
Abstract

Our patient was a woman who was treated by chemo- and radiotherapy after radical hysterectomy. She had a right ureteral obstruction that had been palliatively managed with Double-J stent exchange every 6 months for the last 3 years. She was referred to our clinic with persistant gross hematuria after the latest, reportedly uneventful cystoscopic placement of a 4.8F Double-J stent. Radiography of the kidneys, ureters, and bladder showed the stent was positioned along the ureteral path distally, but coursed somewhat medially above the lumbosacral level, and the proximal loop was noted to be medially rotated and well over the level of the renal pelvis (Fig. 1). A CT revealed that the stent was in the correct position distally but coursed inside the iliac vein and then within the inferior vena cava (IVC) up to the level of hepatic veins (Figs. 2–5). Immediate cystoscopy was performed to prevent further migration into the vessel, and the stent was successfully removed by grasping forceps. Clear blood coming from the right ureteral orifice lasted a short time as observed under direct vision (Figs. 6, 7). The gross hematuria ceased, and the hemoglobin level was stable after this intervention.

Radiography of the kidneys, ureters, and bladder shows medially displaced Double-J stent.

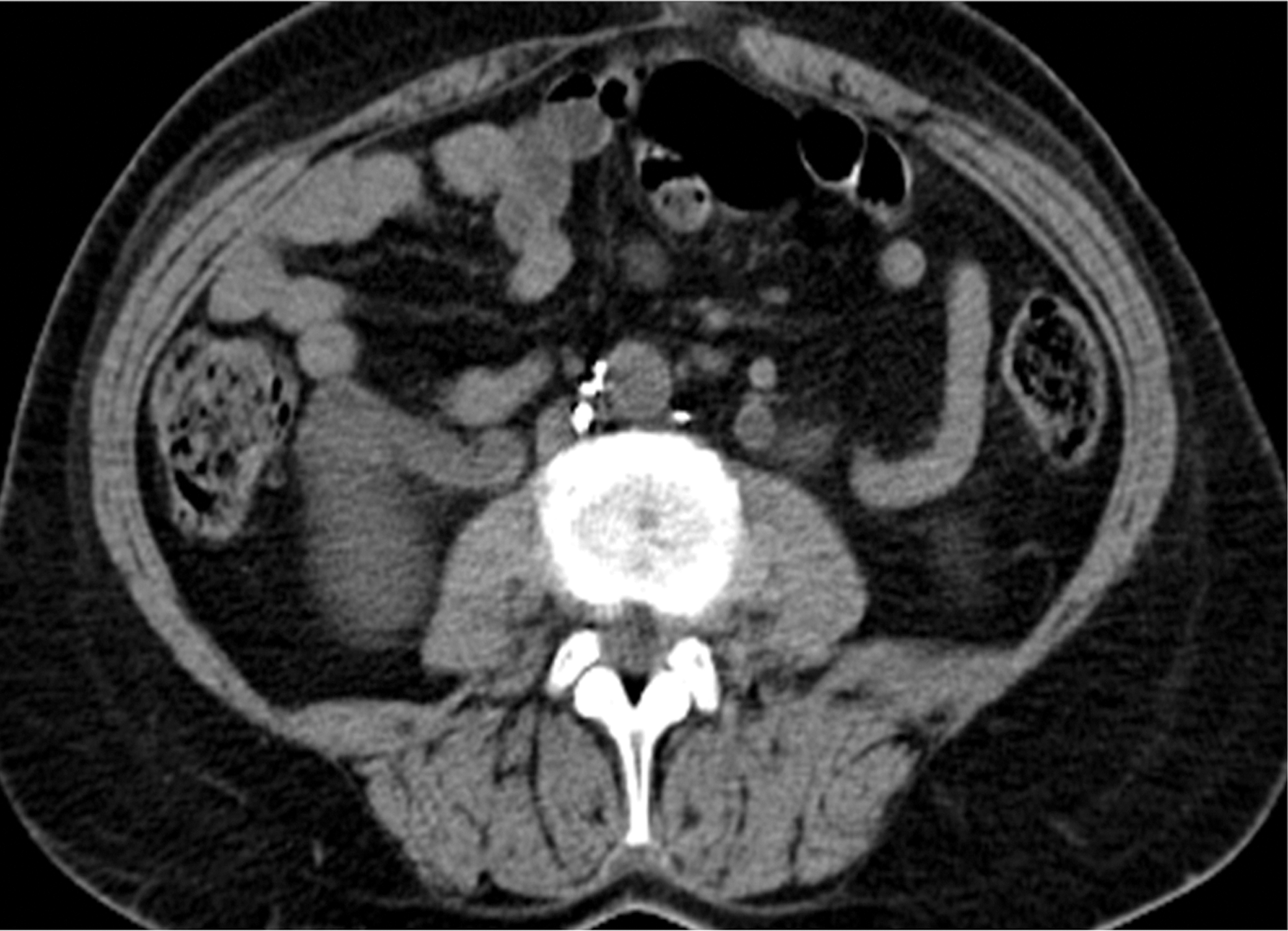
CT scans showing the stent in the correct position distally, but then coursing inside the iliac vein and the inferior vena cava.


