
Abstract
Local intralumenal administration of substances with beneficial effects over the ureter appears to be a very attractive route for the administration of drugs to the urinary system, avoiding systemic adverse reactions associated with per os administration. This work investigates whether vardenafil is a good candidate for local intralumenal ureteral administration. More precisely, we examined the effect of vardenafil on human ureter contractility and on the viability of cultured human urothelial cells (hUC) and bladder smooth muscle cells (hBSMC). Our study revealed that vardenafil induced a dose-depended relaxation of isolated human ureteral tissue. In addition, growth and cell viability of cultured hBSMC and hUC remained unaltered after vardenafil application. Based on the above, this selective phosphodiesterase type 5 inhibitor can be considered as a promising pharmacologic agent for local intralumenal administration in clinical conditions in which ureteral dilation might be beneficial.
Introduction
Pharmacologic manipulation of the ureter has been proven beneficial in several clinical conditions. Systemic administration of alpha-blockers, antagonists of calcium-channel receptors, or nonsteroidal anti-inflammatory drugs (NSAIDs), for example, reduce the incidence of colic episodes and aid spontaneous stone passage in the case of ureteral lithiasis and improve ureteral stent symptoms in the case of an indwelling ureteral stent. 1 –4 Unwanted systemic side effects associated with per os administration of pharmacologic agents, such as gastropligia and interstitial nephritis related to NSAID treatment, or blood pressure alterations because of adrenoreceptor blockage or calcium-channel antagonists, pose a major limitation of current pharmacologic manipulation of the ureter.
Local intralumenal administration of substances with beneficial effects to the ureter appear to be a very attractive route for drug administration to the urinary system that could avoid drug-related systemic adverse reactions. Nevertheless, apart from technical considerations associated with retrograde administration (direct instillation during ureteroscopy, drug-eluting stents, etc), scientific pharmacologic data on the direct effect of substances over the urinary system are sparse, and further investigation is needed. In this regard, after promising experimental evidence showing that phosphodiesterase type 5 (PDE-5) inhibitors induce relaxation to ureteral smooth muscle, we examined the effect of direct vardenafil application on the ureter, examining the effect of vardenafil on ureteral contractility, as well as viability of human urothelial cells (hUC) and human bladder smooth muscle cells (hBSMC). 5
Materials and Methods
Prior approval by the Ethics Committees of the Universities of Patras and Leipzig and a written informed consent from all patients had been obtained.
Organ bath study
The protocol used in our organ bath studies has been described in detail. 6 In brief, during 10 radical nephrectomy cases, 2-cm long ureteral segments were acquired from the most distal part of the ureter on the retrieved renal specimens. Extracted samples were placed in frozen Krebs buffer (pH 7.4) and were transported to our laboratory for further investigation. Ureteral specimens were dissected free from surrounding tissues and were cut into four rings, 4 to 5 mm long each. Ureteral rings were then mounted between two hooks connected with a force transducer device and were embedded to the chambers of a ML870B5/10 Panlab organ bath system, each filled with 10 mL of fresh Krebs solution. Ureteral specimens within the organ bath remained constantly aerated with 95% O2 and 5% CO2 in an environmental temperature set at 37°C. A 4 g pretention was applied to each ring. After 60 minutes of an equilibration period, ureters were exposed to KCl (80 mM). Soon after a stable contraction state was detected, a vehicle solution (Krebs buffer) or one of the three (0.1 μM, 1 μM, and 10 μM) examined doses of vardenafil were administered. Ureteral contraction was recorded using the Labchart software (ADInstruments Ltd, Oxfordshire, UK).
Cell culture study
Cell cultures of hBSMC were established using macroscopic tumor-free segments of bladder wall obtained from three cases of radical cystectomy. Small fragments (about 0.5×0.5×0.5 cm) of the muscular layer of bladder specimens were isolated after dissection of the overlying urothelium and serosa and placed in tissue culture flasks (25 cm2, Corning, Corning, NY) filled with smooth muscle cell growth medium (PromoCell, Berlin, Germany). Cells were passaged at confluence up to four times (P4) with change of medium twice per week. Experiments were performed with P3–P4 cell cultures.
