
Abstract
Background and Purpose:
Different techniques have been used for the treatment of patients with anastomotic stenosis after radical prostatectomy (RP). In this retrospective study, we analyzed our experience with urethral dilation and consecutive transrectal ultrasonography (TRUS)-guided injections of long-acting steroids in the scar area.
Patients and Methods:
We reviewed the records of patients who underwent RP in our department from 2002 to 2010 and presented to the outpatient clinics with symptomatic anastomotic stenosis. Patients were treated with: Urethral dilation, cold knife (CK) urethrotomy, transurethral resection (TUR) of stenosis and dilation/resection of the strictures with consecutive TRUS-guided injection of a long-acting steroid (dilation+TRUS-steroids). Patients remained under follow-up, which included the assessment of voiding and continence patterns, as well as cystourethroscopy.
Results:
In 32 (10.8%) patients, symptomatic anastomotic stenosis was diagnosed. Initial urethral dilation succeeded in only 3 (10.3%) patients; thus, 29 remained with recurrent/resistant stenosis. Urethral dilation+TRUS-steroids was performed in 14 patients, while 8 patients underwent CK and in 7 TUR was performed. Patients in the dilation+TRUS-steroids group had lower re-treatment rates, and none of these patients became incontinent. Patients in the TUR group needed no re-treatment; however, they had the highest incontinence rate (57.1%). As a result, the highest efficiency quotient was in the dilation+TRUS-steroids with the lowest in the TUR group.
Conclusion:
Urethral dilation with consecutive TRUS-guided injections of steroids has the highest efficiency quotient and can be performed under local anesthesia with a low risk of incontinence.
Introduction
Patients and Methods
We reviewed the records of patients who underwent RP in our department from 2002 to 2010 and presented to the outpatient clinics with symptomatic anastomotic stenosis, which was based on the frequency and urgency of urination, persistent urine dribbling (especially after urination), and failure to empty the bladder or frequent emptying only with additional attempts. We analyzed patient demographics (body mass index, age, Charlson Comorbidity Index, previous surgical and urologic operations), and postoperative records to reveal a correlation between these different parameters and the rate of anastomotic stenosis. Postoperative bleeding was assessed by calculating the difference between the pre- and postoperative hematocrit (Hct). Fenig and associates 8 in their previous study found that the optimal cutoff point for postoperative blood loss was a decrease in Hct of more than 6 points. We adopted the former for the purposes of our study.
