
Abstract
Background and Purpose:
Shockwave lithotripsy (SWL) is a widely used treatment for patients with renal and ureteral stones because of its noninvasive approach. Although minor complications occur in most patients, a relative severe complication, perirenal or subcapsular hematoma, may also occur. We evaluate the possible risk factors for perirenal hematoma after SWL.
Patients and Methods:
Between 2001 and 2011, a total of 10,887 SWL treatments were performed for urolithiasis. All SWL procedures were performed using a Siemens Lithostar multiline lithotripter at a frequency of 2/sec under intermittent fluoroscopic guidance. All these patients underwent outpatient treatment without general anesthesia, but pethidine was administered for pain control. Treatment episodes were retrospectively reviewed for medical history, patient age, sex, body mass index (BMI), mean arterial pressure at induction, location of stone, total number of shockwaves, and peak shockwave intensity. We also compared the hematoma group with the control group (no hematoma formation after SWL with matched age and sex) for various factors.
Results:
After 10,887 treatment episodes on a total of 6177 patients during this period, subcapsular or perirenal hematoma developed in 20 patients for a total incident rate of 0.32%. Eighteen patients had the symptom of flank pain, and 2 patients received a diagnosis accidentally without symptoms. Four patients received a blood transfusion because of low hemoglobulin concentration. All of them received conservative and supportive treatment without surgical exploration. Ten (50%) patients had a history of hypertension. Renal hematoma developed in 11 patients at the second or third SWL treatment. Hypertension, higher BMI, and larger stone size are predisposing risk factors (P=0.022, 0.026 and 0.026, respectively) for renal hematoma.
Conclusions:
Renal hematoma is a rare (incidence rate, 0.32%) but possibly lethal complication. The most common symptoms of renal hematoma are severe flank pain and hematuria. A history of hypertension and higher BMI are important predisposing factors to perirenal hematoma.
Introduction
Tissue injury may come from compressive tensile force, thermal injury, free radical generation, and cavitation of shockwaves. 3 Most self-limited complications, such as hematuria or flank pain, can be treated with supportive care and close observation. Some SWL-related major complications, however, may also happen, including perirenal or subcapsular hematoma, colon injury, and pancreatic trauma. 3,4 In some serious cases, death has also been reported. 5 Although the incidence rate of hematoma is less than 1%, it may increase to 30% when the procedure is followed up with CT or MRI.
To prevent major complications from renal hematoma, discovering the predisposing risk factors of renal hematoma is important. We conducted this retrospective study to evaluate the possible risk factors for renal hematomas after SWL.
Patients and Methods
From January 2001 to December 2011, we retrospectively reviewed the cases of renal or perirenal hematoma that developed after SWL in a medical center in Southern Taiwan. During this period, a total of 10,887 lithotripsies were performed on 6177 patients with the diagnosis of urinary tract stones. All SWL procedures were performed using a Siemens Lithostar multiline lithotripter (Siemens Medical, Munich, Germany) with a focal distance of 12 cm and focal zone of 5×80 mm at a frequency of 2/sec under intermittent fluoroscopic guidance in an outpatient department. Most patients received SWL at an outpatient department. A complete clinical history, physical examination, and image study, such as plain radiography of the urinary tract, intravenous urography, and sonography, were performed before SWL. Pethidine was injected intramuscularly in all patients for pain control.
Renal hematoma was discovered by sonography or abdominal CT (Fig. 1). Among these 10,887 lithotripsies, there were 6177 patients with all diagnostic information available. These patients were then matched to the case group with the same age and sex. Consequently, 146 patients were abstracted without renal hematoma formation as the control group for comparing with the hematoma group. The power calculation of intensity (14.66±0.46 vs 14.9±0.79) was 0.55 with a type I error rate of 0.5.
