
Abstract
Background and Purpose:
Obese patients undergoing surgical procedures are at increased risk for perioperative morbidity. The purpose of this study is to determine whether there is an association with body mass index (BMI), clinicopathologic features, and perioperative outcomes and complications in patients undergoing robot-assisted laparoscopic partial nephrectomy (RPN).
Patients and Methods:
Medical records of 283 patients who underwent RPN between 2007 and 2012 were reviewed from an Institutional Review Board approved database. We analyzed the association of perioperative outcomes and complications of the surgery with BMI and clinicopathologic features using analysis of variance, Kruskal-Wallis test, t test and chi-square-test. Eventually, independent factors associated with perioperative outcomes and complications were studied using univariate and multivariate regression analysis.
Results:
Perioperative outcomes including estimated blood loss (EBL), length of hospital stay (LOS) and operative time (OT) were significantly associated with BMI (P=0.002, P=0.009 and P=0.002, respectively). Warm ischemia time (WIT), perioperative complications, and change in glomerular filtration rate (GFR) before and after surgery were not associated with BMI (P=0.459, P=0.86 and P=0.773). In multivariate analysis, BMI, tumor size≥4 cm, and collecting system invasion were independently associated with EBL and OT. Increased LOS was independently associated with BMI and tumor size ≥4 cm.
Conclusions:
Increasing BMI was not associated with a significant increase in perioperative complications, WIT, or change in GFR in patients undergoing RPN at a high-volume tertiary medical center. Collecting system invasion or tumor size ≥4 cm and BMI were independently associated with higher EBL, LOS, and OT, however.
Introduction
Obesity is a growing health concern in the United States and the rest of the world. The prevalence of obesity in the United States was 32% to 35% in 2007. 5 Obese patients undergoing surgery are at increased risk for perioperative morbidity. 6 –8 A growing number of patients with renal tumors who are candidates for PN have increased body mass index (BMI). 9 –12 Furthermore, patients with increased BMI pose certain technical challenges secondary to body habitus and increased perirenal fat. 13,14 Different measures of obesity including visceral fat obesity, 15 –17 visceral/subcutaneous fat ratio, and amount of perinephric fat have been investigated as predictors of perioperative outcomes in previous studies and may be associated with prolonged hospital stay and increased postoperative complications. 15 –19
We report perioperative outcomes and functional renal outcomes according to tumor histology, location, invasion, bulk of the tumors, and correlation with BMI in patients who underwent RPN.
Patients and Methods
A prospectively maintained, Institutional Review Board approved kidney cancer database was reviewed for patients undergoing RPN between October 2007 and March 2012. Demographics and perioperative outcomes including estimated blood loss (EBL) during surgery, length of hospital stay (LOS), warm ischemia time (WIT), operative time (OT), change of glomerular filtration rate (GFR), and perioperative complications (PC) occurring within 30 days of surgery were analyzed. GFR was calculated using the Modification of Diet in Renal Disease formula.
Tumors were grouped into subgroups (SG) based on location (hilar vs nonhilar), appearance (exophytic vs endophytic), invasiveness into the collecting system (invasive vs noninvasive), tumor size (≥4 cm and <4 cm), histopathology (clear-cell carcinoma and nonclear-cell histology), and Fuhrman nuclear grade (≥3 and <3). Tumors were considered to be exophytic if more than 50% of the tumor was exophytic. Adjacency to the collecting system is determined both by preoperative and intraoperative observation. Tumors were classified as invasive to the collecting system (necessitating entrance into and subsequent repair of the collecting system) or noninvasive to the collecting system. Invasion into the collecting system was determined by preoperative CT and/or intraoperative observation. Tumors extending ≤1 cm from the main renal vessels were considered to be hilar. Complications occurring within 30 days of surgery were noted. Trocars placement in our series of RPN for nonobese and obese patients is shown in Figure 1.