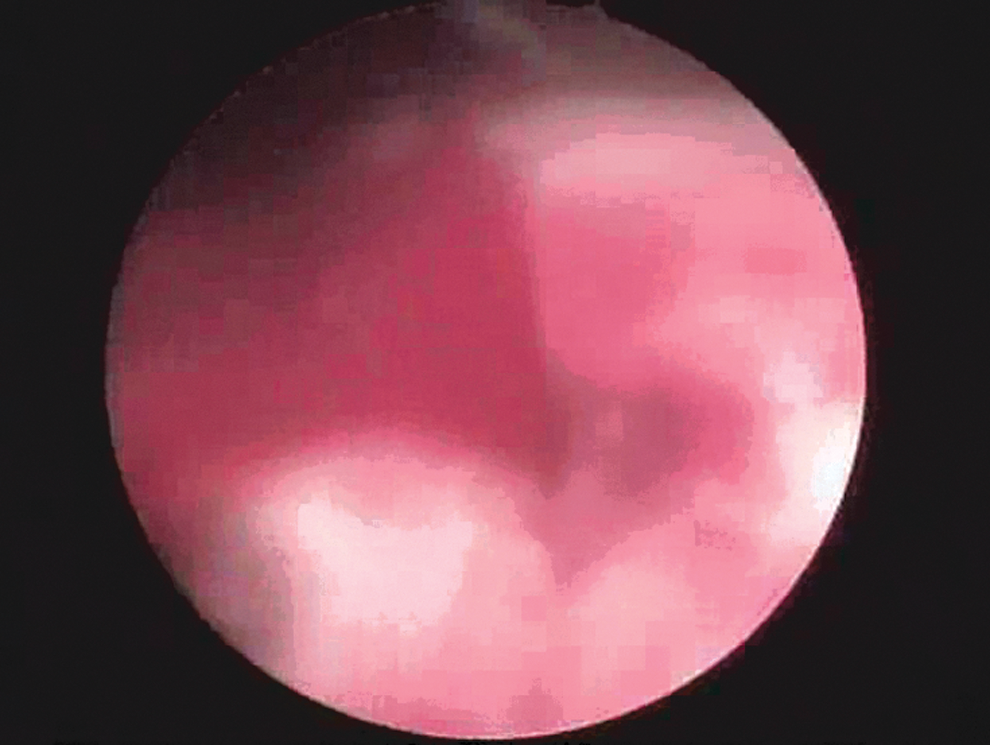
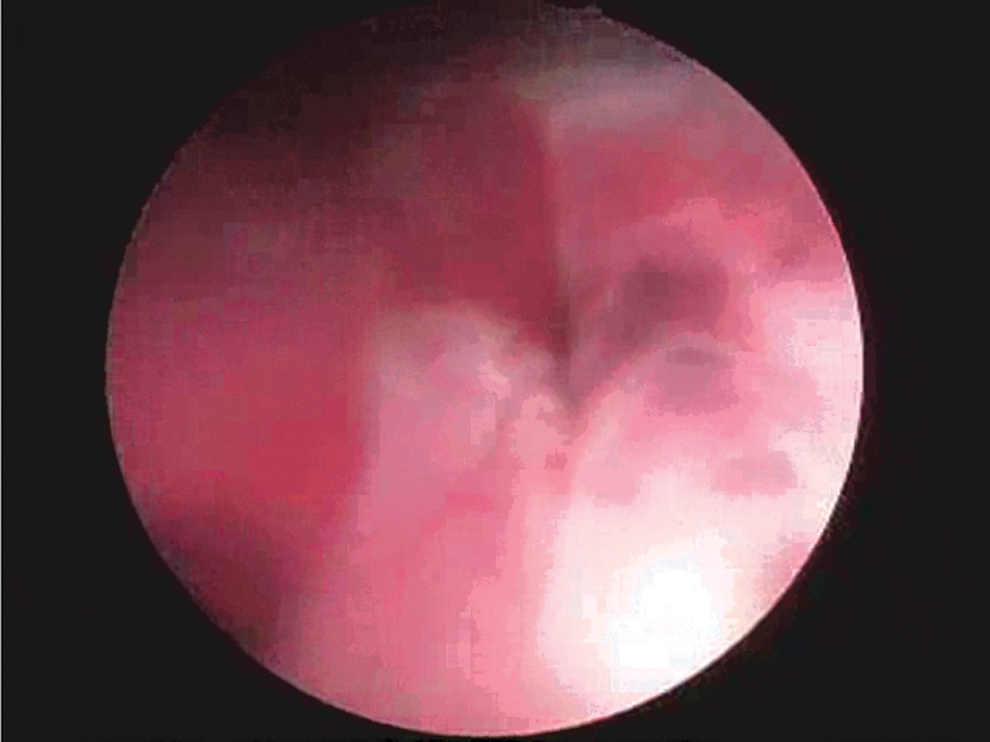
Cystoscopic snapshots of blood oozing from the right ureteral orifice just after the stent was removed.
It is possible for stents to be misplaced, dislodged, or occluded, particularly when dealing with severe strictures or obstructions of the ureter. Ureteral strictures that ensue radical hysterectomy are typically complicated cases in which there is tortuous hydroureteronephrosis and the mucosa is highly friable, and ischemic. 2 The ureter is fixed by fibrosis, and the stricture is usually not amenable to treatment by dilation. A long-indwelling Double-J stent generally fails to prevent or treat the stenosis in such cases. Therefore, exchanging a stent may not necessarily be a simple intervention. Passing a stent through a tight stenosis in a fixed, curved ureter nearby the iliac crossing, which is the common site of a posthysterectomy stricture, is a designated endourologic challenge. Access can be made easier by preferring to use hydrophilic-coated wires and “preformed tip”angiographic catheters to negotiate the angulations and tortuosities of the obstructed ureter. The edema and excessive friability of the mucosa involve a risk of bleeding and false passages after multiple attempts. In our case, bearing a Double-J stent for a long time apparently did not dilate the ureter sufficienty to allow an easy exchange of the stent. The weakened ureteral wall must have been perforated by the guidewire at the usual site of the posthysterectomy stricture where the ureter courses obliquely, medially, and anteriorly out of the bony pelvis. The use of fluoroscopy is essential in such potentially complicated cases. Furthermore, inability to advance the guidewire or the ureteral stent may obligate ureteroscopic visualization of the opening and passage of the guidewire safely and less traumatically.
