
Abstract
Background and Purpose:
Benign prostatic hyperplasia is one of the most common conditions in middle-aged and elderly men. The aim of the study was to investigate the treatment effects of low-frequency ultrasound combined with a microbubbles agent on benign prostatic hyperplasia.
Methods:
Eighteen 7-year-old male beagles with prostatic hyperplasia were randomly divided into six groups (n=3): Control group, 21 kHz ultrasound group, 21 kHz ultrasound and microbubble contrast agent group, 1 MHz ultrasound group, 1 MHz ultrasound and microbubble contrast agent group, and microbubble contrast agent group. The histopathologic damage to prostate cells was assessed via transmission electron microscopy and optical microscopy. The protein expressions of prostate-specific antigen (PSA), inducible nitric oxide synthase (iNOS), and super oxidase dimutase (SOD) were detected by enzyme-linked immunosorbent assay. Levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), blood urea nitrogen (BUN), and creatinine (Cr) were detected by the Biochemistry Automatic Analyzer.
Results:
Significant tissue injury, mitochondria injury, and cell apoptosis were observed in 21 kHz ultrasound and the microbubble contrast agent group. Compared with the control and microbubbles contrast agent groups, the decrease in levels of PSA or increase in levels of iNOs and SOD in the other four groups were statistically significant (P<0.05). The lowest level of PSA and the highest levels of iNOs and SOD were observed in the 21 kHz ultrasound and microbubbles contrast agent group. No significant changes in levels of AST, ALT, BUN, and Cr were observed between the six groups.
Conclusions:
Our results suggest that lower frequency ultrasound may have a better effect on benign prostatic hyperplasia, and microbubble contrast agent application further strengthens this biological effect.
Introduction
Transurethral resection of the prostate is the current gold standard for surgical management of BPH, which leads to many complications. 4 In addition, treatment for LUTS/BPH has also involved the use of alpha-1 adrenoceptor antagonists (alpha-blockers) and 5-alpha-reductase inhibitors with satisfactory results. Some patients, however, still do not benefit from these treatments. 5 Thus, exploration of a more effective and safe treatment strategy for patients with BPH has been a constant pursuit of clinical researchers.
Recent studies have indicated that ultrasound is another potential noninvasive approach for treatment of patients with BPH, in addition to its diagnostic value. Traditionally, therapeutic ultrasound has a frequency range of 0.75 to 3 MHz, 6 which offers good tissue penetration and can result in irreversible tissue necrosis at the target region while not damaging surrounding tissues. 7 Further studies suggest that low frequency ultrasound (20 kHz–1 MHz) has a stronger penetration power than high frequency ultrasound and hence deeper tissues can be treated. 8,9
Microbubble ultrasound contrast agent is a widely used contrast medium in ultrasonography, yet it is also found to act as a cavitation nuclei or enhancer. 10 Recently, ultrasound combined with microbubble contrast agent has been suggested to treat a lot of cancers and diseases. 11,12 In combination with a microbubble contrast agent, ultrasound may promote cellular injury, including the initiation of apoptosis and cell injuries through ultrasonic cavitation effects or via other approaches. 13,14 Fewer studies, however, have been reported about the effects of low frequency ultrasound combined with microbubble contrast agent on prostatic hyperplasia.
In the present study, we aimed to investigate the treatment effect of low-frequency ultrasound combined with microbubble agents on prostatic hyperplasia by determining the changes of histologic damage, cell apoptosis, and levels of prostate-specific antigen (PSA), inducible nitric oxide synthase (iNOS), and super oxygen dimutase (SOD) in male beagles.
