demographics, tumor size, operative time, estimated blood loss, postoperative visual analog pain scale (VAPS), length of hospital stay after surgery, transfusions, surgical conversion, and complication rates.
Postoperative complications were captured in the inpatient setting and within 30 days after surgery, and classified according to the Clavien-Dindo grading system. 14 Surgical conversions in the LESS group were defined as: (1) An unplanned addition of one 5-/10-/12-mm trocar (conversion to reduced port laparoscopy) 2 ; (2) an unplanned addition of more than one trocar (conversion to CL); (3) conversion to open surgery. The use of an additional 2- to 3-mm port with puncture technique for needlescopic instruments was still considered as LESS. 15
Statistical analysis
A meta-analysis was performed to assess the efficiency, safety, and potential advantages of LESS-AD compared with CL-AD. Odds ratio (OR) or risk ratio and mean difference (MD) or standardized mean difference (SMD) were used for binary variables and continuous parameters, respectively. For studies that presented continuous data as means and range values, the standard deviations were calculated using the methodology described by Hozo and associates 16 in line with the Cochrane Handbook. 17 Pooled estimates were calculated with fixed-effect model (Mantel-Haenszel method) 18 if no significant heterogeneity was detected; otherwise, the random-effect model (DerSimonian-Laird method) 19 was used. The pooled effects were determined by Z-test, and P≤0.05 was considered as statistically significant.
The Cochrane chi-square test and inconsistency (I2) 20 were used to evaluate the heterogeneity among studies. P<0.10 indicated the presence of heterogeneity; I2<50% indicated acceptable heterogeneity. Data analysis was performed with the Review Manager software (RevMan 5.1, Cochrane Collaboration, Oxford, England).
Results
Description of included studies and quality assessment