Until isolation of urothelial cells (hUC, n=3), bladder tissue probes were stored overnight at 4°C in Ca2+- and Mg2+-free Hanks balanced salt solution (HBSS) (Biochrom, Berlin, Germany) with 10 mM hydroxyethyl piperazineethanesulfonic acid (HEPES) (Invitrogen, Karlsruhe, Germany), 20.000 IU aprotinin (Calbiochem, Merck KGaA, Darmstadt, Germany), and 1% penicillin/streptomycin solution (Sigma-Aldrich, Steinheim, Germany). Urothelial cells were incubated in stripping-solution (HBSS with 10 mM HEPES, 20.000 IU aprotinin, 1% ethylenediaminetetraacetic acid) for 3 hours at 37°C. 7 Thereafter, urothelial cells were gently removed using a cell scraper in serum-free defined keratinocyte medium (KSFM 17005-075, Gibco, Invitrogen) supplemented with 30 ng/mL cholera toxin (Sigma-Aldrich). After centrifugation at 250×g for 5 minutes, the pellet was resolved in KSFM and planted into tissue culture flasks. Cells were grown with medium change every second day until confluence and passaged up to three times (P3). Experiments were performed with P2–P3 cell cultures.
For the assessment of cell viability, vardenafil was tested for possible mitogenic or apoptotic effects on hBSMC and hUC using the CellTiter-Blue® Cell Viability Assay (CTB, Promega Corp., Madison, WI). Cells were seeded at a concentration of 1.000 cells/well (hBSMC) and 2.000 cells/well (hUC) in a black 384-well μCLEAR-PLATE (Greiner bio-one, Frickenhausen, Germany). At reaching approximately 80% confluency, the cells were stimulated with different concentrations of vardenafil and grown for another 24 hours. For measurement of the cell viability/cell number, 5 μL CTB was mixed with 25 μL of culture medium removed from individual wells. After incubation at 37°C for 1 hour, the fluorescence extinction (extinction 560 nm, emission 590 nm) was measured at a SpectraMax5® microplate reader (Molecular Devices, Sunnyvale, CA). Each experiment (hBSMC, n=3; hUC, n=3) was performed in 10 replicates.
Statistical analysis
For organ bath studies, LabChart software was used to analyze ureteral tension recording data. The mean peak of amplitude after KCl administration was measured for each ureteral ring before and after vardenafil introduction. Using the t test, differences in tension before and after the administration of PDE-5 inhibitor individually for each ureteral segment were compared. Calculated differences in tension for each of the three concentrations of vardenafil were then compared by one-sample t test and (for coverage against lack of normality) the Wilcoxon signed rank test. Finally, mean vardenafil activity for every concentration was compared using analysis of variance (ANOVA) and the Kruskal-Wallis test. A level of 5% difference was considered significant.
For cell culture studies, nonparamic one-way ANOVA (Kruskal-Wallis with Dunn post-test) was performed using GraphPad Prism version 5.00 for Mac OS (GraphPad Software, San Diego, CA). A P value <0.05 was considered significant.
Results
Ureteral contractility
Histiograms compiled by the LabChart software documented a consisted response of all ureteral specimens to vardenafil. Initial administration of KCl induced an immediate increase in the recorded tension of all viable samples. In several samples, spikes of transient and sharp amplitude increase were observed during the increase of tension, before ureteral strips reached a steady contraction state. Vehicle infusion did not alter significantly the recorded ureteral ring tension during the 30 minutes of observation. Vardenafil administration resulted in a dose-dependent reduction of tension on all tested ureteral rings (Fig. 1). Statistically significant reduction in ureteral contraction was noted when Vardenafil 1 μM or 10 μM was administered. In the higher tested dose of 10 μM, a 30% reduction of KCl-induced contraction was recorded. Ureteral contraction results are summarized in Table 1.