Contrary to the other cases, we undertook a transurethral endoscopic approach for removal of the dislodged stent in the IVC. Falahatkar and coworkers placed the Double-J stent cystoscopically but then found it to be located entirely within the venous vascular system. Therefore, it was justified to remove the migrated stent percutaneously through the femoral vein. In the other case by Tang, the stent was inserted via percutaneous nephrostomy, and a part of it was still inside the renal pelvis. The authors opted to use the percutaneous angiographic route for extraction, arguing that it is a less invasive and safer method. On the other hand, we experienced that, as long as a part of the migrated stent is readily accessible endourologically, it can securely be removed from the intravascular compartment, without endangering severe bleeding or fistula. As Tang and colleagues 1 have emphasized, the pressure gradient between the renal pelvis and the IVC may have an effect in the blockage of venous flow into the urinary system, especially considering that the false passage is about 2 mm in diameter. Furthermore, when a transurethral approach is used, it is easy to observe any persistent bleeding as the stent is extracted, and the potential complications of an angiographic intervention are also avoided.
Migration of a Double-J ureteral stent into the IVC is a rare and unforeseen complication. 3 It is imperative to be well prepared for difficult stent placement in problematic situations such as posthysterectomy strictures. In our experience of this uncommon case, transurethral endoscopic removal of the migrated intravascular Double-J stent was an effective and safe method.