
Abstract
Purpose:
To assess the use of prognostic factors and models in renal-cell carcinoma (RCC) and to gain insight in the motivations precluding prognosis estimation and the use of prognosticators.
Materials and Methods:
A questionnaire was sent to 110 urologists involved in the Clinical Research Office of the Endourological Society (CROES) Global Renal Mass Study. Frequencies were gathered using descriptive statistics.
Results:
The majority of the 86 responders worked in a university hospital in Europe. Most of the urologists (97.7%) used the tumor-node-metastasis (TNM) classification, and 44% performed prognosis estimations in all patients. The main reason not to estimate prognosis was lack of accuracy (20.9%) and of additional benefit (11.6%). In addition, clinical, laboratory, or pathologic factors were used by 89.5% of the urologists and biomarkers by 16.3%. Preoperative models were used by 20.9%, postoperative models by 38.4%, and metastatic models by 38.4%. The Raj and Motzer models were the most used in preoperative and metastatic settings, while no predominance among the different postoperative models was seen. The most important reasons to skip the use of models were “lack of additional value” and “lack of familiarity” reported by 30.2% and 27.9% of the responders, respectively.
Conclusions:
The TNM is the mainstay for assessing prognosis in RCC. Our data indicate that penetration of prognostic systems is, at most, moderate, suggesting limited use outside original developmental settings. On the contrary, clinical, laboratory, and pathologic factors are used by almost all urologists for prognosis estimations. The most important reason not to use models is the lack of additional value.
Introduction
Besides TNM, other factors that may influence prognosis in RCC have been identified. Clinical factors include symptoms at presentation by opposition to incidental diagnosis and Eastern Cooperative Oncology Group (ECOG) performance status at diagnosis, laboratory parameters such as thrombocytes and hemoglobin level, and pathologic factors such as Fuhrman grade and the presence of tumor necrosis. 4 Moreover, the discovery of the von Hippel-Lindau gene led to the description of several biomarkers that are involved in the pathogenesis of RCC and of possible prognostic significance. 5,6
In attempts to assess prognosis more accurately, prognostic systems and nomograms that combine some of these factors have been developed for different settings in RCC. 4,7,8 In preoperative prognostic models, clinical and radiologic factors are combined. Pathologic and clinical factors are incorporated in postoperative models. Prognostic systems for metastatic RCC incorporate clinical and laboratory variables.
While internal validation is available for most of these models, external validation in different populations than the developmental one is essential before implementation and widespread use of a model or nomogram. 9
Currently, many prognostic integrated systems are available for RCC; however, sound data about their use in clinical practice are lacking.
The primary objective of this study was to evaluate the use of prognostic factors and models in RCC among urologists. The secondary objective was to gather the negative motivations that preclude the use of prognosticators/prognostic models and to identify demographic factors associated with the use of models or biomarkers.
Materials and Methods
Recruitment
A survey was conducted among the principal investigators of active centers that were participating in the Clinical Research Office of the Endourological Society (CROES) Global Renal Mass Study. A personalized questionnaire was distributed by e-mail between February 2011 and March 2012. Forms could be returned by e-mail or fax. Three e-mail waves were sent, and the inclusion closed in May 2012. No approval of the ethical committee was needed for this study.
Questionnaire
To confection the questionnaire, a literature review was performed on prognostic models and factors. MeSH terms “prognosis, risk factor, survival, prognostic factor, model, nomogram, integrated staging system, validation, and calibration plot” were crossed each with “renal-cell carcinoma.” Related key articles' references were meticulously studied. Besides the TNM, other prognostic systems were selected based on introduction of original variables, description in high impact factor journals, presence of validation studies, or high predictive accuracy. The prognostic systems selected for the questionnaire are displayed in Table 1. 10 –23
RCC=renal-cell carcinoma; DFS=disease-free survival; CSS=cancer-specific survival; cT stage=clinical T-stage; UISS=University of California Los Angeles Integrated Staging System; SSIGN=stage, size, grade, and necrosis; OS=overall survival; ECOG=Eastern Cooperative Oncology Group; PS=performance status; TNM=tumor-node-metastasis; VEGFR=vascular endothelial growth factor receptor; VEGF=vascular endothelial growth factor; mRCC=metastatic renal-cell carcinoma; LDH=lactic dehydrogenase.