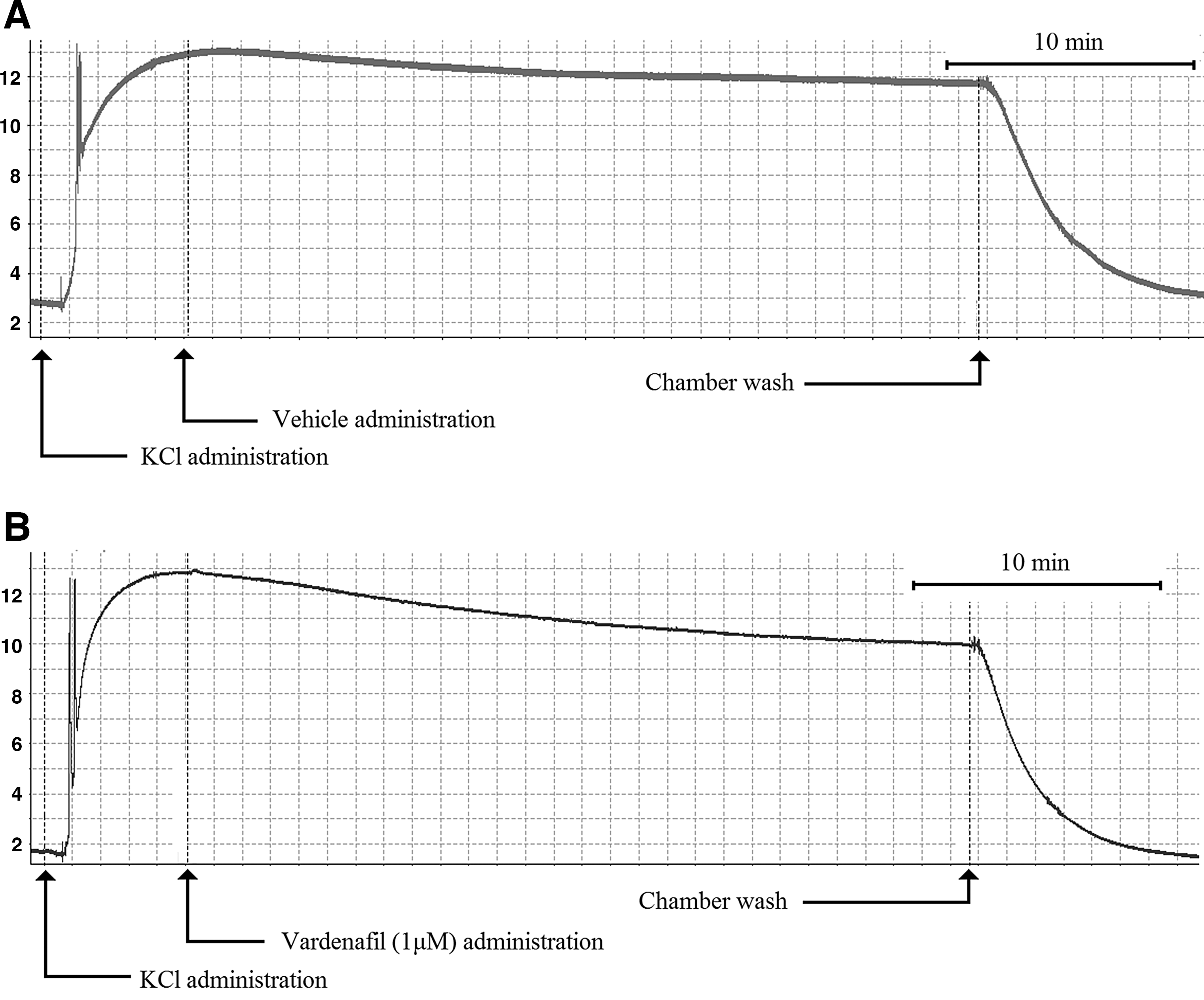
Contractility recordings from vehicle treated
The Effect of Vardenafil on Ureteral Contractility
n=number of examined ureteral rings; g=grams; ns=not significant difference.
Cell viability
Cultured hBSMC and hUC essentially showed no significant differences in growth or cell viability measured by CellTiter-Blue Cell Viability Assay when treated with the three different concentrations of vardenafil for 24 hours (Fig. 2). Human urothelial cells showed a tendency to decreased cell numbers with increasing vardenafil concentrations, which, however, were not significant (Fig. 2B).