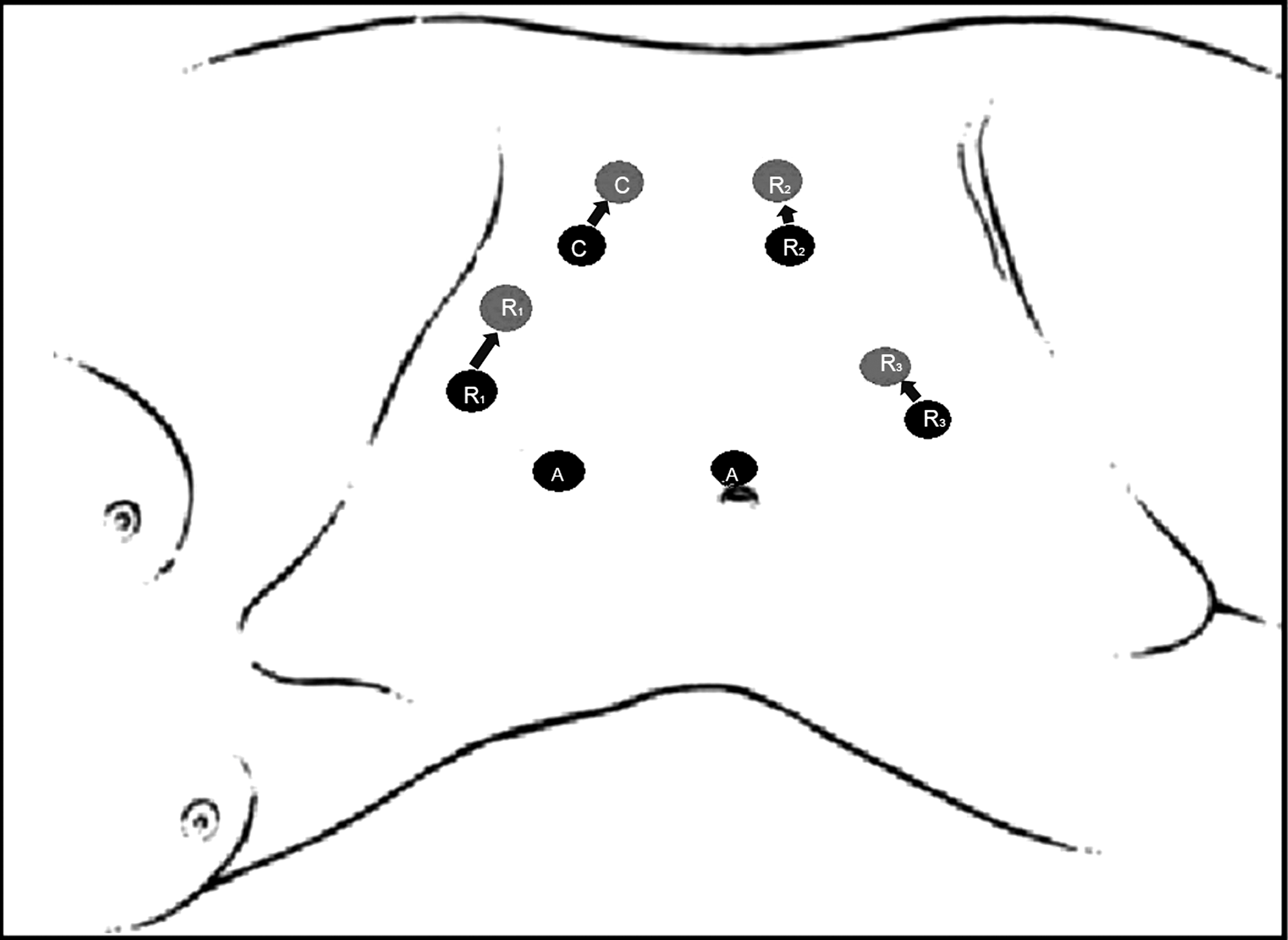
The placement of trocars in robot-assisted partial nephrectomy. Ports are moved laterally for obese patients vs nonobese patients as shown in gray. C: 12-mm camera port; R: 8-mm robotic arms; A: assistant ports.