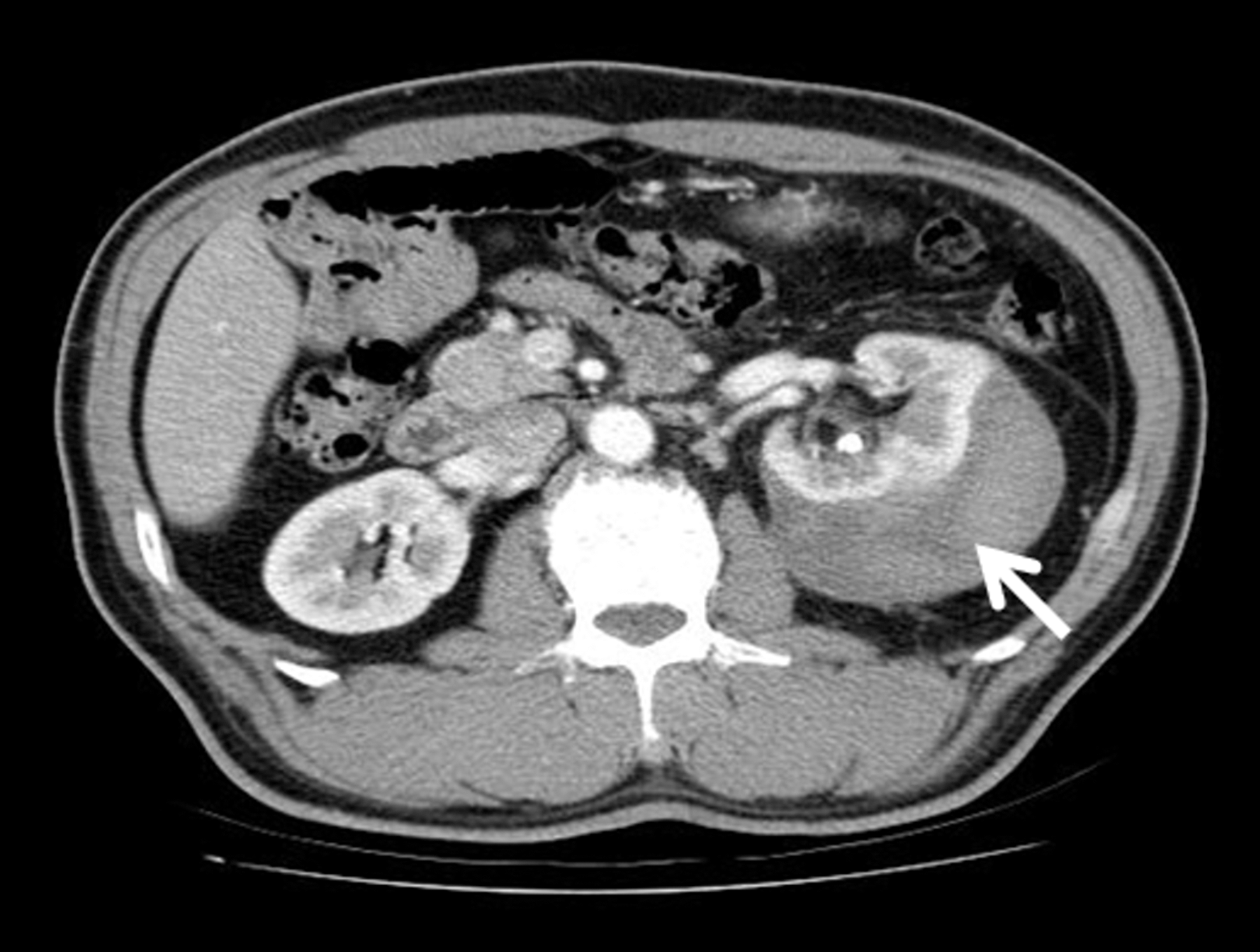
Abdominal CT scan with contrast enhancement showed left renal subcapsular hematoma (arrow).
The following variables were evaluated between the two groups: Age, shockwave intensity (kV), shockwave numbers, body mass index (BMI), maximum axis of stone length, sex, pretreatment arterial blood pressure, and comorbidity. Two sample t test for continuous variables and chi-square test for categorical variables were used. A P<0.05 was considered statistical significant.
Results
Between January 2001 and December 2011, a total of 10,887 lithotripsies were performed on 6177 patients. During this period, a total of 20 cases of SWL-related subcapsular or perirenal hematoma were diagnosed. Among them, 18 (90%) patients were male and two (10%) patients were female. Mean age was 55.65 (±12.6) years. The incidence of SWL-related renal or perirenal hematoma was 0.32%, relative to the number of patients. As shown in Table 1, 18 patients had ipsilateral flank pain and two were asymptomatic. The two cases of asymptomatic hematoma were found by sonography.