Patients with recurrent symptoms and/or a cystoscopic finding of resistant anastomotic stenosis (Fig. 1) were referred to our department and underwent either CK visual urethrotomy with/without transurethral injections of long-acting corticosteroids, transurethral resection (TUR) of stenosis, or dilation of the anastomotic stenosis with consecutive TRUS-guided injection of a long-acting steroid in the scar area (dilation+TRUS-steroids). These different treatments were chosen for each patient at the time by the attendant urologist based on experience and clinical judgment.
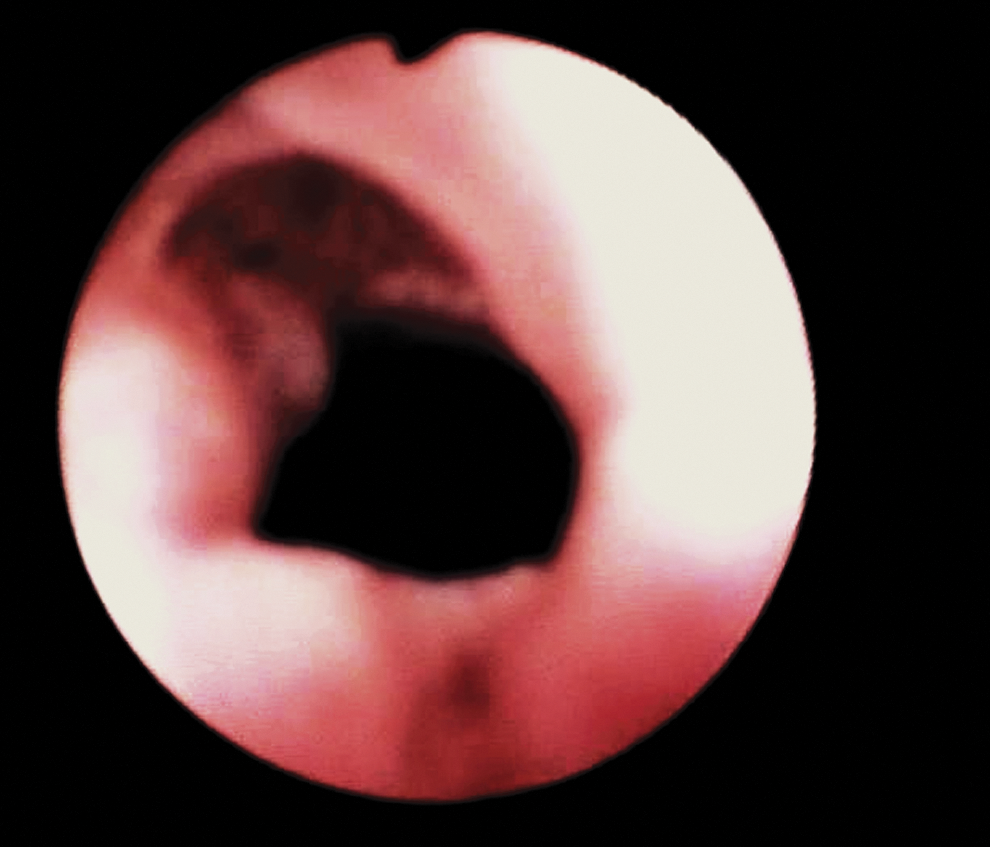
Bladder neck contracture: Narrowing in the area of anastomosis appeared with normal mucosa, and the 16F flexible cystoscope was unable to pass beyond this area.
Technique of stenosis dilation and TRUS-guided injection of long-acting steroids
All the patients in this group underwent an initial attempt of urethral dilation under local anesthesia. For this purpose, a 16F flexible cystoscope was gently placed into the urethra and advanced to the stenotic area. A 0.035-inch guidewire was then introduced and passed into the bladder. This step was followed by urethral dilation with an S∼Curve™/Urethral Dilator Set (Cook Medical Inc.). After the catheter insertion, patients were placed in the left lateral decubitus position, and the TRUS probe was inserted.
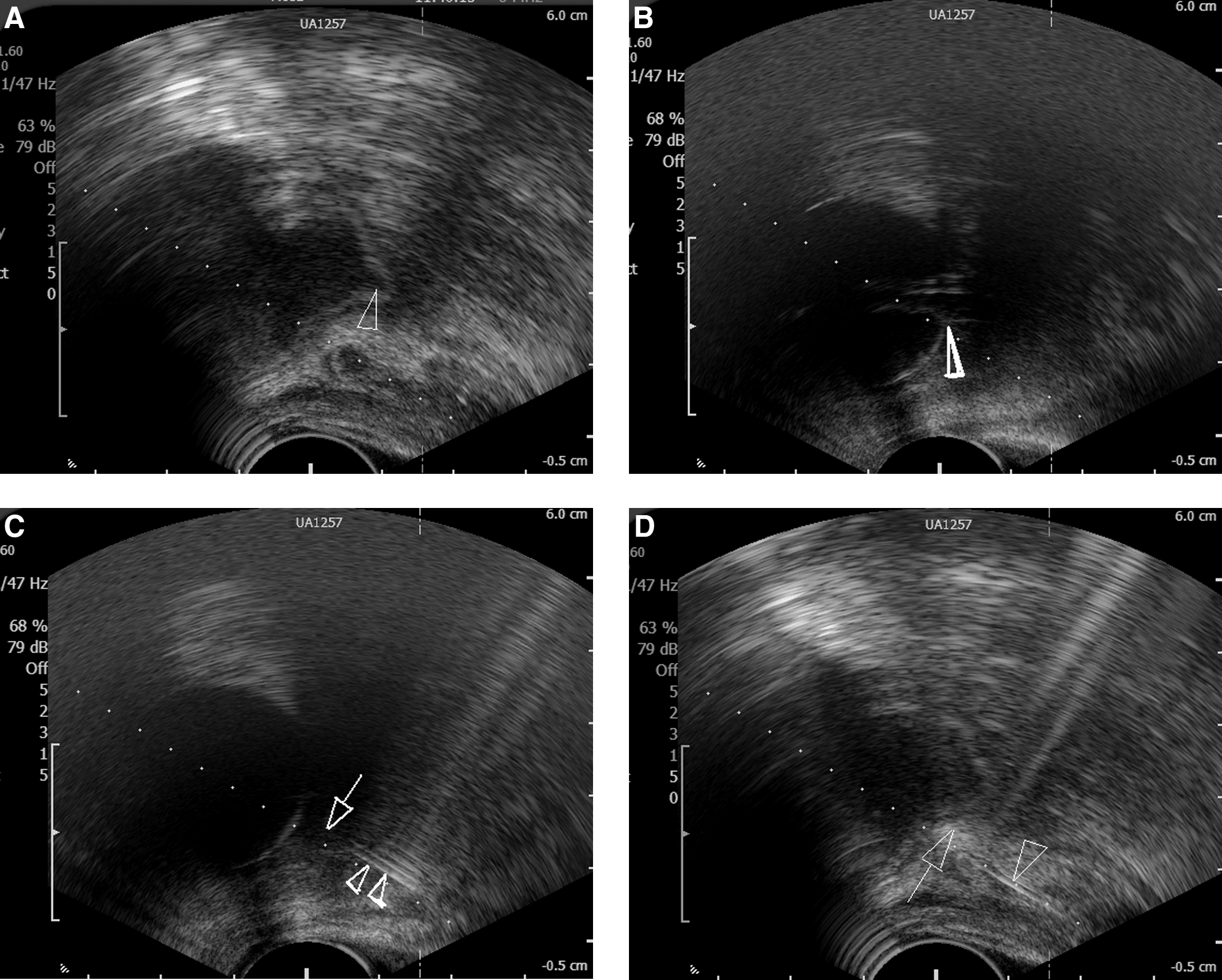
All procedures were performed by the same urologist (S.K.) who had previous experience with TRUS and transperineal prostate biopsies. A 22-gauge spinal needle was passed through the working channel, and a local anesthetic (1% lidocaine) was injected. The placement of the balloon helped localize the appropriate point for steroid injection. Relatively bulky hypoechogenic tissue around the bladder neck funnel and immediately adjacent to the peripheral part of the catheter was considered as the stenotic area. The Chiba biopsy needle was inserted and advanced directly to this point. To ensure homogeneous delivery of medication to the area, we usually injected 2 to 4 mL of methylprednosolone acetate (40 mg/mL) in 3 points (posterior and 2 lateral). We gently injected the medication, avoiding unintentional penetration into the bladder wall (Fig. 2).