Study design
(1) Based on BMI, patients were categorized into five groups according to the WHO (World Health Organization) classification. Perioperative outcomes, age, and SG were compared based on BMI categories using one-way analysis of variance (for continuous) and Kruskal-Wallis test (for categorical) (Table 1).
(2) Perioperative outcomes, BMI, and also tumor size were compared using independent samples t test (for continuous) and chi-square/Fisher exact test (for dichotomous) in SG (Table 2).
(3) EBL, LOS, OT, WIT (continuous as dependent) were studied in univariate linear regression analysis to demonstrate the association between BMI (continuous as independent).
(4) PC (dichotomous as dependent) was studied in logistic regression analysis to demonstrate the association with BMI (continuous as independent).
(5) Perioperative outcomes (as dependent) were studied with BMI (as independent) and SG (as independent) in multivariate analysis. Only the perioperative outcomes that were significantly associated with BMI (P<0.05) in linear (for EBL, LOS, OT, WIT) or logistic (for PC) regression analysis were incorporated in multivariate analysis.
(6) Similarly, the SG showing a significant difference in chi-square/Fisher's exact test in BMI categories were incorporated in multivariate analysis. The statistical analysis was performed using SPSS 17.0 (Chicago, IL) statistical analysis program.
BMI=body mass index; EBL=estimated blood loss; LOS=length of stay; WIT=warm ischemia time; OT=operative time; GFR=glomerular filtration rate
EBL=estimated blood loss; LOS=length of stay; OT=operative time; WIT=warm ischemia time; PC=perioperative complications; BMI=body mass index.
Results
There were 283 patients who underwent RPN available for review. Of these, procedures for 13 were converted to OPN or RPN (8 conversions to OPN and 2 conversions to robot-assisted radical and 3 conversions to laparoscopic radical). The remaining 270 patients were included in this analysis. Patient demographic data are listed in Table 1. The mean and median age of the study group was 60±11.6 and 60 years, respectively. Mean and median tumor size was 2.93±1.26 cm and 2.7 cm, respectively. Mean EBL, LOS, OT, and WIT were 295.6±286.98 mL, 3.41±1.13 days, 200±48.9 minutes, and 22.9±10.4 minutes. Perioperative complications occurred in 18 (6.6%) patients, and there were no perioperative deaths. Sixteen complications occurred postoperatively (Clavien grade I: 11 patients; Clavien grade II: 1 patient; Clavien grade IIa: 2 patients; and Clavien grade IIIb: 1 patient) and 2 perioperatively (not classified). Descriptions and grading of the complications are in Table 3.
DVT=deep vein thrombosis; PE=pulmonary embolism; ATN=acute tubular necrosis; ARF=acute renal failure; IV=intravenous.
The maximum and minimum scores of BMI were 46.8 and 18.1 kg/m2, respectively. According to the WHO classification, the number of patients in each category includes: 52, 19.2% (normal weight: BMI <24.9 kg/m2); 110, 40.7% (overweight: BMI=25–29.9 kg/m2); 71, 26.3% (grade 1 obesity: BMI=30–34.9 kg/m2); 20, 7.4% (grade 2 obesity: BMI=35–39.9 kg/m2); and 17, 6.3% (grade 3 obesity: BMI >40 kg/m2).
Of the 270 tumors, clear-cell renal-cell carcinoma (RCC) was present in 153 (57.4%) patients, papillary RCC in 46 (17%) patients, oncocytoma in 31 (11.5%) patients, angiomyolipoma in 16 (5.9%) patients, chromophobe RCC in 13 (4.8%) patients, simple renal cyst in 3 (1.1%) patients, metanephric adenoma in 2 (0.7%) patients, leiomyoma in 1 (0.4%) patient, renal carcinoid in 1 (0.4%) patient, and unclassified neoplasms in 4 (1.5%) patients. Of the patients with clear-cell RCC, 10 (6.5%) had tumors with Fuhrman nuclear grade ≥3. Fifty-three (19.6%) renal masses were hilar, and 113 (41.9%) tumors were endophytic. Collecting system invasion was noted in 43 (15.9%) cases. Eighty-one (30%) of the masses were ≥4 cm.