BMI=body mass index; Post.=position; Int.=shockwave intensity; Num.=shockwave numbers; Pre-SWL=previous shockwave lithotripsy; HTA=hypertension; BT=blood transfusion; Hosp.=Hospitalization; Med.=medication; R=renal stone; FP=flank pain; U/U=upper ureteral stone.
Eleven (55%) patients in the hematoma group had a history of hypertension and were under medication control at the time of SWL. Both the prothrombin time and activated partial thromboplastin time were evaluated before SWL. Two of the patients were receiving antiplatelet aggregation treatment with aspirin for coronary artery disease. These coagulopathy parameters were all within normal range; antiplatelet aggregation medicine (aspirin) was not suspended in these two patients.
The prevalence of post-SWL hematoma between renal stone cases and ureteral stone cases was similar. A total of 10 (50%) patients had received previous lithotripsy treatments for renal stones. After the development of subcapsular or perirenal hematoma, all 20 patients received conservative treatment consisting of complete bed rest, intravenous fluid supply, follow-up for renal hematoma by sonography or CT if hemodynamically unstable, and checks for vital signs and hemoglobulin levels regularly.
Five (25%) patients had a blood transfusion because of declined hemoglobulin concentration and signs of anemia. No surgical exploration or arterial embolization was performed in any of the 20 patients. The mean length of hospitalization was 6 days. Renal function remained unaffected and no newly diagnosed hypertension occurred after follow-up. All patients were followed at our outpatient department for a minimum of 3 months. The median follow-up period was 5.6 months and the range was 3 to 12 months.
We also abstracted 146 patients without renal hematoma formation as the control group for comparison with the hematoma group. Clinical characteristics of these two matched study groups, separately listed for matched and unmatched variables, are shown in Table 2. There were no statistically significant differences for the variables of shockwave intensity and shockwave numbers (P=0.158 and 0.884, respectively). A comparison of BMI between these two groups revealed a higher BMI in the hematoma group compared with the control group (mean±standard deviation: 26.39±3.54 vs 24.76±2.90, P=0.026, respectively). As for stone length, hematoma group had a larger stone size than the control group (1.35±0.60 vs 1.07±0.52, P=0.026, respectively). In the hematoma group, patients with a history of hypertension had higher hematoma formation percentage (20.4%) than those without hypertension (8%). The association of hypertension and hematoma formation was statistically significant (P=0.022).
Control group: No hematoma formation after shockwave lithotripsy.
SW=shockwave; BMI=body mass index.
Discussion
Although it is well established that potential renal and extrarenal adverse effects can occur as a consequence of SWL, it is generally regarded as the preferred modality for the treatment of patients with urinary tract stones because of its noninvasive nature. The most commonly occurring complication of SWL is flank pain followed by gross hematuria, and urinary tract obstruction from stone fragment migrations. 4 These symptoms often spontaneously resolve in a few days.
SWL-related complications, however, cannot be ignored, because some of these major complications may be lethal. 5 Absolute contraindications for SWL include pregnancy, active urinary tract infection, and uncorrected coagulopathy. 2,3 According to previous studies, symptomatic intrarenal, subcapsular, or perirenal hematomas after SWL are infrequent; less than a 1% incidence rate had been reported by ultrasonography. 6 By using CT or MRI, however, the incidence of renal hematoma may significantly increase up to 30%. 4
The lithotriptor causes stone fragmentation by generating external high-energy amplitudes of pressure through tissue and fluid until encountering stone. Shockwaves act on stones via bubble cavitation, shear, and spelling forces, and finally result in stone disintegration. 7 In addition to stone disintegration, these forces may also lead to the injury of renal vessels or adjacent tissues, particularly in areas of calcification of an atherosclerotic plaque. Therefore, hemorrhagic complications such as hematuria and hematoma frequently follow SWL treatment. 8
Loss of tensile strength of renal vessel walls also increased the incidence of renal hematoma. From this thought, hypertension had been proposed as an important predisposing factor of renal hematoma. 9 In the present results, when compared with results in the control group, hypertension is literally related to the development of hematoma. Other diseases, such as diabetes mellitus, coronary artery disease and obesity, are associated with generalized atherosclerosis with enhanced vascular elastic resistance; these have also been proposed as risk factors. 10 Additional risk factors have been noted to include underlying coagulopathy and use of anticoagulant medications. 11
In the present study, there was no correlation of the shockwaves numbers or intensity. Existing hypertension is the significant risk factor for the development of hematoma. 12 Other variables, such as BMI and stone length, are risk factors that influence the occurrence of renal hematoma. When patients present with higher BMI or larger stone length, the incidence rate of hematoma formation will increase. Inoue and coworkers 8 reported that the outcome of SWL might tend to get worse in proportion to the BMI of the patient.
