
Abstract
Objective:
Surgical treatment of kidney stones in an obese patient (body mass index [BMI] >30 kg/m2) remains challenging as shockwave lithotripsy may not be an option due to weight limitations. We sought to determine the effectiveness of ureteroscopic laser lithotripsy in obese patients compared to nonobese controls.
Materials and Methods:
Patients from 2004 to 2007 were retrospectively analyzed providing a group of 292 patients (163 obese, 76 overweight, 53 normal) who underwent ureteroscopic procedures for urolithiasis at four centers in the United States and Canada.
Results:
The percentage of obese patients requiring flexible ureteroscopy (URS) (79%) was higher than in the other groups (P<0.0001). Flexible URS was associated with a lower stone-free rate (SFR) on multivariate analysis (P=0.034). There was no difference in SFRs of patients who required a ureteral access sheath, basket extraction, or received a postoperative stent. Complication rates did not differ between groups.
Conclusion:
SFRs using ureteroscopic lithotripsy in obese and overweight populations are the same as in the normal weight patients. A flexible ureteroscope was associated with a decreased SFR, but this likely due to a more proximal stone location in these patients. Ureteroscopic laser lithotripsy is an effective and safe technique to treat urolithiasis in the overweight/obese patient.
Introduction
Shockwave lithotripsy (SWL) is often first-line treatment for proximal ureteric and renal stones up to 2 cm in size. 5 Stone-free rates (SFRs) up to 92.6% and 97.5% have been achieved for stones in the proximal and distal ureters, respectively, in a third generation SWL device. 6 Ureteroscopy (URS) with holmium:YAG laser lithotripsy is an alternative modality for patients who may not qualify for SWL due to a large skin-to-stone distance (SSD), 7 morbid obesity, or anticoagulation. URS achieves SFRs superior to SWL. For example, in a meta-analysis of five randomized control trials comparing SFRs of SWL versus URS, a higher SFR was found with URS compared to SWL although URS was associated with a higher complication rate. 8 These results do not apply to lower pole calculi, where the SFRs are largely equivalent between the techniques. 9
Achieving a high SFR utilizing URS typically requires general anesthesia, which in the morbidly obese is associated with higher associated risks, most commonly cardiorespiratory compromise. 10,11 SWL on the other hand, is often performed under sedation or patient-controlled anesthesia with decreased cardiorespiratory risk. 12 Although SWL has fewer complications and is safer relative to URS, it is associated with lower SFRs and may require repeated treatments. 13 Stone fragmentation in obese patients can also be suboptimal as most lithotripters have a maximum focal point of 12 to 14 cm, 14 although such estimated values may not always be useful for large SSDs. 7 In severe to morbid obesity, body mass index (BMI) >35 kg/m2, SWL may not be possible due to a large SSD or weight limitations of the lithotripsy table.
Given these challenges in the management of upper tract urinary stones with SWL in the obese population, retrograde URS can circumvent the disadvantages of SWL and generally achieve a high SFR. In the present study, we compared the efficacy and safety of ureteroscopic lithotripsy of urinary stones in obese patients with that of nonobese controls at four centers in the United States and Canada.
Materials and Methods
Chart data from 2004 to 2007 were collected for all patients undergoing ureteroscopic procedures for urolithiasis after the Institutional Review Board Approval at four tertiary U.S. and Canadian centers. Consecutive patients from this period were included in the study and retrospectively analyzed. Procedures were performed by fellowship-trained endourologists. URS was performed in accordance with each institution's standard practice utilizing the Holmium:YAG laser. The decision to use ureteral access sheaths (UASs) or baskets was left to the discretion of the treating surgeon. Further to that, the technique of either fragmenting the stones into dust for later passage or using active retrieval with a basket during the URS was also left to the surgeon's discretion. It was always the intention to render the patient stone-free and not perform any staged or secondary procedures.
Obesity was defined according to the World Health Organization guidelines. The BMI was calculated by taking weight in kilograms and dividing it by height in squared meters (kg/m2). For our analyses, patients were categorized as normal weight (BMI <25 kg/m2), overweight (25–30 kg/m2), or obese (BMI >30 kg/m2). For all procedures, stone-free status was determined by postoperative follow-up imaging regardless of whether stones were treated by fragmenting into dust or by basket retrieval at the time of URS. The SFR was determined as the proportion of patients undergoing URS who had no evidence of stones or fragments (of any size) on postoperative imaging (computed tomography [CT] scan, kidney-ureter-bladder [KUB] X-ray, ultrasound [US], or intravenous pyelogram [IVP]). The radiologic modality employed to determine the postoperative SFR was left to the discretion of the treating urologist and the pattern of practice at their institution. All patients were imaged within 3 months following URS.