Methods
Ultrasound system and microbubble
A low-frequency ultrasound machine (21 kHz or 1 MHz, probe diameter 20 mm) was developed by Shanghai Jiaotong University and used to treat patients with prostatic hyperplasia. The Esaote Mylab 90 ultrasound image system (Genoa-Firenze, Italy) equipped with a TRT33 biplane electronic linear transrectal transducer (7 MHz) was used to measure the prostate diameter and volume, and the system equipped with a curved array transducer (3.5–5 MHz) was used to identify the position for displaying the prostate image. A sulfur hexafluoride (SF6)-filled microbubble ultrasound contrast agent (Sonovue®; Bracco SpA, Milan, Italy) was used in this study, which consists of 59 mg of SF6 gas and 25 mg of freeze-dried white powder. After adding 5 mL of 0.9% saline into the vial and shaking for several seconds, phospholipid-stabilized microbubbles filled with SF6 with a diameter of <8 μm (mean, 2.5 μm) were generated at a concentration of (2–5)×108 microbubbles/mL. 15
Animals and grouping
Eighteen 7-year-old male beagles with a diagnosis of hyperplasia nodule in the prostate by ultrasound (Animal Center of Shanghai Jiaotong University, China) were used in this study. All procedures were performed in accordance with guidelines of the Chinese Council on Animal Care. Protocols were approved by the local experimental ethics committee. All animals were anesthetized with 35 mg/kg pentobarbital sodium intravenously and placed on a treatment table in a supine position. After the lower abdomen and suprapubic region were shaved, the penis was retracted laterally to the right to provide clear acoustic access through the abdominal wall to the prostate. Transrectal ultrasonographic imaging and volume measurement (ellipsoid approximation) were performed using the ultrasound imaging system. The low-frequency probe was placed on the lower abdomen skin where the prostate image could be displayed by the 3.5 MHz curved array transducer near the root of the penis.
All animals were randomly divided into six groups (n=3): Control group (without treatment), 21 kHz ultrasound group, 21 kHz ultrasound+intravenous injection of 2 mL microbubble contrast agent group, 1 MHz ultrasound group, the 1 MHz ultrasound+intravenous injection of 2 mL microbubble contrast agent group, and the microbubble contrast agent group.
Ultrasound exposure
The low frequency ultrasound (21 kHz or 1 MHz) probe was positioned in the marked position and the cold acoustic coupling gel was placed between the probe and the skin to prevent reflections and standing waves. The spatial-average temporal average intensity was 318 mW/cm2 for 20 seconds with an 8-second interval and peak acoustic pressure was 0.95 MPa. The duty ratio was 67% (the length of pulse was 20 seconds and the duty of pulse was 30 seconds). The ultrasound exposure was repeated three times every other day, at 30 minutes each time.
Histopathologic analysis
After the treatments, the canines were sacrificed, and prostate tissues were collected to detect the histologic changes by using hematoxylin and eosin (H&E) staining. The JEM1230 transmission electron microscopy (Japan) was used to observe the ultrastructure changes in the prostate tissues.
Terminal deoxynucleotidyl transferase-mediated dUTP nick end-labeling assay (TUNEL)
TUNEL was performed with a TACS® 2 TdT-DAB kit (Trevigen; Gaithersburg, MD) following the manufacturer's instructions. Briefly, after deparaffinization and hydration, sections were digested with proteinase K at a concentration of 20 g/mL for 15 minutes. Endogenous peroxidase activity was quenched with 2% H2O2 for 5 minutes. The slides were immersed in terminal deoxynucleotidyl transferase (TdT) buffer. TdT, 1 mmol/L Mn2+, and biotinylated deoxynucleoside triphosphates in TdT buffer were then added to cover the sections, which were incubated in a humid atmosphere at 37 °C for 60 minutes. The slides were washed with phosphate buffered saline (PBS) and incubated with streptavidin-horseradish peroxidase for 10 minutes. After being rinsed with PBS, the slides were immersed in diaminobenzidine (DAB) solution. All slides were counterstained with 1% methyl green for 3 minutes.
Measurement of biochemical markers
Blood samples (5 mL) were collected from the femoral vein before and after treatment. Levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), blood urea nitrogen (BUN), and creatinine (Cr) were detected by the Biochemistry Automatic Analyzer (Hitachi, Inc., Japan). The expressions of prostate-specific antigen (PSA), inducible nitric oxide synthase (iNOS), and super oxidase dimutase (SOD) were detected by enzyme-linked immunosorbent assay (ELISA) kits (BIOTANG Inc, Waltham, MA) according to the manufacturer's instructions.