The questionnaire contained 20 questions (Addendum 1) divided in three sections. The first section (6 questions) explored demographic and global data on prognosis estimation. The second section (7 questions) assessed the use of TNM and other clinical, laboratory, pathologic parameters and markers. Section 3 (7 questions) contained questions on the use of other prognostic models and opinions on their usefulness.
Data for age and years as certified urologists (questions 1, 2) was numeric; questions exploring absolute frequencies (1–5, 7–9, and 14) required a unique response. The rest of the questions were multiple choices, and multiple responses could be chosen but for question 6 that assessed the most important reason “not to estimate prognosis.” Questions 6 and 20 (“usefulness of prognostic models”) had space for free text.
Statistical analysis
The results were analyzed using the descriptive statistics function of Predictive Analytics Software Statistics 18.0.2 (Armonk, NY). Categorical variables were reported as numbers and percentages and continuous variables as median and range (nonparametric distribution).
Associations between demographic data and the use of models or markers were assessed with logistic regression (age, years as urologist) and chi-square tests (number of treated patients, continent, use of markers and models). All tests were performed two-tailed, and a P value of 0.05 was considered statistically significant.
Results
From 110 active centers of the CROES Global Renal Mass Study 86 (78.2%) questionnaires were returned and included in the analyses. All responders were certified urologists (Addendum 2).
Demographic data of the responders are displayed in Table 2. The most important reasons to skip prognostic estimation are illustrated in Figure 1.
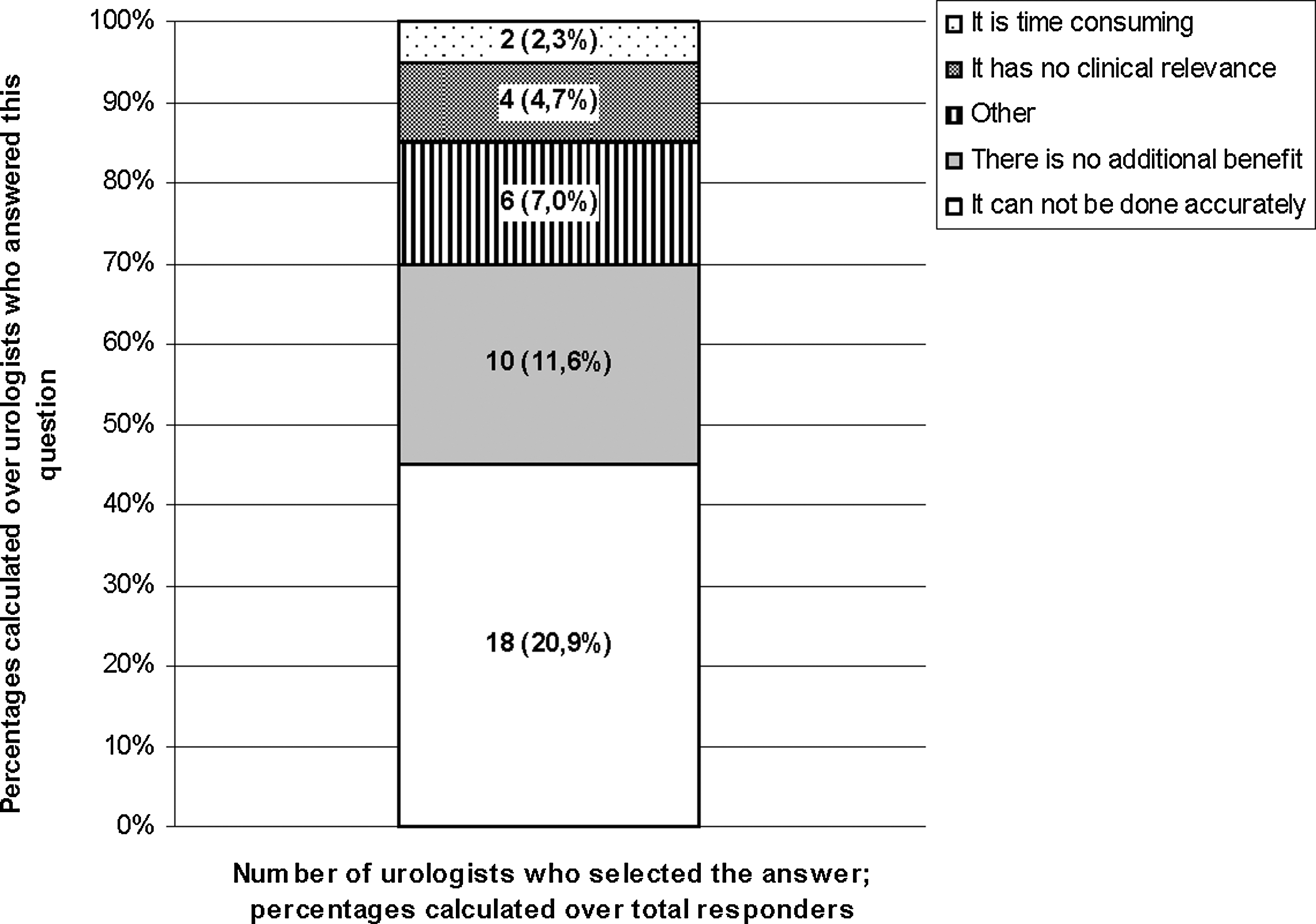
Reasons for urologists to skip prognosis estimation in patients with renal-cell carcinoma question 6). The numbers within the figure correspond to the number of responders who selected the answer, and the percentages are calculated over the total responders. The percentages mentioned on the y-axis are calculated over the number of urologists who answered this question in the survey (n=40). According to the survey, this question was exclusive for those who estimate prognosis.
RCC=renal-cell carcinoma.
Table 3 shows frequencies on the use of TNM staging and other models for prognosis estimation. Overall, 39 (45.3%) responders did not use prognostic models other than the TNM. Motivations not to use other models were: “Too little additional value” and “not being familiar with the model” indicated by 26 (30.2%) and 24 (27.9%) responders, respectively.