Statistical analyses were carried out using GraphPad 5 (GraphPad Software, Inc.). A P-value <0.05 was considered statistically significant. Chi-square analyses were used to compare categorical data and continuous data were screened for normality using a Kolmogarov–Smirnoff test, and then analyzed by either parametric (one-way analysis of variance) or nonparametric (Kruskal–Wallace) testing. Binary logistic regression was performed using SPSS 19 (SPSS, Inc.). A sample size of 71 was determined for the study using the University of British Columbia online statistics calculator (
Results
Of the 292 patients studied, 163 were obese, 76 were overweight, and 53 were normal controls (Table 1). Overweight patients were significantly older than normal and obese patients (p<0.0001, Table 1). Type 2 diabetes mellitus occurred in 77% of overweight patients compared to 44% of normal and 11% of obese patients (p=0.024). The maximum stone diameter was not different across the groups and ranged from 8.9 to 10.4 mm. There were no patients with partial or full staghorns. There were more category 1 American Society of Anesthesiology (ASA) patients in the normal weight group relative to the overweight and obese groups (p<0.0001). Predictably, there were more overweight and obese patients categorized as ASA 2 and ASA 3, while the only ASA 4 patients in the study were obese (n=2). Stone-free status was determined by US (38%), KUB (31%), CT (19%), IVP (3%), or other (9%, including combination KUB and US, retrograde urogram, or nephrostogram).
BMI=body mass index; ASA=American Society of Anesthesiology.
Stones in the obese group were evenly distributed throughout the urinary tract, although there were slightly more stones in the lower pole (Fig. 1). Normal and overweight patients were more likely to have distal ureteral stones (Fig. 1, p=0.0022). There was no difference in SFRs associated with proximal (renal and proximal ureter), or distal ureteric stones according to BMI (p=0.7133 and p=0.7097, respectively, Table 2). For all proximal versus distal stones in the dataset, there was an overall SFR of 75% and 67%, although this was not statistically significant via the chi-square test (p=0.2197).
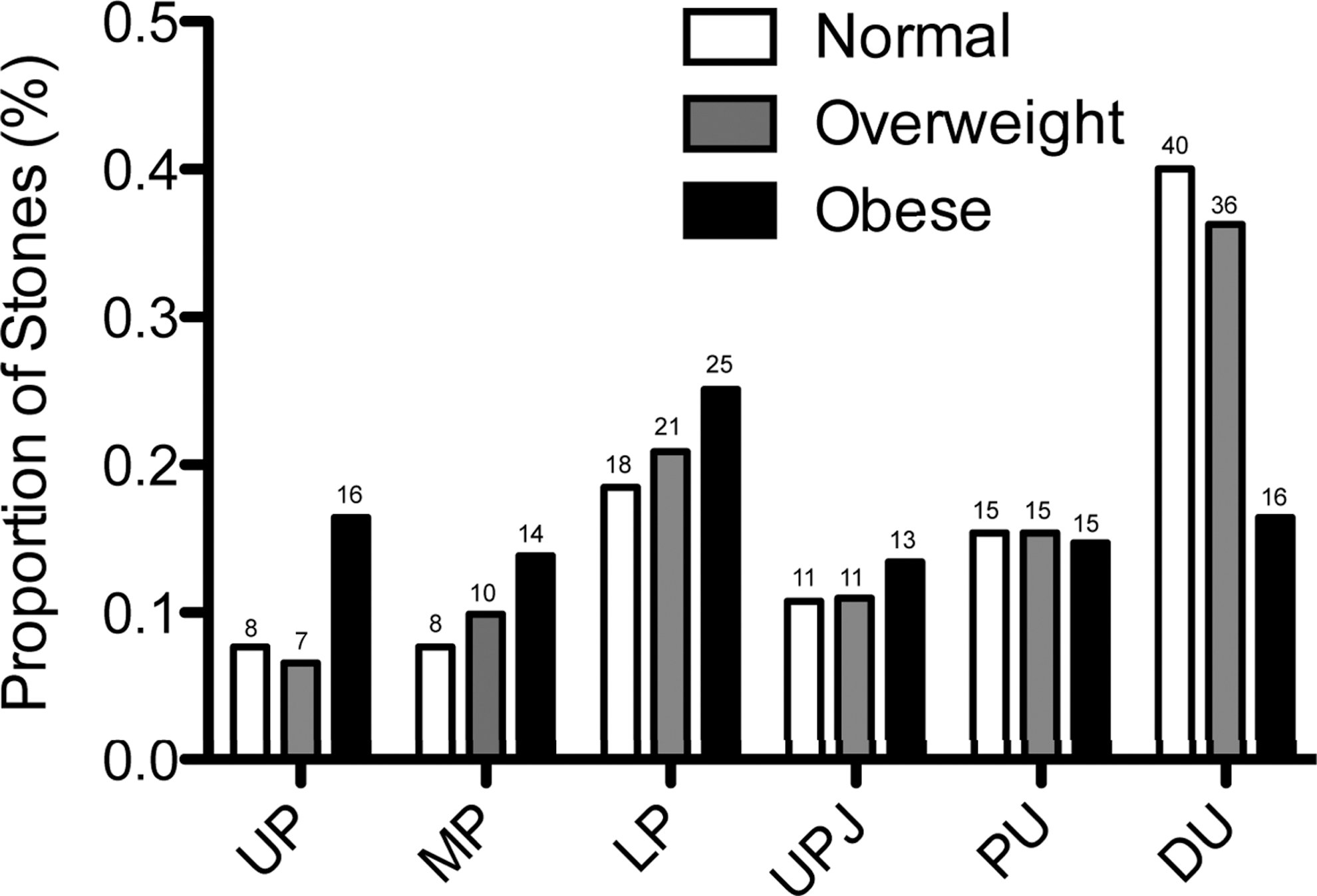