Our recent study also showed higher quantities of abdominal fat, especially visceral fat, were associated with a lower calculus-free rate after SWL treatment. 13 Obese patients may have skin-to-stone distances that exceed the focal length of the lithotripter and so contribute to more surrounding tissue damage. 14 Another possible explanation is that some coagulation and fibrinolytic proteins (such as tissue plasminogen activator and von Willebrand factor) were significantly increased in patients with metabolic syndrome, indicating atherothrombotic disorders in metabolic syndrome. 15 The exact relationship between BMI and hematoma formation, however, needs further research.
Zhong and associates 16 have shown that shockwave-induced cavitation activity was the main mechanism of tissue damage. Whether larger stone size resulted in asymmetric expansion of the bubbles needs further investigation. Although 50% of patients in our study had undergone one or more SWL procedures, it is hard to identify the direct correlation because of the various times between sessions.
Clinical signs of renal hematoma consist of renal colic pain and gross hematuria. Therefore, severe or uncontrollable flank pain and persistent gross hematuria should alert the physician to a potential hematoma complication. When patients present with these signs, a series of laboratory examinations is needed, and vital signs must be monitored. 17 Imaging investigations, such as ultrasonography, CT, or MRI, can be a useful follow-up tool. CT has been demonstrated to be more sensitive than ultrasonography for detecting hematoma.
Animal studies showed that nephron injury could develop in all kidneys after receiving SWL treatment. 5 Some other studies also showed that acute nephron injury may initiate an inflammation cascade, leading to scar formation and loss of functional renal mas. 18,19 In the long run, however, most of these immediate renal damages resolve over days to months. In the present study, renal function remained unaffected in all of the patients with hematoma.
As previously reported, most symptomatic renal hematomas can be treated with supportive care, such as nonsteroidal anti-inflammatory drugs for pain control, complete bed rest, and close laboratory follow-up. The vast majority of hematomas will self-absorb in time. Blood transfusions are administered when hemodynamic instability and signs of anemia occur. Emergency intervention of renal embolization or nephrectomy may be indicated in the presence of persistent hemodynamic instability after blood resuscitation. 20 Patients rarely died of massive hemorrhage.
For preventing these major SWL complications, careful preparation before the SWL procedure is necessary. Detailed history taking and coagulopathy studies are necessary. In addition, some models predicted that the stress of shockwaves can accumulate within the kidney parenchyma under the shockwaves rate faster than the tissue displacement relaxation time. 21,22 According to the theory, treatment at a slower shockwave rate could decrease the incidence of renal injury but increase the stone breakage efficacy. 21 Stepwise increased shockwave power is another treatment strategy to reduce renal injury. 18
The present study showed that hypertension is an important risk factor for the development of renal hematoma. Therefore, the patient's regularly taking antihypertensive medication to decrease arterial atherosclerosis and carefully monitoring of blood pressure before and after SWL are warranted. On the contrary, many studies showed newly diagnosed diastolic hypertension and diabetes mellitus are also risk factors for renal hematoma. 23,24 The term “Page kidney” means the occurrence of hypertension is caused by mass compressive effects of perinephric or subcapsular hematoma. The possible mechanism is an increase in renin concentration levels in the ipsilateral renal vein. 24 Management of Page kidney lies in conservative treatment with antihypertensive medication; surgery for decompression is reserved only when refractory hypertension occurs. 25 There was no new diagnosis of hypertension in our case series.
Conclusions
SWL is a safe and the preferred modality for the treatment of patients with renal and upper ureteral calculi. No matter how popular it is, SWL-related renal injury was confirmed. For preventing fatal adverse effects, adequate evaluation before treatment is a compulsory task. Regularly controlling hypertension may reduce the possibility of hematoma formation.
Footnotes
Disclosure Statement
No competing financial interests exist.