
Abstract
Background and Purpose:
Mini-PCNL was developed to reduce the morbidity of PCNL by using smaller tract sizes. Most mini-techniques, however, require specialized instruments and use ureteroscopes as surrogates for nephroscopes, resulting in decreased visualization, poor irrigation, and difficult fragment extraction. We describe our modified technique (mPCNL) that allows for the use of standard PCNL equipment through a tract that is smaller than standard PCNL (sPCNL) but larger than previously reported for mini-PCNL.
Technique:
After ureteral access with a coaxial anti-retropulsion device, the patient is placed in the prone position. After percutaneous access under fluoroscopic guidance, a 24F balloon dilating catheter is used to place a 24F Amplatz sheath. A standard 26F rigid nephroscope is used to complete the entire procedure, with the modification of selectively removing the outer sheath to allow the scope to fit in the smaller tract. Standard lithotripters and graspers are used, as necessary.
Role in Practice:
We have performed this technique on 52 patients with a mean stone burden of 19.4 mm. Overall stone-free rate was 100%, even for stones >2 cm. This technique allows for improved visualization and irrigation compared with other mini-PCNL procedures and obviates the need to purchase specialized equipment.
Introduction
In an effort to decrease the morbidity-related symptoms of PCNL, there have been a number of instrumentation-related modifications that have allowed for the creation of a smaller tract. These “mini-PCNL” methods were initially applied in the pediatric population, but have since been demonstrated to be effective in the adult population as well. 6,7 Although there remains a lack of a consensus on a true definition of “mini-PCNL,” theoretical benefits of minimizing the nephrostomy tract size include decreased postoperative pain, perioperative narcotic requirement, length of hospital stay, and intra-operative blood loss, in addition to resulting in improved convalescence. 8 Furthermore, a recent prospective study suggested that patients undergoing “mini-PCNL” are more likely to have a tubeless procedure, further decreasing post-operative morbidity by avoiding symptoms related to an external nephrostomy tube. 3
Although there is great variability in described techniques, the majority utilize specialized miniature instruments that are able to fit in the smaller tract sizes. This requirement to use smaller instruments, however, may impact the procedure in several ways. It addition to potentially decreasing visibility and irrigation, it precludes the use of standard PCNL equipment, thereby requiring the acquisition of new scopes and accessories, which can be costly. 2,3
We describe a “modified PCNL” (mPCNL) technique that utilizes standard PCNL equipment through a smaller nephrostomy tract, and present our preliminary experience with this modification.
Technique
Patient selection
We retrospectively reviewed our experience in treating 52 patients with our mPCNL technique. Inclusion criteria included patients with renal calculi who were being treated with a percutaneous approach. Exclusion criteria included patients with concomitant ureteropelvic junction obstruction, caliceal diverticulum, and/or ureteral strictures who were treated for these conditions at the time of PCNL. Stone size was not used as an exclusion criterion. This series represents the experience of a single surgeon (MG) at a tertiary referral medical center, and the decision of using this modified technique was at the surgeon's discretion.
Patient preparation and ureteral access
After induction with general anesthesia, routine flexible cystoscopy is performed in the modified frog-leg position, and a 0.038″ guidewire is inserted into the ureter of interest under direct vision. After confirmation of correct wire positioning, a 5F open-ended catheter or a coaxial antiretropulsion device (Percsys Corp, Palo Alto, CA) is gently advanced over the wire in a retrograde fashion, and the device is placed at the ureteropelvic junction. Retrograde urography is performed to delineate the caliceal anatomy. A Foley catheter is inserted and secured to the device with a 3-0 silk tie to prevent migration during patient positioning.
Percutaneous access
After ureteral access, the patient is transitioned to the prone position, in concert with the anesthesia team. Under fluoroscopic guidance, we use an 11.5 cm, 18-gauge diamond-tipped trocar needle (Cook Medical, Bloomington, IN) for selective caliceal puncture, and advance an 80-cm heavy duty J-wire (Cook Medical, Bloomington, IN) into the collecting system, preferably in the ureter or the desired calix. Once coiling of the wire is confirmed with fluoroscopy, the access needle can be removed. A scalpel is then used to incise the skin and fascia with the guidewire in place. Next, an Ultraxx balloon dilating set (Cook Medical, Bloomington, IN) is used to radially dilate the tract and place the included Amplatz 24F Teflon sheath.