Stone locations. Stones located in the kidney or ureter were segmented as follows: upper renal pole (UP); middle renal pole (MP); lower renal pole (LP); ureteropelvic junction (UPJ); proximal ureter (PU); and distal ureter (DU). Stones located between the UPJ and above the L4 vertebra were considered to be the proximal ureter. If multiple preoperative stones were distributed throughout the urinary tract, all locations with stones were identified and used to determine the overall distribution.
SFR=stone-free rate.
The holmium:YAG laser was used in all cases. Other adjunctive devices that were used are listed in Table 2. A flexible ureteroscope (79%, p<0.0001) and UAS (45%, p=0.0592) were used more often during obese cases. Rates of basket extraction and placement of a ureteral stent were not statistically different across the groups (p=0.9982 and 0.0875, Table 2).
Complications rates following URS were not statistically different (Table 2). Overall, there were four ureteric obstructions (patient BMI 24, 31, 50, 37), one postoperative reintubation (BMI 40), one case of low postoperative oxygen saturation (BMI 27), two pulmonary emboli (BMI 26, 27), and one myocardial infarction (BMI 44). The majority of procedures were done as an outpatient procedure; however, overweight patients were more likely to stay in the hospital compared to normal weight or obese patients (p=0.0030, Table 2).
The overall SFR following URS was 66%, 75%, and 70% in normal, obese, and overweight patients, respectively (p=0.5938, Fig. 2a). A univariate analysis was performed to determine if the device choice affected the SFR (Fig. 2b–e). Normal and obese patients requiring a flexible versus a rigid ureteroscope had lower SFRs (p=0.0002, Fig. 2b). Overweight patients had a higher SFR when a UAS was used, whereas a higher SFR was found in normal weight patients who did not have a UAS used during the procedure (p=0.0283, Fig. 2c). In the overweight group, use of a UAS did not affect the SFR. Use of a basket or ureteral stent did not affect the SFR of any group (p=0.1956 and p=0.8176, respectively, Fig. 2d, e). Interestingly, of the eight super obese patients in the dataset (BMI >50), 37.5% (3/8) were stone-free.
