
Abstract
Upper tract urothelial carcinoma has a high recurrence rate after endoscopic treatment. Immediate postoperative topical chemotherapy may reduce recurrences, as in bladder cancer. A reliable delivery method to the upper tract does not exist. We propose a new infusion pump technology for the delivery of topical chemotherapeutic agents to the upper tract. With the patient under general anesthesia, contrast is infused into the upper collecting system using a standard infusion pump. An optimal infusion rate is determined based on fluoroscopic filling of the upper collecting system and transduced intrapelvic pressures. Using this rate, the infusion is repeated postoperatively with the chemotherapeutic agent. We report one case of successful execution to demonstrate proof of concept. We are the first to describe retrograde upper tract chemotherapeutic irrigation with an intravenous pump. This technique may facilitate and standardize the delivery of intracavitary chemotherapy. Further investigation to determine whether it translates into improved safety and/or efficacy is warranted.
Introduction
Delivering topical chemotherapy to the UT is a major challenge. Three delivery techniques have been described; however, none has demonstrated a significant benefit in survival or recurrence rates for UTUC. 5 –14 Some experts blame an inadequate delivery system for this clinical failure. 15
Regardless of the technique used, UT chemotherapeutic delivery must be performed at low pressures to minimize serious complications, including systemic absorption, spillage of toxic drugs, sepsis, renal damage, and even death. Because of theoretical safety concerns, pump infusion has been previously avoided. 16
We propose retrograde chemoinfusion of the upper tract (RCUT), a new technology that delivers intracavitary chemotherapy uniformly, consistently, and at low intrarenal pressures. Here, the case of a patient with recurrent UTUC who was treated successfully with RCUT is reported. Institutional Review Board approval was obtained before review.
Technology
Under anesthesia, a 5F end-hole catheter is advanced in a retrograde fashion into the renal pelvis under fluoroscopic guidance (Fig. 1). Retrograde pyelography defines the UT anatomy. A Foley catheter is inserted into the bladder and placed to gravity drainage. The catheters are secured to the body with an adhesive dressing (Fig. 2). The ureteral catheter is connected with intravenous (IV) tubing to a bag of half-strength contrast on an IV pump. The circuit is run in-line with a digital pressure transducer. Before transducing pressures, air is flushed from the tubing, and the intrapelvic pressure is zeroed at the level of the kidney. UT filling and intra-pelvic pressures are monitored by fluoroscopy and pressure readings, respectively. Contrast is infused into the UT, and the rate is titrated to achieve uniform, low-pressure filling without overdistention. Once an optimal rate is achieved, serial fluoroscopic images and pressure readings are recorded at 30 seconds, 1 minute, 2 minutes, 5 minutes, and at 5-minute intervals for 30 minutes total.

Retrograde chemoinfusion of the upper tract setup. A 5F end-hole ureteral catheter, advanced into the upper collecting system, is connected via intravenous (IV) tubing to a pressure bag and a bag of either half-strength contrast or mitomycin C (MMC) running on an IV pump with differential flow regulated by a three-way stopcock. The line is flushed, zeroed to atmospheric pressure, and secured at the level of the kidney before transducing intrarenal pressures. An indwelling Foley catheter continuously drains the bladder.

Retrograde chemoinfusion of the upper tract drainage system. A Foley catheter and ureteral catheter are secured to the glans penis with a clear adhesive dressing. Mitomycin C infuses into the kidney and drains continuously via an indwelling Foley catheter into a closed drainage bag, minimizing patient and provider skin exposure to the chemotherapeutic agent.
Afterward, with the patient awake in the recovery room, chemotherapy is infused by IV pump into the renal pelvis at the same optimal rate. Chemotherapy drains via the Foley catheter into a closed bag. After the infusion, the catheters are removed, and the patient is discharged after voiding.
Role in Endourology
Results
An 80-year-old man with recurrent, bulky, low-grade UTUC in a solitary kidney, seeking renal preservation, was treated with RCUT. He had undergone three previous endoscopic treatments complicated by complete obliteration of his midpolar calices (Fig. 3F). After ureteroscopic debulking of a tumor recurrence occupying >50% of the renal pelvis and lower pole calices, RCUT was performed.
