
Abstract
Introduction:
The initial surge of interest in laparoendoscopic single-site (LESS) surgery is balanced by skepticism regarding its future. We sought to evaluate the perspectives of practicing urologists on the role of LESS in urologic training and practice.
Materials and Methods:
An anonymous questionnaire was electronically mailed to members of the Endourological Society and the American Urological Association. Questions were grouped in three domains: training background and LESS experience, perspectives on LESS training, and perspectives on LESS in a current urologic practice.
Results:
Four hundred twenty-two surveys were completed. Respondents had a mean of 11.7 years in practice and 60.7% completed fellowship training. LESS was performed by 44.7% of respondents, however, of these respondents, 75% had only performed <10 LESS cases. For timing of LESS training, 50% believed LESS should be taught during residency and 39% during fellowship. Hands-on workshops and courses were thought to be insufficient by a majority (56%) for learning the LESS techniques before use in practice, and 51% support a credentialing process for urologists performing LESS surgery. Assessing the role of LESS in urologic practice, in its current state, LESS was deemed to provide superior cosmesis (69%) more commonly believed by those with LESS experience 77% versus 63% (p=0.004), however, without yielding a quicker recovery (75%) or less postoperative pain (73%).
Conclusion:
LESS is viewed as an area with potential growth with benefits of superior cosmesis. LESS training should be more integrated into residency and fellowship training and establishing a credentialing process for LESS should be strongly considered by accrediting bodies.
Introduction
There has been a rapid growth of literature on the subject, an exemplifying intense academic interest in this novel approach to minimally invasive surgery. 6 However, the initial surge of interest sparked by the development of LESS surgery has been balanced by a significant degree of skepticism regarding its true benefits given the technical challenges of the approach. We sought to evaluate the perspectives of practicing urologists on the current and future roles of LESS in urologic training and practice.