Four urologists used two models; one used a model not specified in the questionnaire.
Three urologists used two models and two urologists used three or more models; one used models not specified in the questionnaire.
One urologist used all four specified models.
TNM=tumor-node-metastasis; UISS=University of California Los Angeles Integrated Staging System; SSIGN=stage, size, grade, and necrosis.
From the responders, 51 (59.3%) preferred to use nomograms/models in postoperative and 48 (55.8%) in a metastatic setting as opposed to 31 (36%) in local disease and 27 (31.4%) in a preoperative setting. The usefulness of prognostic models was quoted as: “Dividing patients into risk groups” by 59 (68.6%) responders, “providing patient specific information” by 50 (58.1%), and “select patients for adjuvant therapy” and “tailor follow-up” by 39 (45.3%) responders each.
Additional clinical, laboratory, and pathologic factors were taken into account for prognostic purposes by 77 (89.5%) of the responders. Table 4 shows the frequencies of use for the factors mentioned in our survey. Molecular markers were used by 14 (16.3%) of the responders. Among them, vascular endothelial growth factor receptor was the most frequently used marker by 15.1% of the responders (n=13), 9.3% used p53 (n=8), 5.8% used CAIX and Ki-67 (n=5 each), and 1.2% used vimentin and p21 (n=1 each).
ECOG=Eastern Cooperative Oncology Group.
Table 5 depicts the detailed association between the use of markers and models and demographic factors. No association was found between the use of markers and the use of prognostic systems (P=0.17) and the use of models other than TNM and additional clinical or pathologic parameters (P=0.20).
Discussion
We gathered information on current use of prognostic models and clinical/pathologic factors of possible prognostic value in RCC by approaching a convenience sample, which consisted of principal investigators of the prospective CROES Global Renal Mass Study (2010–2012), a contemporary registry on patterns of treatment of renal tumors. 24 In this way, we aimed to ensure that the sample represented the target population: Urologists who were treating patients with RCC and familiar with prognostic models and factors related to the condition. In our sample, the use of models or markers was not related to any demographic data concerning age of the responder and years or type of practice.