After an initial search in the databases, 93 potential studies were identified for further retrieval (Table 1). Finally, nine studies 5 –8,21 –25 were enrolled in our meta-analysis. A flowchart of the searching is shown in Figure 1, including a total of 443 patients who underwent adrenalectomy for small adrenal masses, of whom 171 (38.6%) and 272 (61.4%) were treated with LESS-AD and CL-AD, respectively. All the included studies were observational comparative studies, including seven comparing a contemporary series of patients (level of evidence: 3b), 5 –8,21 –23 one using a historic series as control (level of evidence: 4), 24 and one of a prospective quasi-randomized uncontrolled cohort (allocation based on the order of arrival at the hospital). 25 The majority of studies 6 –8,21 –23,25 used commercially available single-port devices for access entry (ie, Triport, SILS port, Visiport, OCTO port), and one study 22 also used a homemade device based on surgical gloves, which was consistently used in another two studies. 5,24
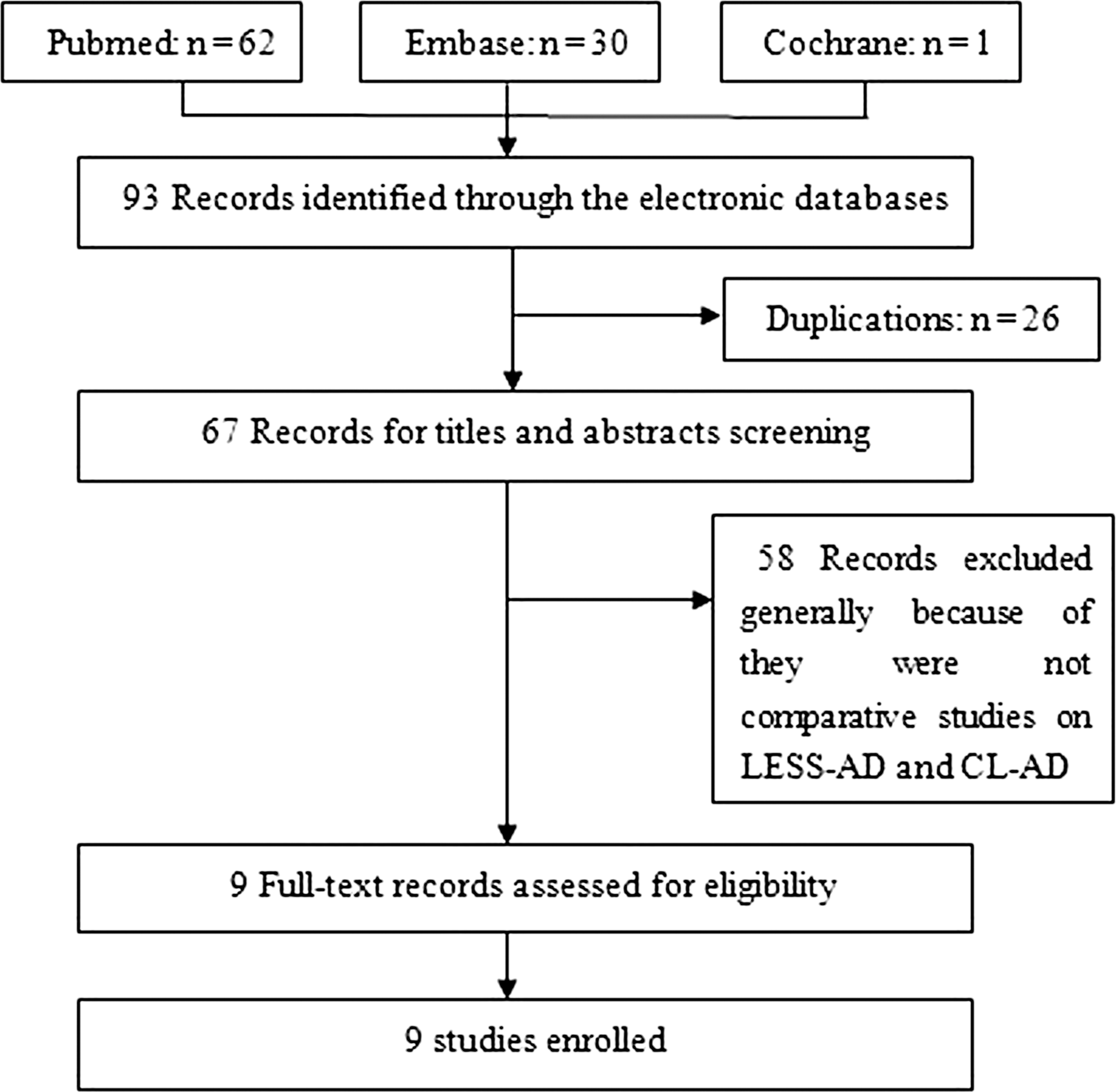
Flowchart for records selection process of the meta-analysis.
Three different access approaches were reported: Transumbilical, transperitoneal subcostal, and retroperitoneal subcostal. The methodologic quality of included studies was relatively high, with a score of six or seven stars. The baseline characteristics of included studies are shown in Table 2.
LESS=laparoendoscopic single site.
Patient demographics and perioperative outcomes
Table 3 depicted the demographics of the included studies, including number of patients, patient age, sex, BMI, laterality, adrenal lesion size, and malignant/benign pathology or radiographic finding. There was no significant difference between the two groups for any of the demographic parameters except for the size of lesions (age: [weight mean difference, WMD]: 1.90, 95% confidence interval [CI] [−1.30, 5.10], P=0.24; sex: OR: 1.21, 95% CI [0.81, 1.81], P=0.35; BMI: WMD: 0.13, 95% CI [−0.83, 1.09], P=0.79; laterality: OR: 0.92, 95% CI [0.55, 1.55], P=0.76; size: WMD: −0.69, 95% CI [−1.11, −0.26], P=0.002).
BMI=body mass index; LESS=laparoendoscopic single site; CL=conventional laparoscopic; AD=adrenalectomy.
According to the preoperative radiological finding if no final pathologic information provided in the whole text.
Three bilateral surgeries both in LESS-AD and CL-AD.