Statistical analysis
All the data analysis was performed using the statistical analysis software SPSS 13.0 for windows (SPSS Inc., Chicago, IL). Data are presented as the mean±standard deviation. Significant differences between the groups were analyzed by one-way analysis of variance and differences were considered significant at P<0.05.
Results
Histopathologic examination
Under an optical microscope, neutrophil infiltrations (Fig. 1A) and increased collapsed acinar cells with deeply stained nucleus (Fig. 1B) were observed in the 21 kHz ultrasound group. Only a small amount of eosinophils, eosinophil granules, and red blood cells were accumulated in the capillaries in the 1 MHz ultrasound group (Figs. 1C, D). After combined injection of microbubbles, pathologic injury in the prostate tissue was further increased, especially in the 21 kHz ultrasound+microbubble ultrasound contrast agent group, showing tissue congestion, a large number of neutrophil infiltrations, and eosinophil granules in the capillary lumen (Figs. 1E, F). Microthrombus was formed in the capillaries in the 1 MHz ultrasound group+microbubble ultrasound contrast agent group (Fig. 1G). None of these changes were shown in the control and microbubble ultrasound contrast agent groups.
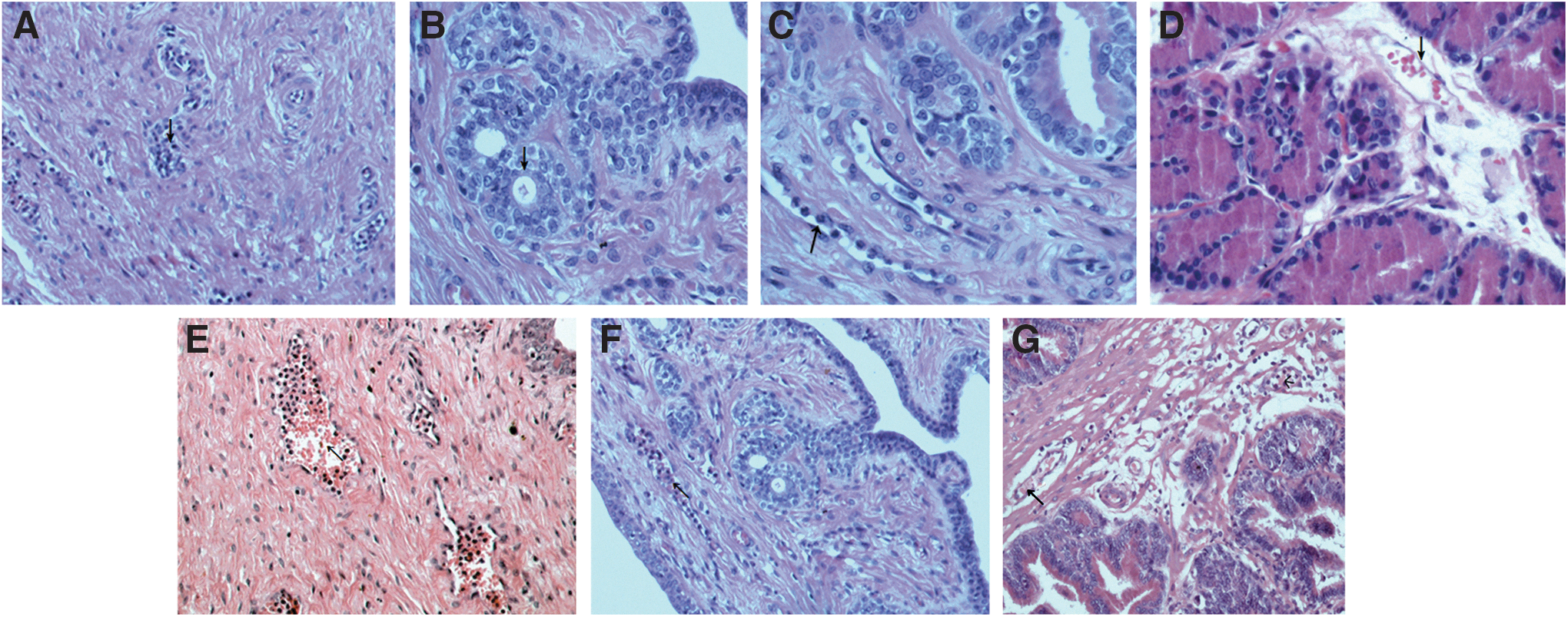
The histologic changes of prostate tissues in canines with different treatments.