All patients received ciprofloxacin 500 mg×2, which was started 1 day before the procedure and continued for 3 consecutive days. We also gave gentamicin, 80 mg intramuscularly, immediately after TRUS-guided injection. The urethral catheter was removed 12 to 16 hours after the procedure. In cases of hard and painful dilation, patients underwent the procedure under general anesthesia. In cases of recurrence, we performed CK incision of the scar area and consecutive TRUS-guided injection of steroids.
Patients were followed in the outpatient clinics. During the follow-up, we assessed the voiding pattern (satisfactory or unsatisfactory), continence (no pad), maximal urinary flow rate, residual volume, and cystourethroscopy. If the bladder neck appeared wide open on the first cystoscopy and patient continued to be satisfied with his voiding pattern, no further cystoscopy was performed.
To assess univariant differences between the study groups, we performed chi-square and one-way analysis of variance tests according to the nature of the variables (P≤0.05). The Fisher exact test was used to assess the difference between low volume groups. We used SPSS 13.0 statistical software. We also calculated the efficiency quotient for each treatment modality: [positive end point %/(100+re-treatment rate (%)+rate of auxiliary procedure (%))]×100. Widely opened anastomotic orifice and satisfaction were regarded as positive end points.
Results
Open RP was performed in 180 patients, while 117 men underwent laparoscopic radical prostatectomy (LRP). In 107 cases, bladder neck (BN) preservation or BN reconstruction with mucosal eversion was performed (BN preservation/reconstruction). There were no significant differences in demographic and postoperative parameters between patients with and without anastomotic stenosis, except for increased rate of blood loss in the group with anastomotic stenosis (1.3% vs 16.2%, P=0.043).
Patients became symptomatic 9.76±3.81 months after operation. The percentage of stenosis reached 8.4% (n=9) in the BN preservation/reconstruction group, compared with 12% (n=23) in the patients with BN resection without mucosal eversion. In 32 (10.8%) patients, symptomatic anastomotic stenosis was diagnosed. The mean age of the patients with anastomotic stenosis was 64.3 years (standard deviation±3.37). Patients became symptomatic 9.76±3.81 months after operation. Initial urethral dilation succeeded in only 3 (10.3%) patients. As a result, 29 men were referred for further treatment (Table 1) and remained in follow-up for 56.4±27.32 months.