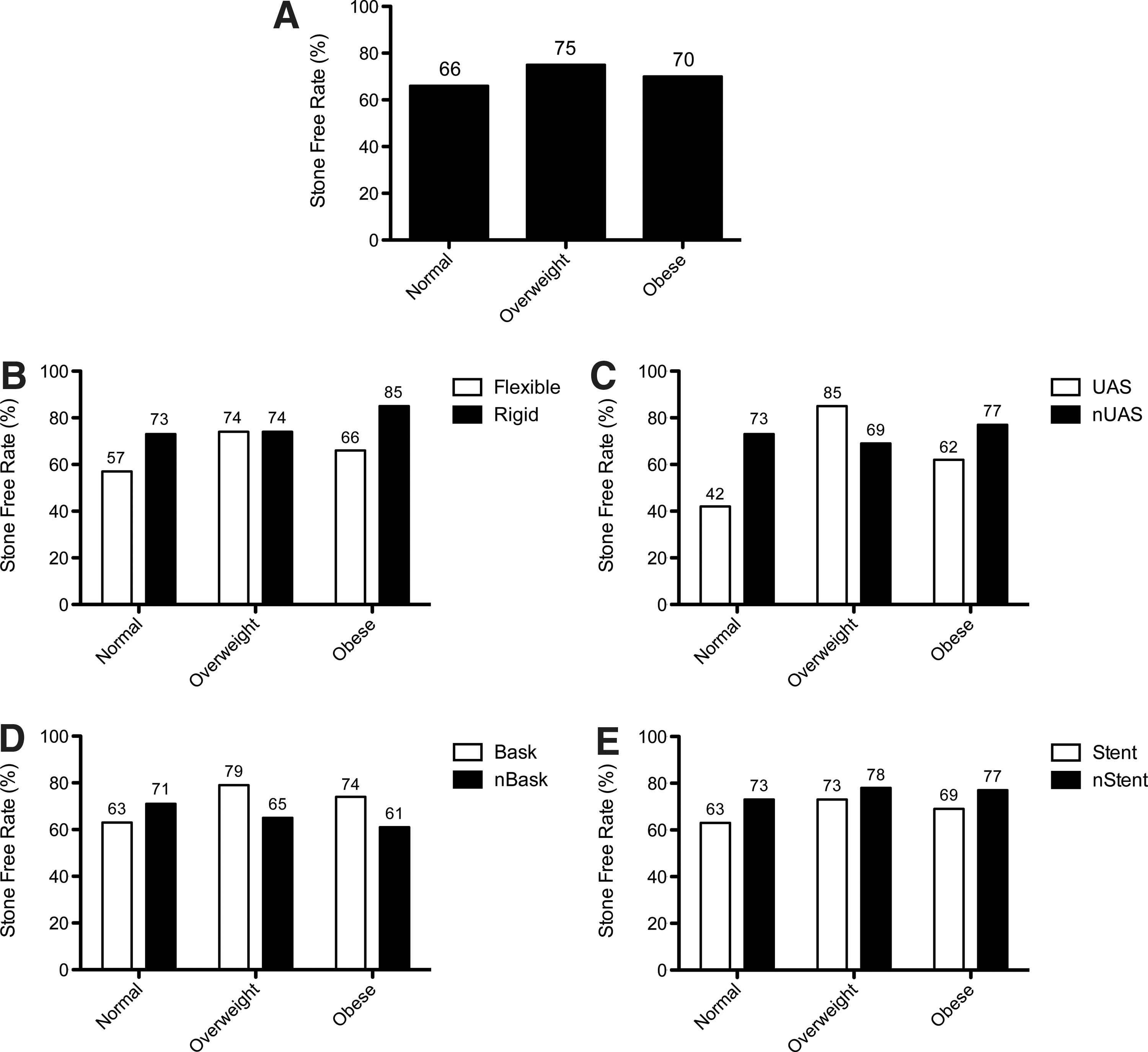
Stone-free rates (SFRs). SFRs were calculated for all patients with verified postoperative stone-free status. The overall SFR is shown in
To further evaluate the affect of a device, stone location, and patient factors such as BMI, ASA category, and diabetes on the SFR, we performed a binary logistic regression using these factors as covariates. Of the covariates, the stone location had the most significant odds ratio (0.475, p=0.059), although this was of borderline significance in this analysis. The use of the other devices as well as the patient-specific factors, were not found to influence the SFR in our regression analysis (Table 3).
CI=confidence interval; DM=diabetes mellitus; UAS=ureteral access sheaths.