Furthermore, ultrastructure changes were displayed under a transmission electron microscope. As expected, no significant change was observed in the control group (Fig. 2A). The 21 kHz ultrasound group, however, showed buckling basement membrane, diminished mitochondria cristae, and mitochondria vacuolation (Figs. 2B, C). Although vacuolated mitochondria were also shown in the 1 MHz ultrasound group (Fig. 2 E), it was less than that in the 21 kHz ultrasound group. The number of vacuolated mitochondria were further increased after ultrasound treatment combined with microbubble contrast agent (Figs. 2D, G). In addition, degranulation of rough endoplasmic reticulum was also observed in the 1 MHz ultrasound and microbubble contrast agent group (Fig. 2F).

Transmission electron microscope observation of prostate tissues in canines after different treatments.
Apoptosis of prostate cells
TUNEL assay was performed to detect apoptosis of prostate cells. In line with the above pathologic changes, no positive cells were detected in the control group (Fig. 3A) and microbubble ultrasound contrast agent group (Fig. 3B). TUNEL positive cells were detected, however, in the the 21 kHz ultrasound group (Fig. 3C), 1 MHz ultrasound group (Fig. 3D), 21 kHz ultrasound with contrast agent group (Fig. 3E), and 1 MHz ultrasound with contrast agent group (Fig. 3F), especially in the 21 kHz ultrasound with contrast agent group.

Terminal deoxynucleotidyl transferase-mediated dUTP nick end-labeling assay was performed to detect apoptosis of prostate cells.
Levels of AST, ALT, BUN, and Cr
Levels of AST, ALT, BUN, and Cr were also measured in the six groups; however, no significant changes were observed between these groups (Table 1).
AST=aspartate aminotransferase; ALT=alanine aminotransferase; BUN=blood urea nitrogen; Cr=creatinine; Sonovue=microbubbles ultrasound contrast agent.
Levels of PSA, iNOS, and SOD
Levels of PSA, iNOS, and SOD were measured by ELISA kits (Table 2). Compared with the control and microbubble ultrasound contrast agent groups, levels of PSA were significantly decreased in the other four groups. The lowest level of PSA was observed in the 21 kHz ultrasound and microbubble ultrasound contrast agent group, which was statistically significant compared with the other five groups (P<0.05). Compared with the control and microbubble ultrasound contrast agent groups, levels of iNOs and SOD were significantly increased in the other four groups (P<0.05), especially in the 21 kHz ultrasound and microbubble ultrasound contrast agent group. Also, the levels of iNOs and SOD were significantly higher in the 21 kHz ultrasound and microbubble ultrasound contrast agent group than those in the 21 kHz ultrasound group, in the 1 MHz ultrasound group, or the 1 MHz ultrasound and microbubble ultrasound contrast agent group (P<0.05).
Compared with the microbubbles ultrasound contrast agent group, P<0.05.
Compared with the 21 kHz ultrasound group, P<0.05.
Compared with the 21 kHz ultrasound combined with microbubbles ultrasound contrast agent group, P<0.05.
Compared with the 1MHz ultrasound group, P<0.05.
Compared with the 1MHz ultrasound combined with microbubbles ultrasound contrast agent group, P<0.05.
Compared with the control group, P<0.05.
PSA=prostate-specific antigen; iNOS=nitric oxide synthase; SOD=super oxygen dimutase; Sonvue=microbbubles ultrasound contrast agent.