There was no demonstrated significant correlation between perioperative outcomes and age or sex. Increased EBL (P=0.002), increased LOS (P=0.009), and increased OT (P=0.002) were all associated with increasing BMI (Table 1). There was a positive correlation between clear-cell histology and increasing BMI, with clear-cell carcinoma present in 48.1% of normal weight patients, 50.9% of overweight, 62% of grade 1 obesity, 65% of grade 2 obesity, and 88.2% of grade 3 obesity patients (P=0.024).
The comparisons of the mean values with standard deviations of perioperative outcomes, tumor size, and BMI in each SG are shown in Table 2. EBL, LOS, OT, and WIT were significantly different in size ≥4 cm than <4 cm (P<0.001, P=0.002, P<0.001, and P=0.001, respectively). EBL, OT, and WIT were significantly greater in patients with collecting system invasion (P<0.001, P=0.001, and P<0.001, respectively). Increased WIT was significantly associated with hilar tumors (P=0.003). Perioperative complications were noted more frequently in patients with collecting system invasion (P=0.038). Mean BMI for patients with clear-cell histology was greater compared with mean BMI for patients with nonclear-cell histology (30.4±5.8 vs 28.2±4.6; P=0.001).
Using univariate regression analysis, EBL (P<0.001), LOS (P=0.009), and OT (P<0.001) were significantly associated with BMI (Fig. 2). WIT (P=0.696; R2=0.001), and PC (P=0.448; odds ratio [OR]: 1.03, 95% confidence interval [CI]: 0.95–1.12) were not associated with BMI, however.
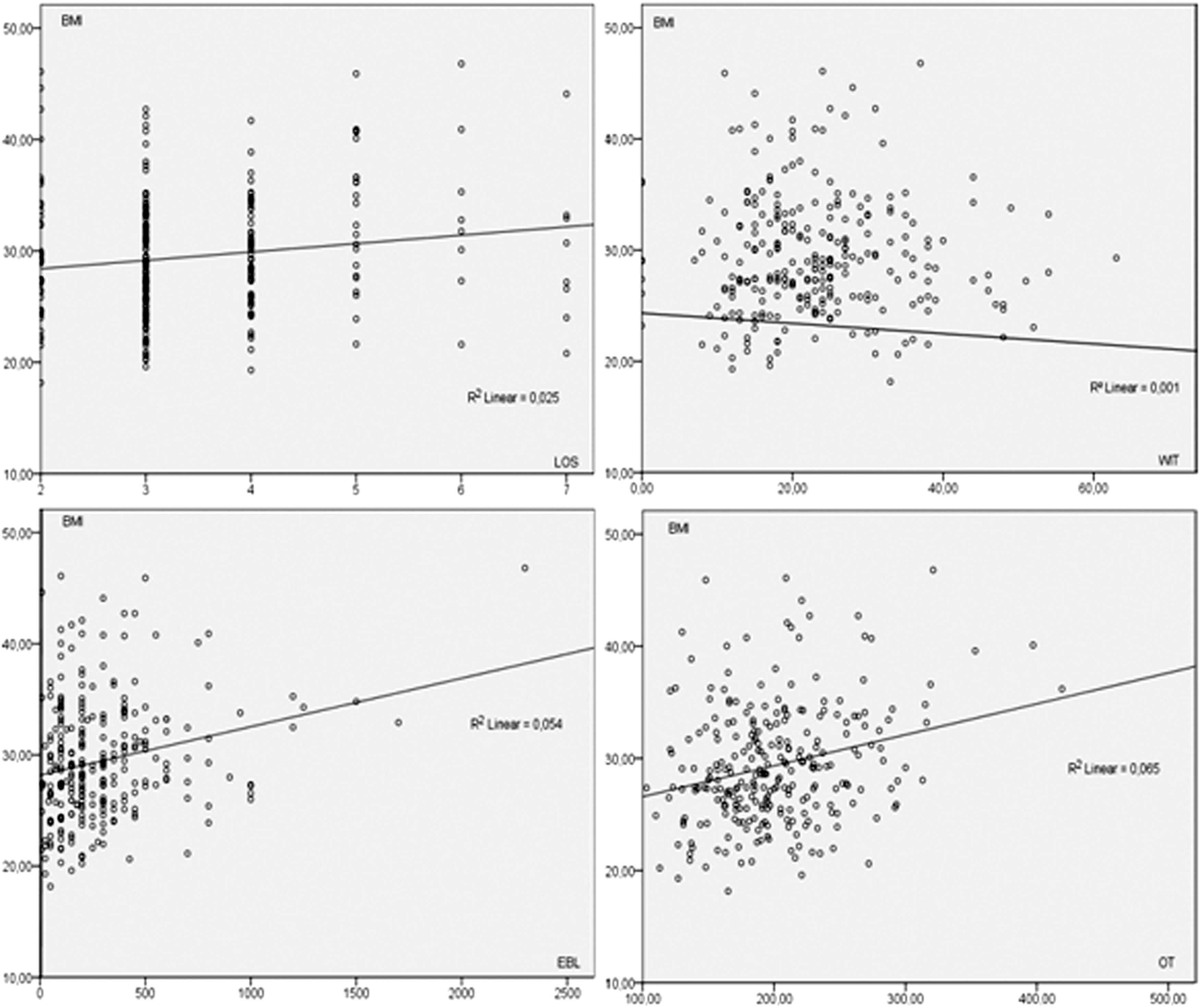
Comparison of estimated blood loss (EBL), length of hospital stay (LOS), operative time (OT) and warm ischemia time (WIT) with BMI by linear regression analysis (P<0.001, P=0.009, P<0.001 and P=0.696, respectively).
WIT was excluded from multivariate analysis because it was not correlated to BMI on univariate analysis. SG and BMI were studied using multivariate regression analysis to estimate EBL, LOS, and OT. BMI demonstrated a significant correlation with EBL, LOS, and OT in multivariate analysis as an independent variable (P<0.001, P<0.001, and P<0.001, respectively). Collecting system invasion and tumor size were independently associated with EBL (p<0.001, P<0.001, respectively) in the multivariate model. Tumor size was also independently associated with LOS (P=0.002). OT demonstrated a significant correlation with collecting system invasion and tumor size (P=0.024, P<0.001).