Discussion
Our data suggest that (1) obese patients have equivalent outcomes compared to normal weight patients following URS, (2) operative devices used during URS (baskets, UASs, and stents) do not affect the SFR, (3) an increased BMI is associated with a prolonged hospital stay, but an equivalent complication rate to nonobese patients. Our results are consistent with others describing equal efficacy of URS in obese compared to nonobese patients. 15 This is consistent with the concept that external obesity does not necessarily correlate with an aberrant internal anatomy; factors such as increased retroperitoneal fat in obese patients do not clearly influence the ability of the operator to gain access to the ureter. As such, normal BMI patients do not as such gain a SFR advantage versus obese patients. In a series of eight cases of patients with morbid obesity, the SFR was 70% following URS. 16 Even after one URS treatment, an SFR of 78% has been shown in 30 morbidly obese patients. 17 Our dataset contained a small subset of super obese patients with a relatively low SFR, which might suggest that the efficacy of URS in obese patients declines at extreme body habitus, despite its relative efficacy for the majority of obese patients; however, this was only based on eight patients, so a more detailed investigation would be necessary in this group. We did find a statistically significant association for low SFRs and use of a flexible ureteroscope or UAS in both normal and obese patients by univariate analysis. On multivariate analysis, there was a trend for the stone location to be predictive of the SFR, but this was not significant across all weight classes. It might be inferred that procedures for distal ureteral stones accessed with semirigid ureteroscopes are typically more successful than for proximal renal stones regardless of the use of a flexible scope. The SFR as such during URS depends on the stone location to a greater extent than the modality used. The stone location dictates the technique employed to extract the stones as well as the SFR and any advantage gained by one modality versus another is outweighed by the location with respect to the SFR. A large URS series has reported a SFR of 98% in the distal ureter compared to 84% clearance in the kidney following URS. 18 Flexible ureteroscopes were used for the majority of our renal cases, but only in 20% of our cases where the stone was in the distal ureter (data not shown). Similarly, the trend to lower the SFR with the use of a UAS in normal weight patients is likely a consequence of the same inverse relationship between a reduced SFR and a proximal stone location.
Our data show that the use of a basket or stent is not necessary in all cases as it does not affect the SFR and avoiding these may prevent potential complications and patient morbidity. Complications from basket extraction include ureteral perforation, avulsion, and nephrectomy. 19 Stents are associated with dysuria, flank pain, hematuria, migration, and urosepsis. 20
The mean age of overweight subjects in our dataset was at least 7 years greater than either the normal or obese groups. The increased prevalence of diabetes and ASA 2 status is consistent with this finding. Accumulation of weight, in our overweight patients, may have been a simple consequence of aging in these patients, resulting in delayed stone formation and presentation with urolithiasis later in life.
Stones in our obese patients were distributed broadly throughout the urinary tract. Obese patients were less likely to have had SWL treatment before URS compared to normal weight patients. A morbidly large body habitus might restrict the efficacy of SWL, or increase the risk of complications following percutaneous nephrolithotomy (PNL). As such, individual urologists may be more likely to recommend URS on first presentation, even for larger stones.
Patients with an elevated BMI were more likely to have a prolonged hospital stay relative to normal weight patients who more frequently undergo URS as an outpatient procedure, which is consistent with a report of 14,407 patients who underwent various surgical procedures. 21 The obese patients in our study are subject to the same comorbidities that accompany a high BMI just as in the nonstone forming general population. They represent a group with higher in-hospital mortality necessitating larger over health care expenditures, which are not dissociated from the overall length of stay. Although the exact number is not known from our data, many of these patients had a planned overnight stay in the hospital because of their BMI and comorbidities (e.g., sleep apnea). Despite this, we failed to find a statistically significant difference in the prevalence of confirmed postoperative complications between patient groups. Nevertheless, we must stress the importance of vigilant postoperative monitoring following URS in obese patients given the known risk of cardiopulmonary complications, and comorbidities that affect recovery. 11,22,23
One shortcoming of this study is that patients had different imaging techniques to determine stone-free status. We had to accommodate for differences in institutional and surgeon practice patterns. While a CT scan is clearly the best method, it has also been recognized recently that stone patients are being exposed to a lot of unnecessary radiation, which may result in secondary malignancies.
In normal BMI patients, SWL is the first line therapy for stones smaller than 20, PNL for stones greater than 20 mm, and URS is reserved primarily for stones located in the mid- to distal ureter or failed SWL. Determining an appropriate treatment for obese patients should follow a similar, but slightly different algorithm. The decision of whether to perform SWL depends on the patient's BMI, the effective focal length of the shockwave lithotriptor and its maximum fluoroscopic imaging capabilities. PNL is also possible in these large patients, but the center must be equipped with special equipment and supportive services such as anesthesiologists who are comfortable with obese patients, specialized surgical beds, powerful fluoroscopy machines, longer Amplatz sheaths, longer Chiba needles, longer rigid nephroscopes, and longer intracorporeal lithotripters. In the absence of these specialty items, URS can be performed, even for larger stones, but may require a prolonged single procedure or be staged over several procedures. We have shown that URS in obese patients results in equivalent stone-free outcomes with equal rates of complications to that of nonobese patients.
Footnotes
Acknowledgments
The authors would like to express their gratitude to Olga Arsovska, from the University of British Columbia, Department of Urologic Sciences, who played an integral role in providing research support, coordinating the data collection, and drafting the article.
Author Disclosure Statement
No competing financial interests exist.