Prognostic estimation and the use of prognostic models
Our survey shows that the TNM classification is universally used in RCC. Furthermore, 44% and 24.5% of the urologists estimate prognosis in all and most of the RCC cases, respectively. These data confirm the excellent penetration of the TNM classification whether as a clinical tool in treatment decisions 2,3 or as predictor system. The pathologic TNM is not only a powerful predictor for cancer-specific survival with accuracy of 85% 25 and may drive the opportunity for adjuvant survival management in the future, 25,26 but it is also helpful in designing follow-up schemes. Besides general acquaintance with the TNM classification, as oldest in use, present results support its “friendly use” and generality. 27
There is a discrepancy, however, between the rate of responders that acknowledge estimating prognosis and the figures on the use of the TNM. The prognostic value of the TNM seems to be somehow underestimated or forgotten because less than half of the responders estimate prognosis in all cases. Although this figure is upgraded to 69% when including those that estimate prognosis in most of the cases, still one-third of the responders might consider the TNM as a mere classification and associate prognosis estimation with the use of prognostic systems other than the TNM.
Preoperative prognostic systems using only clinical and radiologic factors were marginally used by our responders. Usefulness of preoperative models is a matter of debate. Preoperative determination of recurrence risk or survival is not likely to influence the treatment decision that mainly depends on clinical TNM stage and patient characteristics. 2,3 Moreover, prognosis estimations with postoperative data are equally or more accurate than preoperative estimation. 10 –13 Nevertheless, in the current interventional scenario, a certain number of patients with small renal masses who are treated by ablation or surveyed may still benefit from the use of these preoperative models because definitive pathology, based on surgical specimen, will not be available to properly stage tumors. 11
Our survey indicates a moderate penetration of postoperative models, although there was no clear preference for any model. Survival outcomes, patient population, and performance, mostly expressed as concordance-indexes, (c-indexes) among these models and their external validation studies differ widely in the literature. 14 –17 The c-index of the 2002 TNM ranges from 0.746 t0.848 for the T-stage. 13,18,25 Currently, only a few models have shown a higher c-index in settings other than their developmental one. 28 Furthermore, validation has either failed or is not available for some. On internal validation, an accuracy of 1.0, meaning perfect prediction, is never expected. To provide incremental value to the TNM classification, however, the existing models should approach an accuracy of 0.9 on external validation, which none currently do. 8
Use of prognostic models in metastatic RCC
The use of prognostic models in a metastatic setting was moderate (38.4%). The professional profile of the sample, exclusively urologists, may be the explanation. Although the number of cases of metastatic RCC seen by individual/year was not recorded, it might be relatively low and likely a survey focusing on oncologists would have shown different results. The figure presented here may be discussed under two different perspectives. For those countries where uro-oncologists are entitled to medically treat patients with metastatic RCC, this figure is a pessimistic one, because risk prognostic assessment in metastatic RCC is of outmost importance to determine treatment. Conversely, for those countries where metastatic RCC is directly under supervision of onco-urologic specialists, the figure shows a nonnegligible interest of urologists in metastatic RCC prognostic estimation. The authors consider that country-based surveys on this specific point would provide a better answer.
As expected, the Motzer model was by far the most frequently used in the metastatic setting. 20 The accuracy of this model ranges from 52% to 73% including some reports on vascular endothelial growth factor targeted therapy. 8 The Choueiri model 22 for which no internal or external c-indexes are provided, was much lesser used.
Use of additional factors
Almost 90% of the urologists indicated that they take into account clinical, laboratory, and pathologic parameters when estimating prognosis. Approximately 80% of the urologists used several of these factors, and more than half also used three or more different factors of one category. Although the use of additional factors did not correlate with the use of prognostic systems other than the TNM, these data indicate a strong awareness of the urologic community on the possible prognostic impact of symptoms, histologic subtype, and nuclear grade.
Although some studies reported Fuhrman grade, symptomatic presentation, ECOG performance status, or age as independent predictors for survival, other factors such as subtype, hemoglobin and thrombocytes level still show conflicting results. 4 In spite of their frequent use, no uniform interpretation for risk of death or disease-free survival (DFS) exists for these factors.