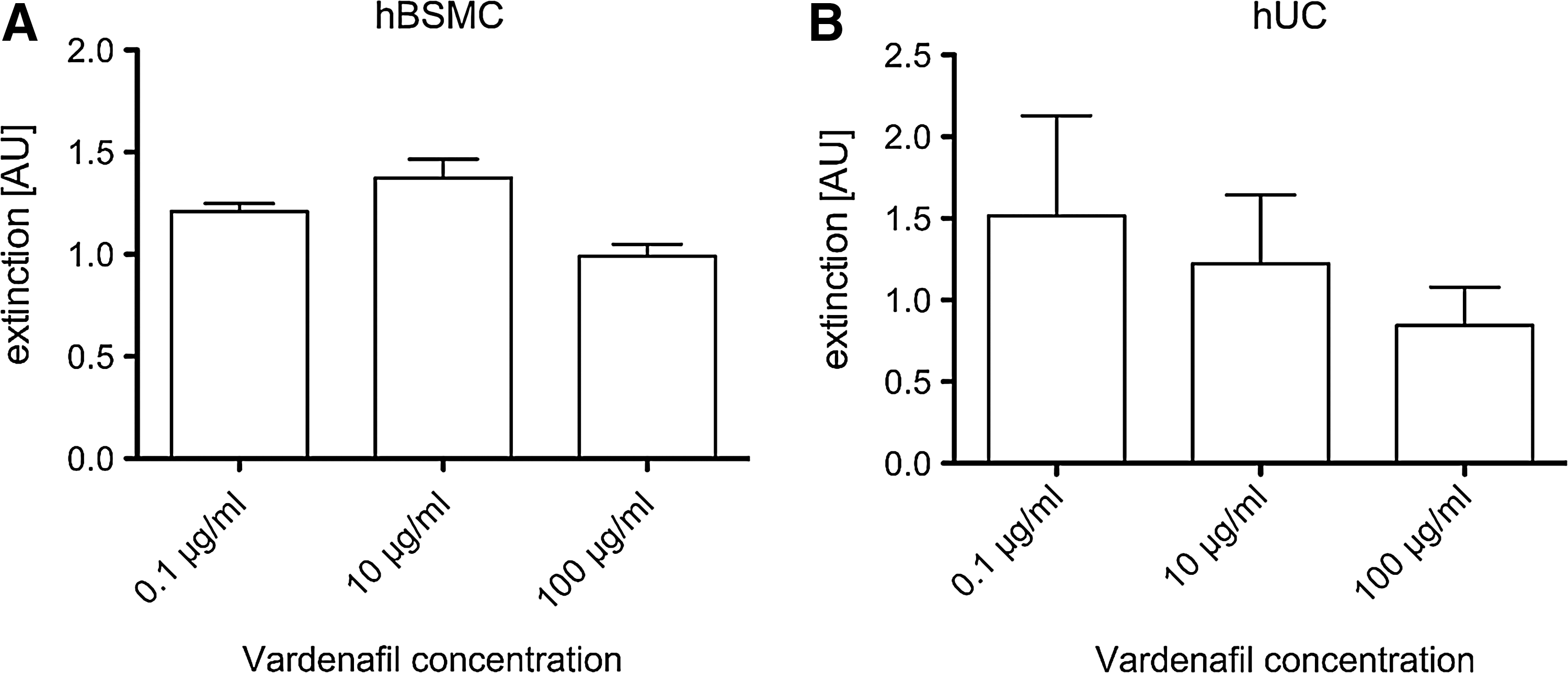
Effect of vardenafil on proliferation/cell viability of cultured human bladder cells.