Methods
Survey design and administration
A survey was designed with questions grouped into three domains: (1) respondent general training background and experience with LESS surgery, (2) perspectives on LESS training, and (3) perspectives on the role of LESS surgery in urologic practice now and in the future (
Data collection
All data were collected through the online survey distributor over a 6-month time period spanning from October 2011 through March 2012. Raw data responses for each question posed were downloaded with no link to the identity of the individual respondents. The data were maintained in a respondent-deidentified, data-encrypted database.
Statistical analyses
The overall dataset combining the responses from the ES and AUA were analyzed for each question in all three domains. Subsequently, subgroup analysis was performed to assess for differences in perspectives held by respondents who reported having experience with LESS techniques versus those who denied prior experience with LESS surgery using the Pearson's chi-square test for binary questions with affirmative and negative responses and the Wilcoxon signed rank test for questions with greater than two response options. All statistical analyses were performed using R v.2.15.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
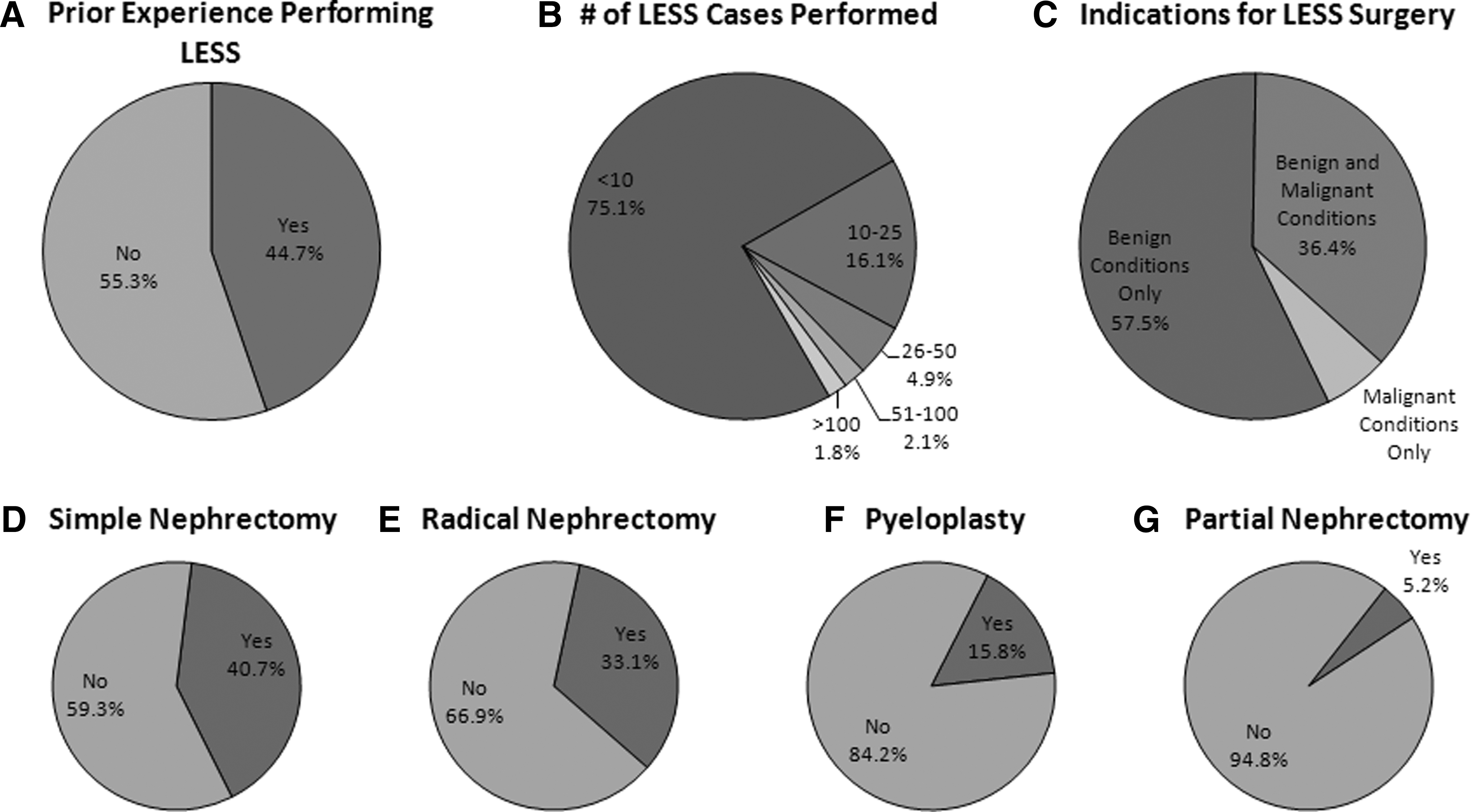
A total of 422 urologists of 5050, who were contacted (8.4%), responded to the electronically administered survey. This consisted of 97 respondents who received the survey via the ES electronic mail list and 325 respondents contacted via the AUA electronic mail list. Professional demographics of the total pool of respondents revealed a mean career length of 11.7±9.4 years (range 0–40) in practice following the completion of training. Fellowship training was completed by 60.7% of all subjects, significantly more common in those reporting experience with LESS surgery (77.8% vs. 37.6%, p<0.0001). Questions assessing experience with LESS demonstrated that 44.7% of respondents had performed LESS procedures in their career. Of these urologists with LESS experience, 75.1% reported performing fewer than 10 cases, and the majority (57.6%) reported employing LESS procedures solely for benign indications (Fig. 1).