Nephroscope setup
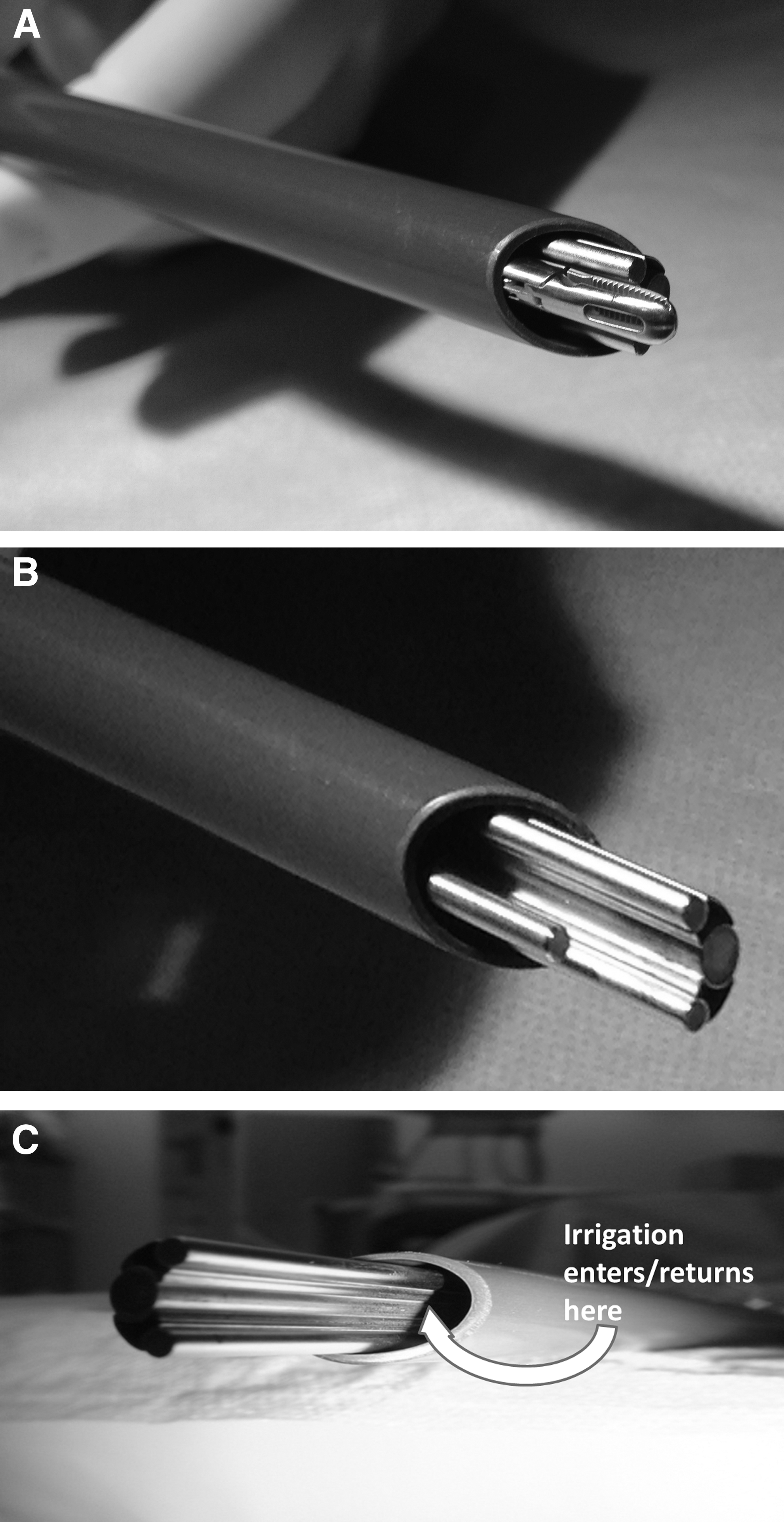
A 26F rigid nephroscope (Karl Storz, El Segundo, CA) can be used for all components of the procedure. To accommodate the smaller tract diameter for patients undergoing the mPCNL procedure, however, the outer sheath of the nephroscope is removed; no further modifications to the scope are necessary (Figs. 1A–1C).
Stone fragmentation and retrieval
The remainder of the mPCNL is then performed as usual through the smaller tract. In fact, standard ultrasonic or pneumatic lithotripters can be used to fragment and subsequently remove stone fragments. Of note, because the outer sheath and, thus, the working channel of the nephroscope has been removed, we recommend care be given to ensure that introduced instruments are inserted under vision into the nephrostomy tract. This can be achieved easily by the surgeon using fingers to keep the instrument in close approximation to the scope when inserting it into the tract, as well as visibly watching the instrument enter the sheath. In addition, we recommend using an open-ended catheter to aid in the placement of guidewires or laser fibers, because this will help ensure that the wire or fiber can be accurately directed in the absence of the outer metallic sheath; however, stents do go easily over guidewires without any significant buckling. Once the instruments are within the tract, they may be used as normal without further concern (e.g., excessive torque), and with increased experience it becomes second nature to hold the scope and instrument together.