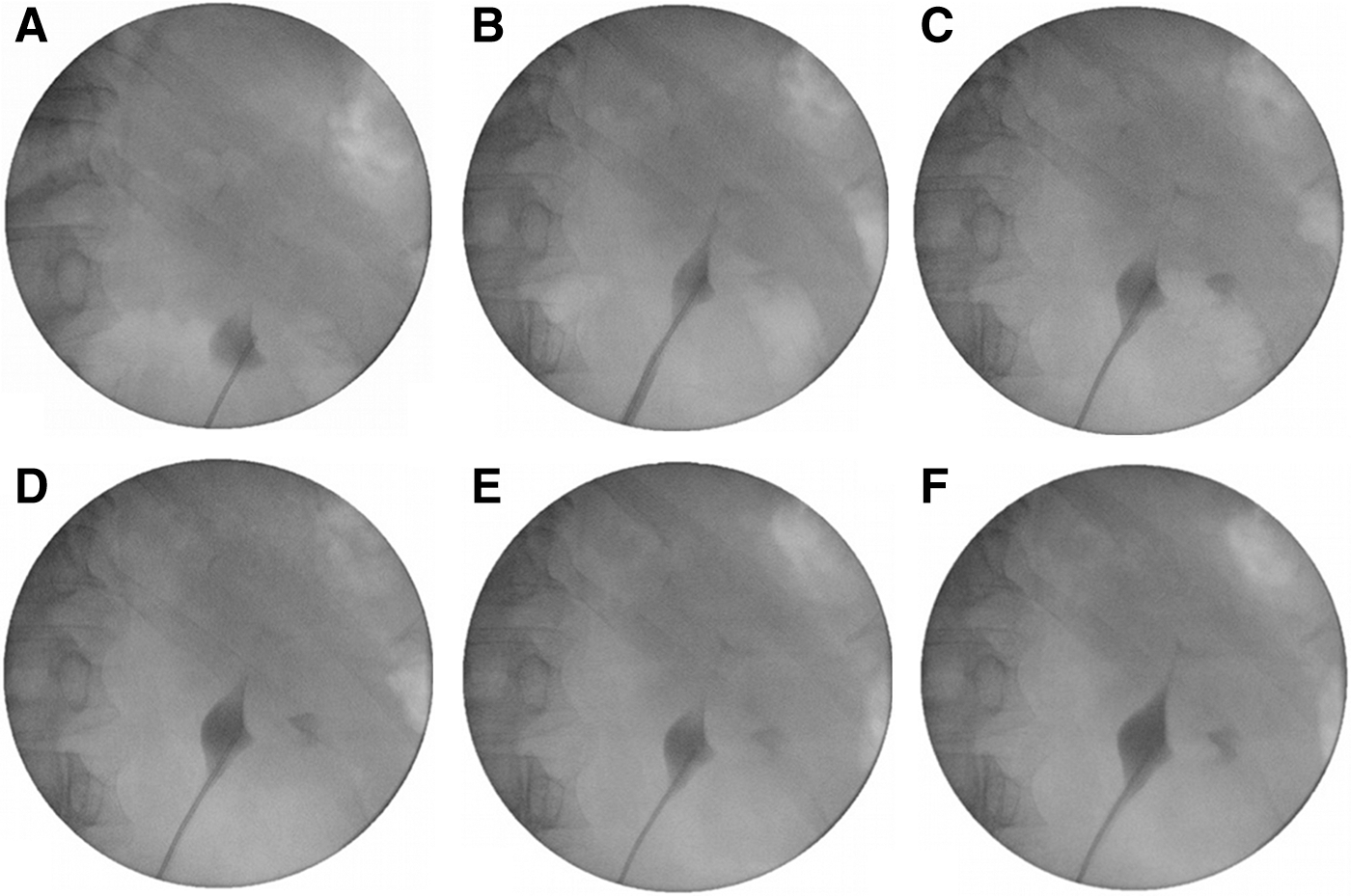
Retrograde contrast infusion with an intravenous pump. Serial fluoroscopic images demonstrate uniform filling of the upper collecting system with half-strength contrast at 2, 5, 10, 15, and 30 minutes
Contrast infused at 100 mL/h for 30 minutes (50 mL total), filling the renal pelvis and calices uniformly without pyelovenous backflow on serial fluoroscopy (Figs. 3 A–E). UT filling appeared to reach a steady state after approximately 10 minutes, resembling the retrograde pyelogram. Intrapelvic pressures were 4.9±2.2 cm H2O and never exceeded 15 cm H2O, the approximate cutoff for pyelorenal backflow. 17
Mitomycin C (MMC), 40 mg, was infused at 100 mL/h for 1 hour. The patient was asymptomatic throughout the infusion. There were no complications, including myelosuppression. There were no local ureteroscopic recurrences with 13 months of follow-up.
Discussion
Intracavitary chemotherapy has been proposed as an adjuvant treatment for UTUC. 18,19 Unfortunately, it has not shown a survival or recurrence benefit. 5,7,8,10,11,13,14 This may represent a technical failure of existing drug delivery techniques rather than a biologic failure of the chemotherapeutic agents themselves.
Much of what we know about topical chemotherapy for UTUC has been based on expert opinion and data extrapolated from BUC. 20 In the bladder, an incomplete response to topical chemotherapy is attributed to two factors: (1) Insensitivity of the tumor cells to the chemotherapeutic agent and (2) inadequate drug delivery to the tumor cells. 21 Inadequate drug delivery, a modifiable risk factor, may be caused by drug dilution and/or insufficient urothelium-drug contact time. 21,22 Before discounting the efficacy of topical chemotherapy for UTUC altogether, it seems reasonable that we should develop a standardized delivery system that minimizes drug dilution and maximizes urothelium-drug contact time.