A small percentage of urologists indicated that they use markers for prognostic purposes. Their use as an integrated model was negligible. It is worth mentioning that recently a model integrating biomarkers has shown a high additional predictive value (c-index 0.904) for DFS in localized RCC. 18 Besides the fact that most of the biomarkers models are of recent publication, the absence of consistent results on the value of individual markers as well as cost issues limit their current use as prognostic tools. 29 Although the subject is the object of sharp research, a longer period is necessary to assess the true impact of such models. Their generality will ultimately depend on their additional value when combined with other prognostic systems in use and their availability.
Reasons to skip prognostic estimation
The main reason to preclude prognosis estimation reported by half of the responders to this question was the lack of accuracy of the different prognostic systems/factors. Other reasons in decreasing order were lack of additional benefit, absence of clinical relevance, and being time consuming.
These opinions reflect the well-known concerns on the external performance of prognostic systems 27,29 and open the door for a critical assessment on the developmental methodology of prognostic systems in cancer, on their usefulness in the current treatment practice in RCC, and on their functionality.
In response to the more specific question on the reason for not using models other than TNM, again the most important reason was lack of additional value, and one-third of the urologists indicated that lack of familiarity with models was the reason not to use them. Seeing that the questionnaire was spread among research minded urologists, the actual number of urologists who are not familiar with prognostic systems will likely be higher.
Limitations
The limitations of our study include: Models selection, population sample, and geographic distribution of the responders.
Not all the models described in the literature were included in our survey. Inclusion of all reported models would have lengthened the questionnaire and most likely decreased the response rate, which was higher than expected in this kind of survey.
The convenience sample was dictated by the focused practice. In fact, it is impossible to assess the potential population, because no data are available on the total number of uro-oncologists and most specifically those dedicated to RCC. Although this figure is expected to be very high, a power calculation shows that the high response rate of our survey provided the sample with a 95% of confidence (±10% of variability) and thus could be considered representative.
The use of a convenience sample precludes extrapolation on the use of models and markers among general urologists not involved in oncology. The figures presented here might be even lower should general urologists have been surveyed. This is a further point of concern when considering the usefulness of more complex predictive models than the TNM.
With respect to the geographic distribution, because 70% of the responders belonged to European countries, we cannot ensure that the results can be extrapolated to other continents. There were no apparent differences in response results between European and American urologists, but the American sample was scarce.
Conclusions
The TNM staging system is universally used, although only 40% of the urologists acknowledge using prognostic assessment in RCC. Preoperative prognostic models are scarcely used and postoperative models are only moderately used. There is no clear preference for any of the postoperative models. The main reasons that hinder the use of prognostic models other than the TNM are lack of accuracy, absence of additional benefit, and lack of familiarity. In the metastatic setting, the Motzer model is the most frequently used. Clinical, laboratory, and pathologic factors are being used by almost all urologists. Our data indicate that the penetration of the recently described staging models and integrated systems is, at most, moderate, suggesting a limited use outside of the original developmental settings.
Footnotes
Acknowledgments
The authors thank the Clinical Research Office of the Endourological Society for providing the sample addresses. This study was funded by an unrestricted research grant from the Cure for Cancer Foundation.
Disclosure Statement
Dr. Jean de la Rosette is consultant for BSC. For the remaining authors, no competing financial interests exist.