Flexible nephroscopy can be performed easily with standard flexible cystoscopes. In cases of a concomitant ureteral calculus, antegrade ureteroscopy and basket extraction can be performed to ensure stone-free status. When appropriate, nephrostomy tubes should be placed at the end of the case, with or without ureteral stents; this is at the surgeon's discretion. Our preference is for tubeless procedures when tract bleeding is minimal; in other cases, a 14F or 16F Foley catheter is used as a nephrostomy tube. Routine follow-up care should remain consistent with standard institutional PCNL protocols.
Equipment
• Flexible cystoscope
• 0.038″ guidewire
• Coaxial antiretropulsion device (Percsys Corp., Palo Alto, CA)
• 18G trocar needle for percutaneous access
• 80cm heavy duty J-wire
• Ultraxx balloon dilating catheter set (Cook Medical, Bloomington, IN)
• 26F rigid nephroscope
• Standard lithotripters and stone graspers
• Ureteral stent and/or nephrostomy tube, as necessary
Role in Urologic Practice
Over the past 15 years, several modifications to the classic PCNL technique have been proposed in an effort to reduce the associated morbidity of this procedure. One of the efforts to decrease morbidity was to miniaturize the tract, which has popularly been termed “mini-PCNL.” Initially proposed in 1997, it was theorized that the decreased tract size would result in decreased renal trauma, thereby reducing the risk of operative blood loss, as well as postoperative pain. 6,7 Since its introduction, however, a number of modifications to the original mini-PCNL technique have been proposed, with varying results, and have led to a lack of uniformity that has limited any comparison between studies.
Despite the differences in technique, one common element is that the modifications necessitate the need for specialized instruments that can be accommodated by the miniaturized nephrostomy tract. This includes the need for specialized lithotripters and graspers, and demands the use of a smaller nephroscope or ureteroscope in place of a standard offset-lens rigid nephroscope. In addition to the added cost requirements, there are other undesired effects to this arrangement. Many of these studies report poorer visualization because of the decreased scope size, decreased irrigation and outflow, inability to use a flexible nephroscope to inspect all calices, and difficulty removing stone fragments through the smaller tract. 2 The combination of mixed results and need for specialized mini-instruments have limited the widespread implementation of mini-PCNL.
We sought to report on our modified technique to successfully perform PCNL through a smaller nephrostomy tract size without the need for special miniature instrumentation. To accomplish this, we used a balloon dilating catheter to dilate the tract to 24F, which has a 36% smaller area compared with a 30F tract. In addition, we removed the outer metallic sheath of the rigid nephroscope, which subsequently allowed us to perform PCNL using our standard scopes, lithotripters, and instruments, without compromising visualization or irrigation (Figs. 1A–1C). Although this technique has been used by select endourologists, it has not previously been scientifically studied or reported in the urologic literature.
We have successfully used this modified technique in 52 patients over the past 24 months. The mean stone burden for these patients was 19.4 mm. Overall, patients undergoing mPCNL had an intraoperative 100% stone-free rate, as defined by absence of visualized stone fragments on intraoperative nephroscopy and fluoroscopy. Operative data are listed in Table 1. It is noteworthy that in a subset of patients (n=18) with stone burdens ≥2 cm who underwent mPCNL, the technique was still successful despite the larger volume of stone. In our experience, we think that the mPCNL technique enabled us to perform procedures in patients with nondilated collecting systems that would have been more difficult or traumatic with a standard 30F access. It is especially useful in pediatric patients or those with narrow infundibula who do not have sufficient space to dilate to 30F, or accommodate a standard nephroscope with the other sheath without causing tears of the collecting system or infundibula.
EBL=estimated blood loss.
Our initial, promising results are likely because our modification subjectively resulted in enhanced visualization combined with improved irrigation, allowing for the removal of relatively large stone fragments and the use of standard PCNL equipment. Although we did not experience any adverse outcomes, one potential concern is that the edge of the unsheathed nephroscope may damage renal parenchyma or the collecting system. While the edge of a sheathed metallic nephroscope can be just as potentially traumatic to tissue, especially since the leading edge is not visible in that situation, endourologists using our modified technique should be cognizant of this possibility.
Conclusions
mPCNL can be safely performed with excellent outcomes, even for stone burdens ≥2 cm. In addition, it allows for the use of standard PCNL instruments, significantly decreasing costs normally associated with mini-PCNL. This technique may be most helpful in a pediatric population or in patients with tight collecting systems. These findings warrant prospective randomized studies to fully evaluate the advantages of this new technique relative to standard PCNL.
Footnotes
Acknowledgment
Michael Lipsky is supported by a grant from the Doris Duke Charitable Foundation and the Einstein Research Fellowship.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.