Percentage of survey respondents who reported
Inquiry about select renal LESS operations demonstrated simple nephrectomy, radical nephrectomy, pyeloplasty, and partial nephrectomy to be done in order of decreasing proportion among urologists who reported having experience with LESS procedures during their career to date (Fig. 1).
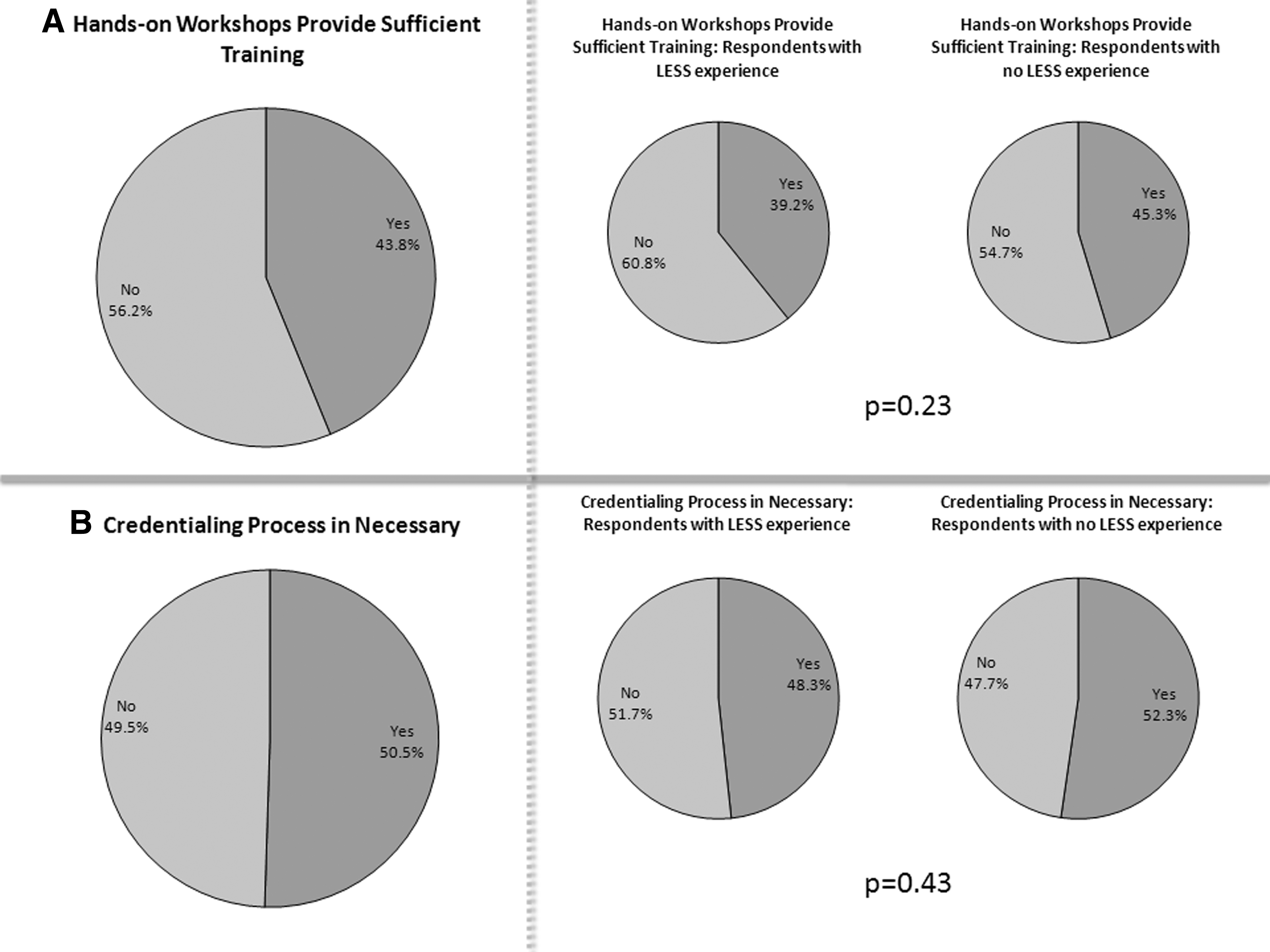
Questions deriving perspectives on the role of LESS in urologic training demonstrated that only 36.4% of respondents for whom it was applicable had their residents or fellows actively participating in LESS cases. In the overall respondent population, 11.5%, 39.0%, 38.8%, and 10.7% believed that LESS should be introduced and taught during Early residency (Uro 1–2), Later residency (Uro 3–5), Fellowship, and After training, during practice periods, respectively. Hands-on workshops and courses were thought to be insufficient by a majority (56.2%) to learn LESS techniques before incorporating these cases into practice, an opinion agreed upon by a majority of respondents in subset analysis irrespective of experience with LESS surgery (p=0.23). Nearly half of the respondents (50.5%) thought there should be a credentialing process for urologists who perform LESS procedures, statistically equivalent in the subset of respondents with LESS experience versus those without (48.3% vs. 52.3%, p=0.43) (Fig. 2). The estimated learning curve to become proficient for reconstructive LESS procedures (i.e., pyeloplasty) was deemed to require experience with more cases compared to ablative/extirpative LESS procedures (i.e., nephrectomy), p<0.0001. Furthermore, this pattern of a longer estimated learning curve for reconstructive procedures was consistent regardless of the survey respondents' experience or lack of experience with these techniques, p=0.0008 and p<0.0001, respectively.