GFR change was not associated with BMI (P=0.747). Also, comparing the categories of BMI showed no difference of change in GFR (Table 1). Change in GFR, however, was significantly associated with OT and WIT (P=0.049 and P<0.001, respectively) but not EBL and LOS in univariate linear regression analysis.
Discussion
Increasing rates of obesity have become a public health concern in recent decades. 5 It has been clearly demonstrated that obesity is associated with metabolic disorders such as diabetes, hypertension, coronary artery disease, and metabolic syndrome. 5 From the epidemiologic standpoint, various factors have been proposed to explain the association of obesity and RCC. 20,21
Morbid obesity is also a documented potential risk factor for increased postoperative complications. 22 –24 Higher rates of conversion to open surgery have been reported in obese patients undergoing laparoscopic surgery. 25 Nitori and associates 26 compared obese (BMI ≥30) and nonobese (BMI <30) patients (n=77 vs n=21, respectively) undergoing laparoscopic colorectal surgery. 26 Within this series, patients with a BMI >30 had a higher conversion rate than open surgery (8.3% vs 1.1%). In a similar group of patients undergoing laparoscopic colorectal surgery, Kamoun and colleagues 27 compared 118 patients with BMI <30, and 62 patients with BMI ≥30. A higher open conversion rate (32.3% vs 14.4%) was associated with patients with BMI ≥30. Interestingly, a higher rate of conversion to open surgery has not been demonstrated in obese patients undergoing LPN. Colombo and coworkers 28 compared patients with BMI ≤30 (n=238) with patients with BMI >30 (n=140). There were two conversions in the nonobese group and four conversions in the obese group, although these numbers were not statistically significant. Similarly, Romero and colleagues 29 reported no open conversions in a cohort of obese (BMI ≥30; n=56) and no-obese (BMI <30; n=56) patients undergoing LPN. Similarly, within our study, we did not find a statistically significant difference in conversion rate between the weight categories of patients undergoing RPN (P=0.679, Table 1).