Abbreviations Used
Survey on the Use of Prognostic Models in RCC
Age in years: ___________
Answer in years: ___________
□ University hospital
□ Community hospital
□ Community hospital (individual practice)
□ Less than 50
□ Between 50 and 100
□ More than 100
□ In none of the patients
□ In some patients
□ In half of the patients
□ In most patients
□ In all patients Continue to question
□ There is no additional benefit to the treatment
□ It has no clinical relevance
□ It can not be done accurately
□ It is time consuming
□ Other (please specify):
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
____________________________________________________________________________
□ Yes
□ No
□ Yes
□ No Continue to question
□ ECOG performance status
□ Karnofsky performance status
□ Symptoms at presentation
□ Age
□ Race
□ Haemoglobin
□ Erythrocyte sedimentation rate
□ Calcium
□ Thrombocytes
□ C- reactive protein
□ Subtype RCC
□ Fuhrman nuclear grade (including sarcomatoid differentiation)
□ Necrosis
□ Sinusal ingrowth
□ Vascular ingrowth
□ Yes
□ No Continue to question
□ CAIX □ PTEN
□ p53 □ Vimentin
□ p21(nuclear) □ B7-H1
□ VEGF/VEGF receptors □ Ki-67
□ Yes
□ No Continue to question
□ Cindolo preoperative prognostic model
□ Raj (MAYO/MSKCC) preoperative nomogram
□ Karakiewicz preoperative prognostic model
□ Yaycioglu prognostic model
□ I do not use preoperative models
□ Kattan postoperative nomogram
□ UCLA integrated Staging System
□ SSIGN (MAYO)
□ Karakiewicz postoperative nomogram
□ Klatte postoperative nomogram
□ Kim prognostic model (2004)
□ I do not use postoperative models
□ Motzer (MSKCC) prognostic classification
□ Heng prognostic model
□ Choueiri prognostic model
□ Kim prognostic model for mRCC (2005)
□ No metastatic RCC models
After this question, please continue to question
□ Too little additional value
□ Too complicated
□ No clinical relevance
□ Too expensive
□ Techniques not available in hospital
□ Not familiar with models
□ Preoperatively
□ Postoperatively
□ In local disease
□ In metastatic disease
□ To select patients for adjuvant therapy
□ To tailor follow up
□ To divide patients into risk groups
□ To provide patient specific information
□ Other (please specify):
_________________________________________________________________________________________________________
_________________________________________________________________________________________________________
________________________________________________________________________________________________
Appendix
J. Amon, Hosptital Universitario Rio Hortega, Valladolid, Spain
M. Aron, University of South California, Institute of Urology, Los Angeles, USA
M. Alvarez-Maestro, Hospital Infanta Sofia, Madrid, Spain
Y. Aslan, Numune Research and Training Hospital, Ankara, Turkey
R. Autorino, Cleveland Clinic, Cleveland, USA
S. Bariol, VMO at Westmead and Blacktown Hospital, Sydney, Australia
E. Barret, Institut Montsouris/Université Paris Descartes, Paris, France
B. Baseskioglu, Eskisehir Osmangazi University Medical Faculty, Eskisehir, Turkey
J. Bernhard, Bordeaux University Hospital, Bordeaux, France
I. Billiet, Groeninge Hospital, Kortrijk, Belgium
D. Bolton, University of Melbourne, Melbourne, Australia
A. Bouzourita, Charles Nicolle Hospital, Tunis, Tunisia
A. Breda, San Bassano Hospital, Bassano del Grappa, Italy
V. Bucuras, Timisoara Clinical Emergency Hospital, Timisoara, Romania
J. Cadeddu, University of Texas Southwestern Medical Center, Dallas USA
L. Campos-Pinheiro, Hospital Curry Cabral, Lisbon, Portugal
F. Coz, Hospital Militar de Santiago, Santiago, Chile
A. Crisci, University of Florence, Florence, Italy
G. Delia, Ospedale San Giovanni, Rome, Italy
S. Eggener, University of Chicago Medical Center, Chicago, USA
T. Erdogru, Akdeniz University Hospital, Antalya, Turkey
T. Frede, Helios Kliniken, Berlin, Germany