RP=radical prostatectomy; TUR-BN=transurethral resection-bladder neck; Qmax=maximal flow rate.
Eight patients underwent CK, seven TUR, and 14 dilation+TRUS-steroids (Table 2). Patients in the TUR group were significantly older, while the dilation+TRUS-steroids group was the youngest (P=0.001). Patients in the dilation+TRUS-steroids group had lower re-treatment rates, and none of these patients became incontinent. Patients in the TUR group needed no re-treatment; however, they had the highest incontinence rate (57.1%). As a result, the highest efficiency quotient was in the dilation+TRUS-steroids group and the lowest in the TUR group.
TUR=transurethral resection; RP=radical prostatectomy; BNC=bladder neck contracture; BN=bladder neck; Qmax=maximum flow rate.
Discussion
Despite tremendous progress in laparoscopic and robot-assisted laparoscopic approaches, which has positively influenced the techniques of BN preservation and watertight anastomosis, the anastomotic stenosis is still present in 2.2 % to 12% of patients. 9 –11 Our retrospective records had identified symptomatic anastomotic stenosis in 10.8% of our patients. These patients had significantly higher postoperative blood loss. These data are in agreement with those previously reported and emphasize that significant postoperative bleeding might result in pelvic hematoma, which causes traction on and compression of the anastomosis and subsequent formation of stenosis. 8,9,12
Besarani and colleagues 2 reported that graduated dilation of the anastomotic stricture under light sedation was an effective treatment with a small number of patients needing additional procedures. The outcome of our study, however, showed that only 9.4% of the patients with anastomotic stenosis did not need further treatment. The results reported by Giannarini and coworkers 3 also showed that in only 7% of the patients was urethral dilation alone successful in relieving anastomotic stricture.
Consequently, most of the patients with anastomotic stenosis need different treatment. In our study, TUR showed the lowest re-treatment rates, and these data are in full agreement with the results reported by Popken and colleagues. 4 This technique, however, had the lowest efficiency quotient. This fact can be explained by the high rate of incontinence after TUR. The high rate of incontinence after resection could be explained by excessive damage to the external sphincter and is supported by the data reported by Gousse and associates 13 who used deep transurethral incision of the BN contracture with Collin knife electrocautery and showed an analogous rate of de-novo incontinence and a need for artificial sphincter implantation. In contrast, the dilation+TRUS-steroids group showed the highest efficiency quotient with a low re-treatment rate. With this technique, patients were free from incontinence, and the procedure was successfully performed under local anesthesia in 85.7% of the cases.
In fact, steroid injection is generally considered effective for scar reduction. The mechanism of action is complex and involves inhibition of fibroblast growth as well as increased activity of collagenase. Consequently, collagen deposition in the tissues is reduced, so that the scar becomes less thick and rigid. This method was successfully used in previous studies, dedicated to the treatment of resistant urethral strictures and recurrent BN contracture. 14,15 The bulk of the experience with this technique, however, comes from the literature dedicated to the treatment of refractory esophageal strictures. These studies emphasized the importance of ultrasonography-guided injection of steroids throughout the entire length of the stricture. 6,7
In our study, we used TRUS-guided injections of steroids into the scars. The rationale for this approach is based on the fact that in the transurethral technique, the needle has to be inserted into the scar. When the scar is too tough, it is very difficult to inject the content and, as a result, the needle can easily “penetrate” through and miss the scar tissue. Consequently, there is the risk of steroids being injected into relatively distant areas rather than close to the scar. To overcome this problem, the injection should be performed immediately peripheral to the affected tissue, with the needle directed to the scar area. TRUS control assures that the medication is injected homogeneously into the scar and in close proximity to the required area.
Several shortcomings of our study must be presumed. Our study is retrospective and, as a result, encompasses typical bias. We also took into account only symptomatic stenosis; the latter can hide the actual rate of this complication. We also recognize that this is a low volume study.
Conclusions
Anastomotic stenosis is still present even after BN preservation/reconstruction techniques. Most of the patients with this complication will need definitive form of treatment, other than graduated dilation of the anastomotic stenosis. Dilation+TRUS-steroids injection is a safe and reliable technique and has a low rate of recurrence and de-novo incontinence. In most of the cases, it can be performed under local anesthesia, and it might be considered as a “first-line” treatment option.
Footnotes
Disclosure Statement
No competing financial interests exist.