Discussion
Vardenafil is a PDE-5 inhibitor known for its use in the treatment of erectile dysfunction. Occupation of the catalytic site of PDE-5 by vardenafil inhibits cyclic guanosine monophosphate (cGMP) breakdown leading to an increase of intracellular cGMP. The latter initiates a signal transduction cascade to corpus cavernosum musclulature, which encompasses a decrease in cytosolic Ca+2 inducing smooth muscle relaxation, improving penile erection. 8 Nevertheless, PDE-5 enzymes are not located solely in the penis but are widely distributed in the human tissue, including platelets, vascular smooth muscle, brain, lungs, heart, and kidney. 9,10 Intensive investigation of PDE-5 inhibition in systems other than the reproductive have led to promising results, as demonstrated in the case of pulmonary hypertention, congestive heart failure, diabetic neuropathy, Raynaud phenomenon, digital ischemia, and other clinical entities. 11
The human ureter is considered a direct target of action for vardenafil, given that PDE-5 isoenzymes have been identified in cytosolic supernatants derived from human ureters. 12 Gratzke and associates, 5 in an in vitro investigation, verified that human ureter is responsive to PDE-5 inhibitors, demonstrating that vardenafil, sildenafil, and tadanafil could reverse the tension of isolated human ureteral smooth muscle via cGMP-mediated pathways. Based on the above, in addition to the well-established good safety profile of PDE-5 inhibitors, many investigators have proposed that PDE-5 inhibition can be considered a promising approach for the treatment of patients with ureteral colic. 13 Yet clinical data are still missing, and further investigation is still awaited.
In this work, we confirm that direct vardenafil application induced a dose-dependent relaxation of isolated human ureteral tissue. This effect of vardenafil on the ureter is in accordance with the relaxant properties of PDE-5 inhibitors on the musculature of the rest of the urinary tract as previously documented in various experimental settings. Uckert and colleagues 14,15 have demonstrated that substances regulating cyclic nucleotide-mediated pathways can attenuate norepinephrine-induced contraction in isolated prostatic tissue and can inhibit spontaneous or electrical field stimulation-induced contractile activity of isolated human seminal vesicle tissue. In addition, sildenafil has been shown to induce relaxation on human bladder dome strips via a mechanism involving the H2S, cGMP, cyclic adenosi2ne monophosphate- and K(+) channel-dependent signaling pathways. 16,17
Our results identify vardenafil as a good pharmacologic candidate for local intralumenal administration in clinical conditions in which ureteral dilation might be beneficial. For example, current technology allows coating of ureteral stents with substances exhibiting desirable characteristics. Heparin coated and paclitaxel eluting drug-eluting stents (DESs) are recent examples of such technology. 18 –20 Using this technology, a vardenafil DES could alter stent-related factors contributing to stent-related morbidity, such as flank pain and stent-related discomfort, by reducing ureteral spasm or increased intraureteral pressure over the indwelling stent that are considered main mechanisms of stent-related morbidity. In addition to the above, our study demonstrated an acute initiation of ureteral relaxation after vardenafil application. The latter property of vardenafil renders the substance appealing for use during ureteroscopy or other upper tract retrograde procedures. Direct intralumenal vardenafil instillation could induce an acute ureteral dilation that might assist instrument passage.
It should be emphasized that any substance designated for local use in the ureter (ie, embedded on an ureteral DES) should not stimulate cell proliferation or induce cell apoptosis on ureteral cellular population (urothelium and smooth muscle). Any substance contributing to urothelial proliferation could induce urothelial hyperplasia and thus jeopardize ureteral patency. In contrast, any substance inducing cell apoptosis potentially could have a negative impact on ureteral healing and contribute to ureteral stricture formation. Based on the outcomes of this study, the addition of vardenafil on the ureteral stents may be considered safe and would induce no adverse reaction to the ureter, because no significant effect on the urothelium or ureteral smooth muscle tissue (apart from relaxation) was identified.
Conclusions
Vardenafil induces a dose-dependent relaxation of isolated human ureteral tissue. In addition, direct vardenafil application had no significant effect on growth or cell viability of cultured hBSMC and hUC. Based on the above, this selective PDE inhibitor may be considered a promising pharmacologic agent for local intralumenal administration in clinical conditions in which ureteral dilation might be beneficial.
Footnotes
Acknowledgments
The authors thank Mrs. Annett Weimann and Mrs. Mandy Berndt for their technical support and Prof. Dr. Frank Gaunitz (Dept. of Neurosurgery, University Hospital, Leipzig, Germany) for providing access to the microplate reader.
Disclosure Statement
No competing financial interests exist.