Discussion
The application of therapeutic ultrasound in combination with contrast agent is a new concept and has elicited interest in various medical fields. 16,17 As microbubbles are cavitated by the ultrasound, the local shockwaves increase the capillary permeability followed by inducing a serial of pathologic alterations such as thrombosis, microcirculation blockage, prostatic necrosis, and atrophia. 14 Thus, microbubble-mediated ultrasound cavitation may be effective to treat BPH theoretically. 18
In the present study, an in vivo experiment was designed to further confirm our hypothesis. As expected, low-frequency ultrasound in the presence of microbubbles significantly increased the pathologic damages of prostate tissues, such as buckling basement membrane, diminished mitochondria cristae, mitochondria vacuolation, and cell apoptosis, compared with the absence of microbubbles groups. Interestingly, this effect was more obvious in the 21 kHz ultrasound with contrast agent group compared with the 1 MHz ultrasound with contrast agent group. These changes may be explained based on the following reasons: Compared with ultrasound at megahertz frequencies, the pressure level to induce cavitation for kilohertz-frequency ultrasound is relatively low. Low-frequency ultrasound has a stronger penetration power than high-frequency ultrasound and is easily able to rupture the microbubble. Moreover, the energy lose for low frequency ultrasound is low and hence deeper tissue can be treated. 8,9 In addition, our findings also demonstrated that these treatments would not damage the normal function of prostatic tissue, with no significant difference in renal function laboratory data (BUN, Cr, AST, and ALT).
It is reported that oxidative stress is a potential pathogenesis of BPH. 19 The cause of enhanced oxidative stress could be overproduction of free radicals or decrease in the activities of free radical scavenging enzymes such as SOD. 20 These radicals induce apoptosis and necrosis in cells via several targets, such as cell membranes, intracellular bioactive molecules, or DNA and protein. 21 To alter the above peroxidation antioxidant balance may be an underlying mechanism to treat BPH.
In the present study, the SOD was shown to be significantly increased after 21 kHz ultrasound, 21 kHz ultrasound and microbubble ultrasound contrast agent, 1 MHz ultrasound, 1 MHz ultrasound and microbubble ultrasound contrast agent treatment, especially obvious in 21 kHz ultrasound and microbubble ultrasound contrast agent group. Consistently, we also found that low-frequency ultrasonic irradiation with microbubble agent could promote cell apoptosis. This suggests that treatment with low-frequency ultrasound and microbubbles significantly improves BPH.
Recently, increasing evidence indicates that nitric oxide (NO) is involved in modulating the prostatic smooth muscle relaxation, in the control of the urethral outlet activity, and in the nonadrenergic, noncholinergic-mediated cascades that control lower urinary tract storage and emptying.
22
This suggests that an increase in the NO activity and/or its availability may alleviate BPH.
23
–25
Both macrophages and neutrophils are the source of iNOS, which can catalyze NO generation in a reaction where the amino acid
As expected, our results showed that iNOS was significantly increased after ultrasound alone or ultrasound combined with microbubble ultrasound contrast agent. Importantly, the iNOS level was significantly higher in the 21 kHz ultrasound and microbubble ultrasound contrast agent group than that in the 1 MHz ultrasound and microbubble ultrasound contrast agent group, suggesting lower frequency may have better treatment effect.
Furthermore, prostate volume is assessed by baseline serum PSA. 27,28 PSA is present in small quantities in the serum of men with healthy prostates but is often elevated in the presence of prostate cancer or other prostate disorders. 29 Thus, a decrease in PSA level may be a predictor of outcome of treatment of BPH. As expected, the results showed that the lowest level of PSA was observed in the 21 kHz ultrasound combined with microbubble ultrasound contrast agent group, which was statistically significant compared with the other five groups.
Conclusion
The prostate tissues and cells are injured or induced to apoptosis after treatment with low-frequency ultrasound combined with microbubbles contrast agents. Interestingly, the lower the ultrasound frequency is, the better the therapeutic effect. This study may provide experimental evidence for using low-frequency ultrasound combined with microbubbles contrast agents to treat patients with prostatic hyperplasia in the clinic.
Footnotes
Acknowledgments
This study was supported by the National Natural Science Fund (grant No. 81271597) and the Natural Science Foundation of Shanghai (grant No. 10JC1412600).
Disclosure Statement
No competing financial interests exist.