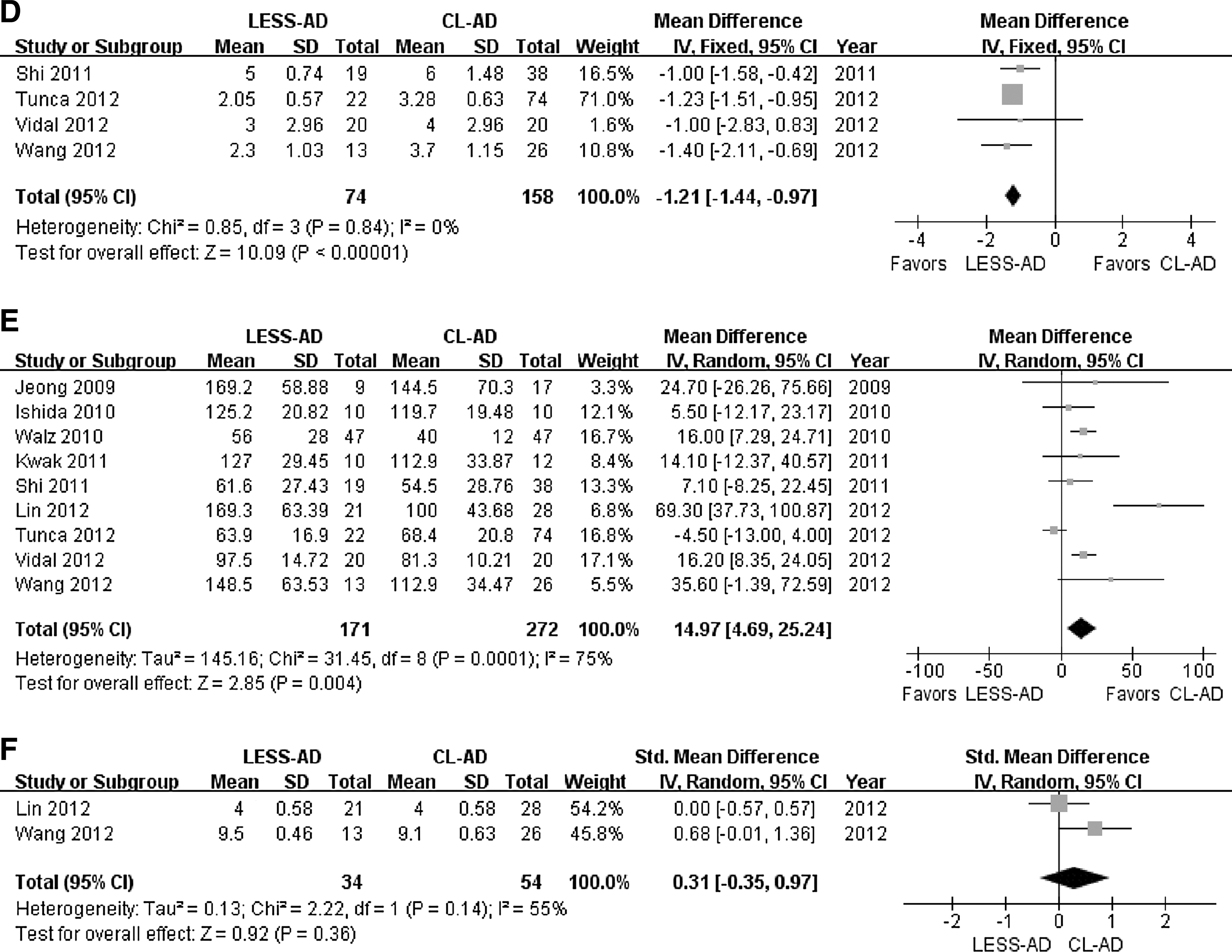
There was no significant difference between the two groups regarding estimated blood loss (WMD: −1.40, 95% CI [−9.72, 6.91], P=0.74) (Fig. 2A), time to oral intake resumption (weight standardized mean difference [WSMD]: −0.40, 95% CI [−0.87, 0.07], P=0.09) (Fig. 2B), and length of stay (WMD: −0.50, 95% CI [−1.02, 0.02], P=0.06) (Fig. 2C). The LESS-AD patients had a significantly lower postoperative VAPS score (WMD: −1.21, 95% CI [−1.44, −0.97], P<0.00001) (Fig. 2D) compared with those in CL-AD, but LESS-AD patients needed longer operative time (WMD: 14.97, 95% CI [4.69, 25.24], P=0.004) (Fig. 2E). Both groups had a comparable cosmetic satisfaction score (WSMD: 0.31, 95% CI [−0.35, 0.97], P=0.36) (Fig. 2F).