L. Fossion, Maxima Medisch Centrum, Eindhoven, the Netherlands
P. Gontero, Molinette Hospital, Turin, Italy
G. Gopalakrishnan, Vedanayagam Hospital & Postgraduate Institute, Coimbatore, India
S. Gravas, University Hospital of Larissa, Larissa, Greece
G. Gueglio, Hospital Italiano, Buenos Aires, Argentina
S. Guven, Selcuk University Meram Medical School, Konya, Turkey
C. Hernandez, Hospital Gregorio Marañón, Madrid, Spain
M. Hora, University Hospital Plzen, Plzen, Czech Republic
S. Jackman, University of Pittsburgh Medical Center, Pittsburgh, USA
A. Joyce, St.James University Hospital, Leeds, United Kingdom
H. Kim, Denver Medical Center, Denver, USA
R. Kockelbergh, University hospital Leichester, Leichester, UK
T. Knoll, Klinikum Sindelfingen, Sindelfingen, Germany
J. Kums, Isala Klinieken, Zwolle, The Netherlands
A. Kural, Istanbul Bilim University School of Medicine, Istanbul, Turkey
P. Laguna, Academic Medical Center, Amsterdam, the Netherlands
C. Lallas, Jefferson University Hospital, Philadelphia, USA
E. Lechevallier, Hôpital de la Conception, Marseille, France
B. Lee, Tulane University School of Medicine, New Orleans, USA
E. Liatsikos, University of Patras, Rio-Patras, Greece
C. Luigi, Univerity of Foggia, Foggia, Italy
T. Mendonca, Centro Hospitalar de Lisboa, Lisboa, Portugal
C. Mochtar, Cipto Mangunkusumo Hospital, Jakarta, Indonesia
P. Modi, Institute of Kidney Disease and Research Centre, Civil Hospital, Ahmedabad, India
J. van Moorselaar, Vrije Universiteit Medisch Centrum, Amsterdam, the Netherlands
K. Mteta, Kilimanjaro Christian Medical University College, Moshi, Tanzania
V. Murthy, Nizam's Institute of Medical Sciences, Hyderabad, India
S. Naito, Kyushu University, Fukuoka, Japan
P. Olbert, University Medical Center, Marburg, Germany
Y. Ozgok, Gulhane Military Medical Academy, Ankara, Turkey
D. Pacik, Masaryk Municipal Hospital, Jilemnice, Czech Republic
S. Pahernik, Heidelberg University Hospital, Heidelberg, Germany
J. Palou, Fundacio Puigvert, Barcelona, Spain
R. Pelger, Leiden University Medical Center, Leiden, the Netherlands
T. Polascik, Duke University, Durnham, USA
H. van Poppel, University Hospital Leuven, Leuven, Belgium
F. Porpiglia, San Luigi Gonzaga Hospital, Turin, Italy
D. Prokar, Guy's Hospital, London, United Kingdom
D. Rabah, King Saud University, Riyadh, Saudi Arabia
J. Rassweiler, SLK-Klinikum am Gesundbrunnen, Heilbronn, Germany
L. Rioja, Hospital Universitario Miguel Servet, Zaragoza, Spain
L. Salamon, CHU Henri Mondor, Paris, France
J. Sanchez Zalabardo, Hospital Clínico "Lozano Blesa", Zaragoza, Spain
J. Santos-Dias, Hospital da Luz, Sao Paulo, Brasil
N. Shakhssalim, Shahid Beheshti University of Medical Sciences, Tehran, Iran
W. Shingleton, Ochsner Clinic, New Orleans, USA
V. Singh, Postgraduate Institute of Medical Education & Research, Chandigarh, India
M. de Sio, Second University Hospital, Naples, Italy
A. Skolarikos, Sismanoglio Hospital, Athens, Greece
P. Sountoulidis, General Hospital Of Veria, Veria, Greece
S. Subotic, Urologische Klinik Universitätsspital Basel, Switzerland
A. Tefekli, Medical Faculty of Istanbul, University of Istanbul, Istanbul, Turkey
L. Tuncay, Pamukkale University, Denizli, Turkey
C. Acar, Pamukkale University, Denizli, Turkey
K. Tupikowsky, Wroclaw Medical University, Wroclaw, Poland
L. Turkeri, Marmara University Hospital, Istanbul, Turkey
B. Turna, EGE university hospital, Izmir, Turkey
T. Tuytten, Academisch Centrum Maastricht, Maastricht, the Netherlands
A. Unsal, Kecioren Hospital, Ankara, Turkey
G. Verhoest, Rennes University Hospital, Rennes, France
J. Viorel, Prof.Dr.Th.Burghele Hospital, Bucharest, Romania
S. Wolf, University of Michigan Health System, Ann Arbor, USA
U. Yildirim, Istanbul Goztepe Training Hospital, Istanbul, Turkey
R. Zdrojowy, Akademia Medyczna Wroclaw, Poland