Reported views on the
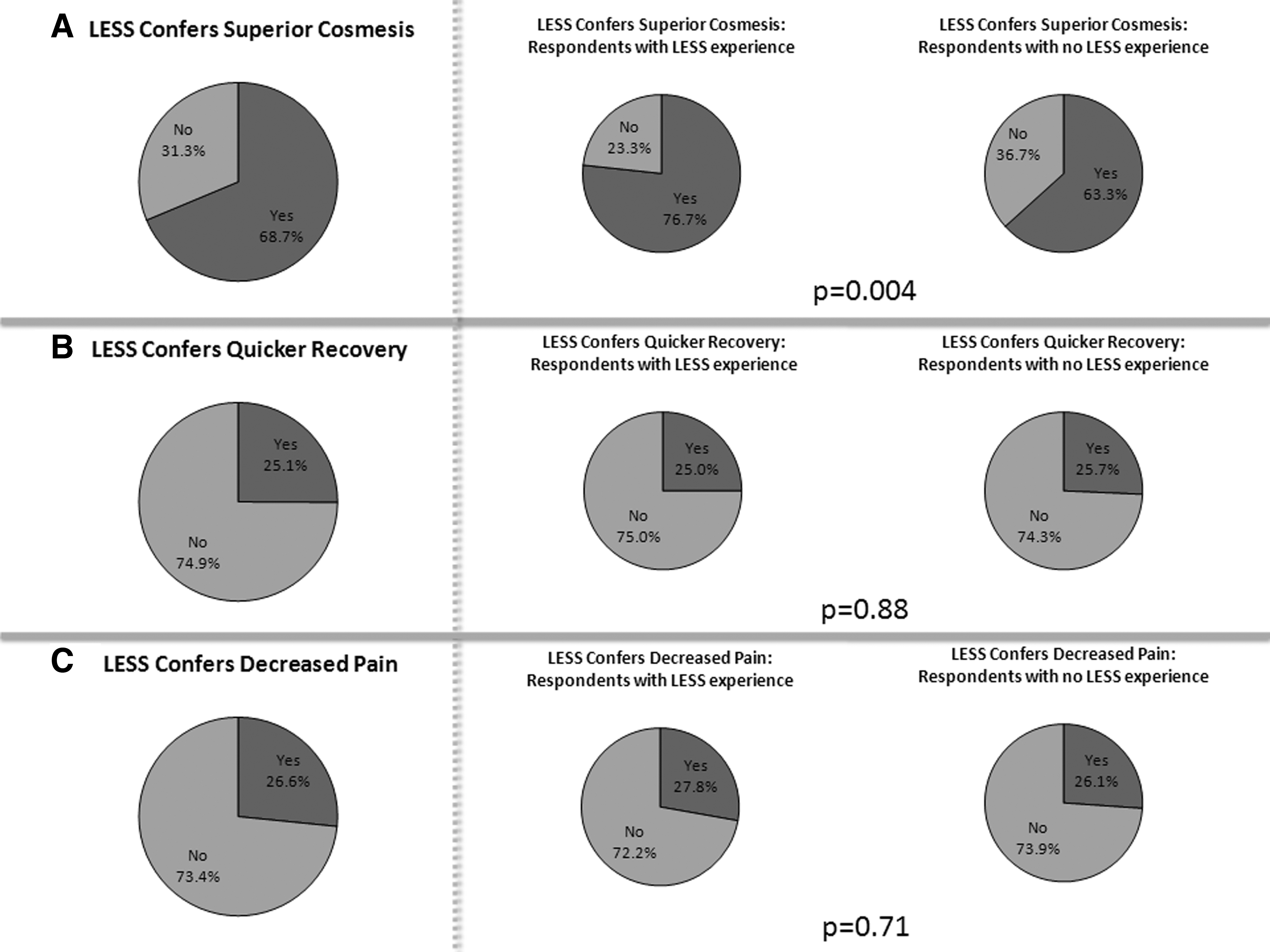
Investigation of perspectives on the role of LESS in urologic practice demonstrated an opinion that the single-site approach, in its current state of use, provided superior cosmesis (68.7%), significantly higher in the cohort of respondents who have experience performing LESS surgery (76.7% vs. 63.3%, p=0.004). However, 74.9% and 73.4% of respondents believed the approach did not yield quicker recovery nor decreased postoperative pain, respectively. These findings were consistent, irrespective of the respondents experience with LESS surgery: p=0.88 and p=0.71, respectively (Fig. 3).
Reported views on the potential benefits of LESS in conferring
Discussion
Historically, the adoption of new surgical techniques requires a stepwise process to progress from a theoretical advance to mainstream practice. The implementation of conventional laparoscopy, for a wide variety of urologic procedures, followed a consistent pattern of investigation as exemplified in the body of published literature. Descriptions of laparoscopic techniques were presented initially as case reports for different procedures. Then, the case–control series demonstrated procedural feasibility, safety, and efficacy. Ultimately, cohort studies and randomized control trials were prospectively designed to validate the value of the new technique compared to the accepted and widely practiced gold standard techniques of open surgery in the era of developing conventional laparoscopy. During this progression, through the evermore rigorous investigation with increasing levels of evidence, laparoscopic techniques were learned, perfected, and implemented in a broader arena of practice, expanding from a few select academic centers to a multitude of practice settings worldwide.