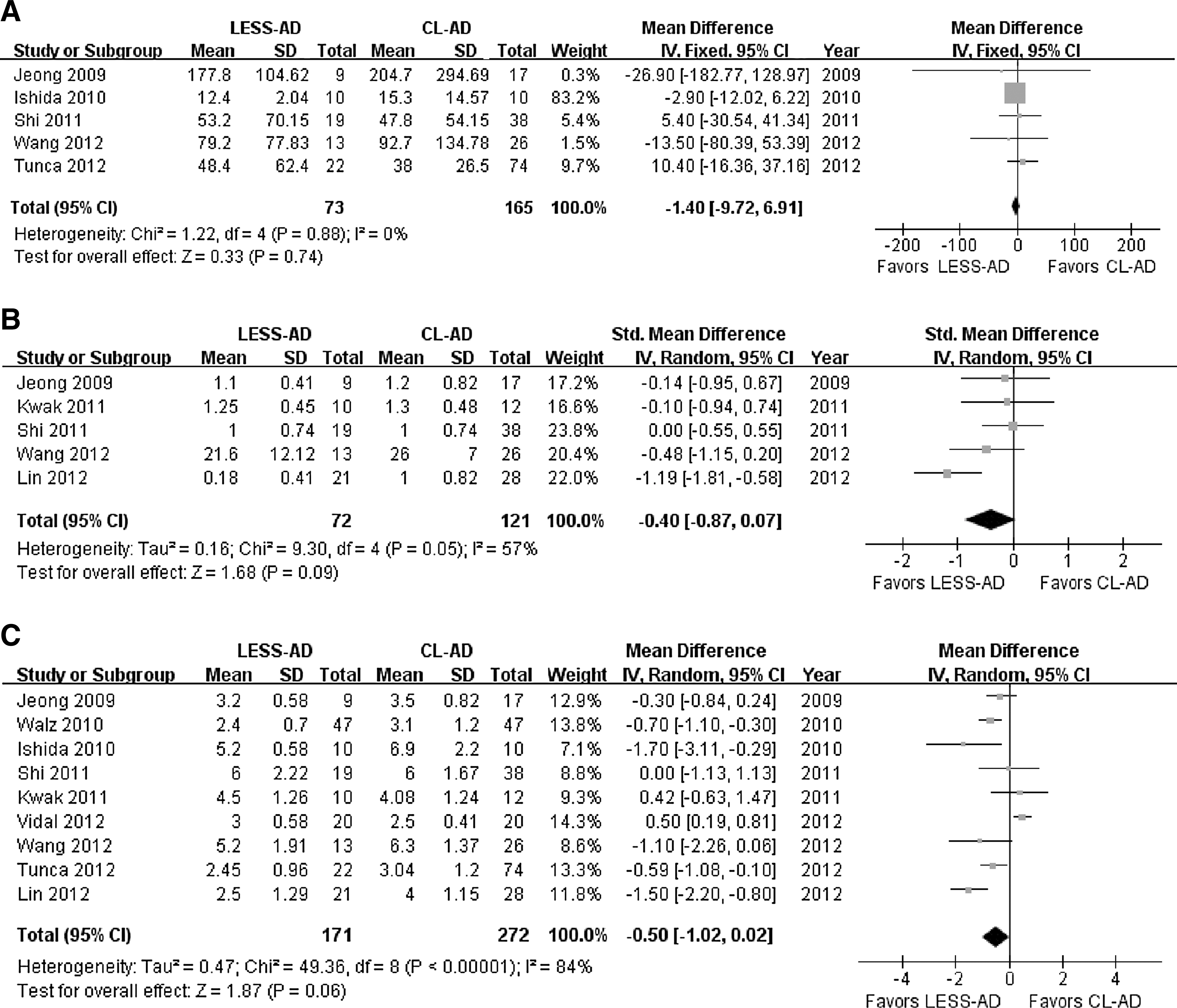
Forest plots of perioperative outcomes: (A) Estimated blood loss; (B) time to oral intake resumption; (C) length of stay; (D) visual analog pain scale; (E) operative time; and (F) cosmetic satisfaction. LESS-AD = laparoendoscopic single-site adrenalectomy; CL = conventional laparoscopic; SD = standard deviation; CI = confidence interval; Std = standardized.
With regard to adverse events, there was no significant difference between the LESS-AD and CL-AD groups in terms of surgical complication rate (OR: 1.83, 95% CI [0.88, 3.81], P=0.10), total conversion rate (OR: 4.66, 95% CI [0.88, 24.64], P=0.07), and transfusion rate (OR: 1.15, 95% CI [0.14, 9.16], P=0.13) (Fig. 3).