Our study did show a significantly increased risk of several adverse perioperative outcomes for patients in higher weight categories. There was a statistically significant difference in EBL between patients with normal weight, overweight patients, and those with grades 1, 2, and 3 obesity (183±163 vs 286±233 vs 361±326 vs 275±284 vs 447±528, respectively; P=0.002). Similarly, Naeem and associates 30 reported higher EBL in obese patients undergoing RPN compared with nonobese patients (P=0.026, Table 4), as did Romero and coworkers 29 in a comparison of obese vs nonobese patients undergoing LPN (P<0.05; Table 4).
Data presented as mean values and percentages unless stated otherwise.
Intraoperative complications; bpostoperative complications; c<50% endophytic, n (%); d50% to <100% endophytic, n (%); e100% endophytic, n (%); fcollecting system repair, n (%); gmedian value; hmean change in GFR; i% change in GFR; jendophytic, n (%); khilar, n (%), lcollecting system invasion, n (%).
EBL is lower in BMI <30 group than BMI ≥30, P=0.026; μEBL is lower in BMI <30 group than BMI ≥30, P<0.05; §This study included patients who underwent laparoscopic and open partial nephrectomy. This table includes only the results of the laparoscopic subset of patients; ¶EBL is higher as BMI gets higher, P=0.002; #LOS is higher as BMI gets higher, P=0.009; УOT is higher as BMI gets higher, P=0.002.
EBL=estimated blood loss; LOS=length of stay; OT=operative time; WIT=warm ischemia time; PC=perioperative complications; GFR=glomerular filtration rate; LPN=laparoscopic partial nephrectomy; BMI=body mass index; RPN=robot-assisted partial nephrectomy.
In the present study, we noted a statistically significant increase in operative time with increasing BMI. We also saw a significant association between longer length of stay and higher BMI, though the cause of this is also unclear. In contrast, differences in OT and LOS were not demonstrated in other studies comparing obese and non-obese patients undergoing minimally invasive (laparoscopic and robotic) partial nephrectomy. Interestingly, we found no statistically significant differences in WIT, change in GFR, or perioperative complication rates among BMI categories, which is consistent with previous studies of patients undergoing LPN or RPN (Table 4).
An increased incidence of clear-cell RCC was noted by Bergstöm and coworkers 31 among tumors excised for patients in higher BMI categories. This finding was statistically significant in our study as well. Similarly, this risk increase has been indicated in a number of large epidemiologic cohort series. 32,33
The present study represents the largest study within the literature analyzing the impact of BMI on perioperative outcomes in patients undergoing RPN. It is also unique in that we grouped patients into five different BMI categories compared with other studies in which patients were categorized into two study groups: Obese and nonobese. Categorization into five groups limited the BMI distribution and, in addition, the use of regression analysis resulted in reduction of type 1 error. A limitation of this BMI distribution technique is the inherent increase in type 2 error. Furthermore, an additional limitation was the retrospective nature of the study and that the patients were enrolled nonconsecutively. Although the study population was relatively large, our sample size may still be inadequate to show subtle differences in outcomes between subgroups. Other factors causing increased EBL, LOS, and OT may have confounded our results, although we did control for known determinants using multivariate analyses.
Conclusions
With the increased prevalence of obesity among the population and stage migration of renal tumors, an increased number of obese patients will need treatment for small renal tumors. The current article underlines the feasibility and safety of RPN for obese patients. In centers performing a high volume of nephron-sparing surgery, RPN can be referred as a viable treatment option for obese patients with small renal masses without the risk of increased perioperative morbidity.
Footnotes
Disclosure Statement
No competing financial interests exist.