Comparatively, LESS is currently in the adolescence phase of its development and dissemination. Technically oriented case reports of LESS have reported use of the approach for over a dozen unique urologic procedures. These have been supported by numerous retrospective case series and case–control series reporting evidentiary support of LESS as a feasible, safe, and procedure-specific efficacious modification to conventional laparoscopy. 2,7 –9 Most importantly, these publications have demonstrated a dissemination pattern, whereby, LESS techniques have been performed globally and at increasingly more centers. However, investigations demonstrating higher levels of evidence are rare, with only a few randomized control trials performed to date, comparing urologic LESS to conventional laparoscopy. 4,10 Furthermore, the lack of uniformly assessed learning curves and the relative novelty of the approach have not driven the planning of formal, reproducible curricula and consideration of credentialing processes for LESS surgery by any accrediting bodies within urology or other surgical specialties.
Results of this survey demonstrated that nearly 45% of respondents had experience with LESS surgery, but the majority of these individuals had only been involved in less than 10 cases of LESS surgery at the time they took the survey, confirming the relative inexperience with the approach in the larger population of practicing urologists. Furthermore, responses revealed that the majority of urologists reserved LESS for benign indications, and simple extirpative operations were more commonly undertaken than operations requiring reconstruction with intracorporeal suturing, such as pyeloplasty or partial nephrectomy.
Despite the limited experience with LESS by the majority of survey respondents, the majority believed hands-on workshops were insufficient to learn LESS techniques and 89.2% believed LESS techniques should be introduced during formal urologic training, either residency or fellowship. Also, half of survey respondents stated that urologists should have a credentialing process to perform LESS procedures. Given these findings, perhaps, efforts should be made to provide an added exposure to LESS and formally integrate LESS techniques into the curricula urology residencies and endourology/laparoscopy fellowship programs.
The current state of LESS in urologic practice was felt to provide superior cosmesis by 68.7% of respondents, and this was more strongly supported by those urologists who have performed LESS surgery. However, the speed of recovery and improvement in postoperative pain parameters were thought to be unchanged when comparing LESS to conventional laparoscopy, irrespective of respondents' experience with LESS techniques. This suggests that the majority of survey respondents and LESS practitioners are well-informed and aware of the literature, which does not clearly point to such benefits for LESS surgery. A recent review of the public perception of LESS surgery found that patients highlight the importance of a surgeon's reputation, surgical success, and minimizing complications were paramount over measures of postoperative pain and convalescence with cosmetic outcomes given the least importance; cosmesis was deemed most important in younger patients, women, and those undergoing surgery for benign indications. 11 In a study administered before and after surgery, the size and number of scars were deemed more important in a LESS cohort of patients compared to those undergoing laparoscopic and open surgery before surgery, but was no longer found significantly different postoperatively. 12 Additional well-conducted prospective studies, ideally, randomized trials, are necessary to answer these questions regarding the potential clinical values of LESS, maturing the field from its adolescence to a developed technique with a defined role in the field.
Our survey attempted to query urologists who are active members in two large professional organizations within the field. The American Urologic Association survey respondents demonstrated a broad range of practice locations and urologists with a wide range of specialty trainings and lengths of practice experience. The ES population was targeted to ensure an adequate sampling of urologists with practical exposure to and experience with LESS techniques. This group also provided a global population of members. In our final population of respondents, there was a fairly equal representation of those with prior LESS experience and those without likely due to the preemptive attempt to minimize undercoverage bias by targeted specific populations of respondents. Nevertheless, there is an inherent voluntary response bias to this survey, likely over-representing individuals who have strong opinions on the matter of LESS prompting them to respond to this completely voluntary survey with no direct benefit to the respondents surveyed. Also, this is augmented by the nature of electronically administered surveys, which typically have lower response rates as yielded in this study, but allow for higher total number of survey responses given the ease of administration to a large population of potential respondents. 13,14 The limited response rate may not provide a statistically generalizable result for all urologists, but to date represents the best reported assessment of urologists' perspectives on LESS surgery.
Conclusions
LESS is viewed as a technical advance with potential growth with benefits of superior cosmesis. Urologists believe that LESS training should be more formally integrated into urologic residency and applicable fellowship training programs, and establishing a credentialing process for LESS should be strongly considered by accrediting bodies.
Footnotes
Disclosure Statement
No competing financial interests exist.