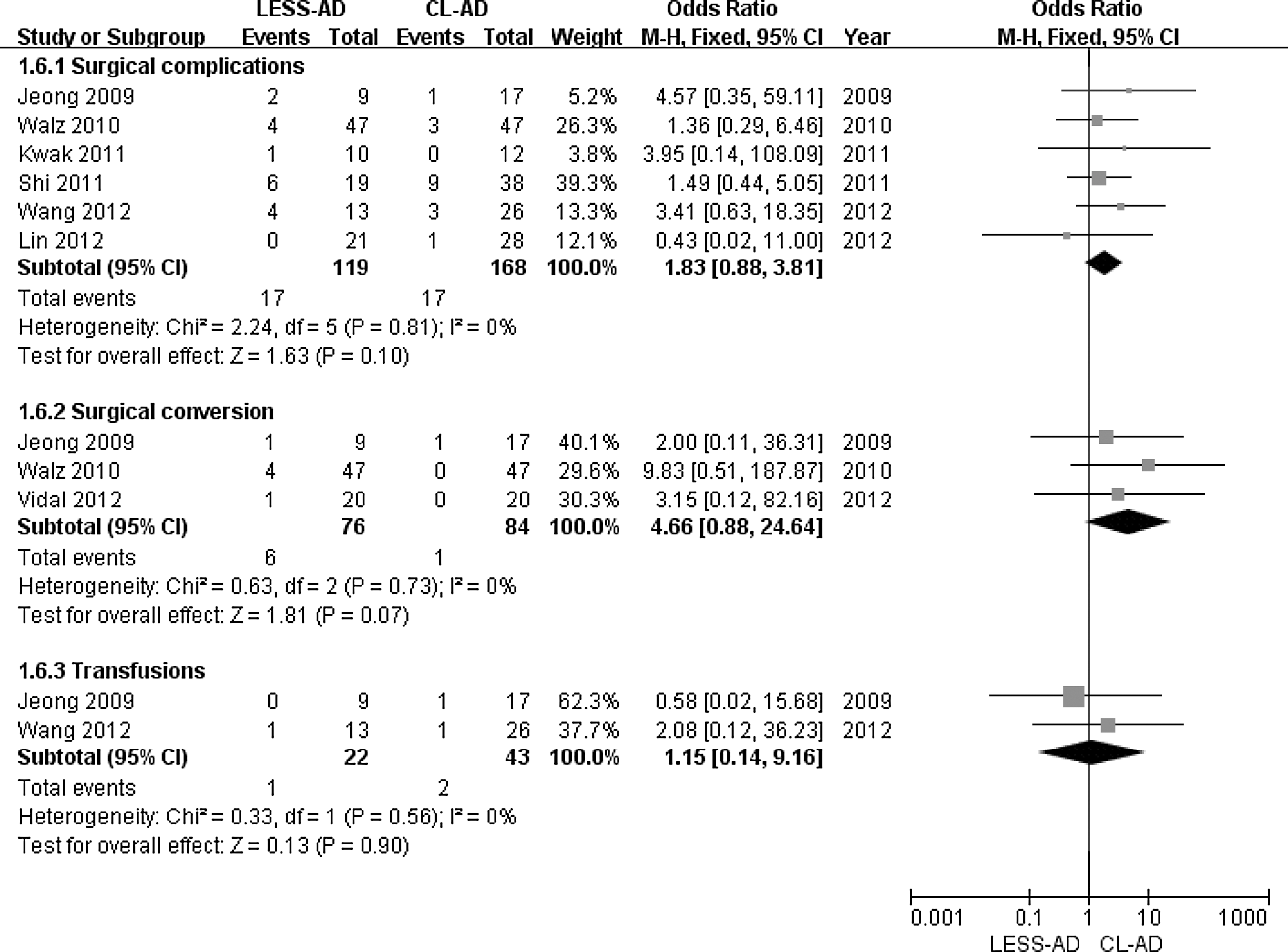
Forest plots of complication rate, conversion rate, and transfusion rate. LESS-AD=laparoendoscopic single-site adrenalectomy; CL=conventional laparoscopic; CI=confidence interval.
Discussion
LESS has been developed with the hypothesis that minimizing the number of skin incisions needed to gain access to the abdominal or pelvic cavities may benefit patients in regard to pain control, convalescence, cosmesis, and access-related complications. Driven by these intuitive advantages, the world experience in urologic LESS is steadily increasing. 2
LESS-AD is one of the most appealing procedures, because there is neither need to enlarge the incision to remove the specimen at the end of the surgery nor intraoperative reconstruction needed. 4 Many studies revealed the feasibility and safety of LESS-AD. 26 –29 In addition, several comparative studies have demonstrated that LESS-AD duplicates the perioperative outcomes of conventional laparoscopic surgery, with objective patient benefits in terms of better postoperative pain control and less analgesic requirement, 5 –8,23,24 quicker time to oral intake, 8,24 shorter recovery time, 6,23,24 or improved cosmesis. 8 Other studies, however, examining the objective advantages of LESS-AD compared with its laparoscopic counterpart, have not reproduced these findings. 22,25 In the present study, we provided the overall efficacy and safety of LESS-AD compared with that of CL-AD, based on the currently available comparative studies of these two procedures.