The bladder and UT are ultrastructurally and functionally very different, and these differences must be considered when discussing UT drug delivery. The relevant differences include: (1) The UT drains rather than stores urine; (2) the upper collecting system is difficult to fill under low-pressure because of its relatively noncompliant walls; and (3) the UT's small volume is constantly diluted by urine. Consequently, the UT is prone to inadequate drug dwell time, nonuniform filling with incomplete urothelial contact, and drug dilution. Existing UT drug delivery techniques do not address these concerns.
Each of the three delivery techniques — namely, antegrade infusion through a nephrostomy tube, retrograde instillation through a ureteral catheter, and passive reflux through an indwelling stent or resected ureteral orifice — has its disadvantages. Antegrade infusion involves inherent risks, including renal parenchymal injury from percutaneous access, tumor seeding along the nephrostomy tract, drug leakage around the nephrostomy tube, infection in an open system, and patient discomfort. Extravasation of MMC outside the urinary tract, especially when delivered in a percutaneous fashion, may cause local inflammation and, potentially, tissue necrosis. Retrograde instillation necessitates intermittent manual syringe injection of the chemotherapeutic agent, which is time-consuming, laborious, and potentially harmful for both the patient and the clinician. Repeated injections increase the clinician's handling of the chemotherapeutic agent and may require overnight observation. 23 Furthermore, this technique may be inherently prone to high-pressure filling and overdistention of the UT from blind injection, leading to lethal myelosuppression in one case. 11 Reflux delivery, which necessitates stent placement, assumes that reflux to the UT is complete and consistent, an assumption that is not guaranteed, making drug delivery by this method unreliable. 24
No published studies have evaluated these techniques for their individual efficacy in achieving and maintaining urothelial-drug contact during treatment. Pollard and associates 25 are the first to present a head-on comparison between these delivery techniques in a porcine model and found retrograde instillation to be most effective. While it may achieve superior drug delivery in a static model, whether manual retrograde instillation can maintain constant drug delivery to the urothelium for an hour is another important consideration. Unlike the bladder, a hollow viscus that can be filled under gravity (e.g., cystography), the UT with its relatively noncompliant walls needs pressured filling to reach all calices (e.g., retrograde pyelography). To maintain sufficient pressured filling to contact the entire urothelial surface and not exceed safe intracavitary pressures, UT chemotherapeutic delivery needs a highly controlled approach.
Previously, the use of an IV pump for drug delivery was considered taboo, given theoretical concerns over pressurized filling leading to systemic drug absorption and/or bacterial sepsis. Although our experience is limited, we have provided hydrostatic, fluoroscopic, and clinical proof that RCUT can be accomplished at safe intrarenal pressures without causing overt pyelorenal backflow or systemic toxicity.
Despite the validity of our concept, RCUT is still investigative and needs additional refinement and testing before its universal adoption. Our present study relies on fluoroscopic filling of the UT as a proxy for urothelial drug delivery; however, pathological analyses of urothelial surface exposure and tissue absorption, as performed for intravesical chemotherapy, would strengthen our argument. 26 Optimal drug concentration is another area under active study for BUC as well as UTUC. In this case, 40 mg MMC was diluted in 100 mL of saline, a concentration previously reported for UTUC treatment. 11 Based on data suggesting that bladder tissue uptake of MMC is concentration-dependent, using a higher drug concentration for RCUT might produce improved tissue drug absorption without causing increased systemic absorption. 27 Because chemotherapy is continually infused into the UT in our treatment protocol, however, it should be less susceptible to dilution than intravesical therapy, which is continually diluted over the hour-long dwell time. RCUT is associated with additional costs, including longer operative times and extra equipment.
While critics may argue that the process of determining an optimal infusion rate is too time-consuming and expensive, we disagree. Firstly, it appears that the initial fluoroscopic study could be abbreviated safely by a third given that UT filling reaches a steady state after 10 minutes. Secondly, once an individualized UT filling rate is determined for a particular patient, we hope to apply that rate to future postoperative and maintenance drug infusions in that same patient without repeating the initial manometric and fluoroscopic investigations. By placing the ureteral catheter in the office, as previously described, maintenance infusions could be performed in a relatively automated fashion. 16 Finally, we believe that the potential long-term benefits of RCUT — i.e., fewer complications and decreased tumor recurrences — will offset its additional costs.
Topical adjuvant chemotherapy has failed to show an appreciable benefit for UTUC, and an inadequate drug delivery system may be partially to blame. This report provides proof of concept of RCUT technology. By hopefully standardizing the delivery of intracavitary chemotherapy, RCUT may facilitate accurate assessment of its efficacy in UTUC. Further experimental and clinical studies are planned to validate this concept.
Footnotes
Disclosure Statement
No competing financial interests exist.