In contrast to individual studies, no significant differences were detected in recovery of bowel function and hospitalization in the present meta-analysis. For one thing, the further invasiveness reduction achieved in LESS is not as obvious as that obtained from open surgery to standard laparoscopy. For another, the process of postoperative recovery is complex, and many factors have major influences on this process (ie, preoperative nutritional status, patient age, comorbidities, etc.).
The indirect benefit of quicker recovery achieved by removing several small skin incisions from the procedure of LESS-AD, if it exists, is subtle compared with CL-AD, and a well-designed prospective comparative study with a large patient sample is needed to elucidate this issue. As expected, the operative time of LESS-AD is significantly longer in these early series because of the recognized unfavorable ergonomics with LESS (ie, reduced triangulation, clashing or crossing of instruments, and in-line visualization). For this parameter, great heterogeneity was observed among studies, which may derive from the learning curve effects and the different access approaches used (ie, transumbilical, transperitoneal subcostal, and retroperitoneal subcostal) with obvious distinct surgical difficulties.
One direct advantage of LESS-AD concerns postoperative pain. In our meta-analysis, the postoperative VAPS score in the LESS-AD group was significantly lower than that in the CL-AD group. Nevertheless, the VAPS score can be influenced by the amount of analgesics used. In this regard, the parameter was not consistently used (ie, number of patients needing analgesics, amount of morphine equivalent, or the duration of intravenous patient-controlled analgesia use) in the included studies of this study. The VAPS combined with the amount of morphine equivalent would better evaluate the postoperative pain. In the present study, however, we failed to carry out meta-analysis of analgesic requirement between the two groups.
Another important advantage of LESS-AD is subjectively improved cosmesis, one of the driving forces in the development of LESS surgery. Only two studies, however, reported the patient-reported cosmetic satisfaction on a Likert-type scale and pooled estimates of these data did not reveal significant difference. There is no validated survey for patient reporting of scarring outcomes after abdominal surgery, but a comprehensive survey evaluating body image, cosmetic consequences of scarring, and patient preference for future surgical approach developed by Dunker 30 has been widely used. 31 –33 Kurien and colleagues 34 and Parkand coworkers, 35 as pioneers, used this methodology to evaluate the comprehensive cosmetic outcomes after urologic LESS kidney surgery. Patient-reported body image and cosmesis outcomes analysis using such a comprehensive survey in LESS-AD, however, is still lacking to date.
Surgical safety is one of the main concerns in urologic LESS. The present study showed that the two groups had a comparable rate of surgical complications, conversions, and transfusions, and most of the postoperative complications were of lower Clavien-Dindo grades, reflecting the strict patient selection for LESS-AD. The overall complication rate and conversion rate in LESS-AD were lower than those reported in a recent global multi-institutional analysis regarding all kinds of urologic LESS surgery (overall complication rate: 9.9% vs 12.7%; overall conversion rate: 3.5% vs 19.6%). 36 The absence of demanding reconstruction in which intraoperative suturing is needed may account for these differences.
There are several limitations in the present meta-analysis. First, no RCTs were included in our meta-analysis because of lack of comparative RCTs in this field. Our study provides several implications to address those controversies with a sound methodology in future studies. Second, the long-term efficacy and safety of LESS-AD cannot be evaluated for lack of enough follow-up. Third, there is great heterogeneity among studies for some parameters. Surgeons with different backgrounds in conventional laparoscopy and LESS surgery for other urologic indications and three different surgical access approaches among studies contributed to different surgical efficiency. This might result in the heterogeneity.
Conclusions
In early experience, LESS-AD appears to be a safe and feasible alternative to its conventional laparoscopic counterpart, with decreased postoperative pain noted, albeit with a longer operative time. As a promising and emerging minimally invasive technique, however, the current evidence has not verified other potential advantages (ie, cosmesis, recovery time, convalescence, port-related complications, etc.) of LESS-AD.
Footnotes
Acknowledgments
This study was supported by the Military Major Project for Clinical High-tech and Innovative Technology of China (No. 2010gxjs057) and the Municipal Hospitals' Project for Emerging and Frontier Technology of Shanghai (No. SHDC12010115).
Disclosure Statement
No competing financial interests exist.