
Abstract
Purpose:
To evaluate our initial outcomes of retroperitoneal partial nephrectomy (RPN) performed by off-clamp excision.
Patients and Methods:
Between January 2011 and October 2102, patients with T1 posterior renal masses or in the renal convexity were selected for RPN with the intent of performing the modified zero ischemia technique. Patient characteristics, operative details, complications, and long-term outcomes were analyzed.
Results:
There were 19 patients included (mean age 60 years, range 37–81 years; body mass index 27.8 kg/m2, range 25–34 kg/m2). Mean tumor size was 35 mm (20–50 mm), and preoperative aspects and dimensions used for an anatomical (PADUA) classification score was 9 (7–11). Surgical time was 182 minutes (110–255 min), and the series warm ischemia time was 4.9 minutes (0–28 min). The off-clamp procedure was performed in 15 (79%) patients. Mean estimated blood losses (EBL) were 414 mL (100–1600 mL). Transfusion was necessary in two cases, while one reoperation and one conversion to open surgery were needed. Mean hospital stay was 4.5 days (range 3–11). One (5.3%) case of positive margins was reported. Serum creatinine levels varied from 86 to 94 μmol/L (preoperative and 6-month follow-up). Considering the learning curve of the technique, separate analysis of the initial 9 and last 10 cases revealed that while tumor characteristics remained comparable (size 33 vs 37 mm; PADUA score 8.8 vs 9.2), no clamping was performed in the later cases with decreased EBL (544 vs 297mL), surgical time (207 vs 159 min), and shorter hospital stay (5 vs 4 days).
Conclusion:
Our preliminary results on off-clamp RPN are promising and may pave the way for a real zero ischemia nephron-sparing surgery. Larger and randomized studies should follow in to confirm our initial results.
Introduction
More conflicting data on the determinant role of ischemia with respect to renal function outcomes are provided by studies on renal transplants from nonheart-beating donors that reveal an excellent long-term graft survival rate. 5 Nonetheless, and despite the absence of a consensus on the most appropriate cut point for WIT, it would seem reasonable to assume that a short or, better still, zero ischemia time will be better for the kidney.
With this in mind, several authors have published technical modifications related to vascular clamping with the aim of reducing the WIT during laparoscopic partial nephrectomy (LPN). 6,7 Recently, Ng and associates 8 and Gill and colleagues 9 proposed a “zero ischemia” technique through a combination of pharmacologically induced hypotension with renal artery branch microdissection and superselective clamping during transperitoneal LPN. It is, however, reasonable to consider that at least some level of ischemia will still result from both the induced hypotension and the superselective clamping. Interest in the quest for a pure zero ischemia technique is further manifested by a recent report from Novak and coworkers 10 on a preliminary series of off-clamp robot-assisted transperitoneal LPNs.
Based on our initial experience of retroperitoneoscopic partial nephrectomy (RPN) with delayed clamping, we realized that in many patients, off-clamp excision is feasible with reasonable blood loss and no major complications. Whether this is a consequence of the retroperitoneoscopic access itself, or an optimized enucleation technique, or the particularities of the arterial supply of the posterior renal surface, with the posterior segmental artery supplying up to 50% of the renal parenchyma, 11 remains unclear.
Our purpose is to present our initial experience of a modification of the superselective clamping technique described by Gill and associates, 9 adapted to the retroperitoneoscopic approach for tumors located in the posterior renal aspect and renal convexity, the ultimate aim of which is to achieve pure off-clamp nephron-sparing surgery.
Patients and Methods
The present series includes our initial experience with retroperitoneoscopic nephron-sparing surgery. All the cases were performed by the same surgeon (JAP) in our institution, where 530 laparoscopic radical nephrectomies have been performed since 2001 and 276 LPNs since 2002. Between January 2011 and October 2012 (22 mos), 19 consecutive patients with T1 renal tumors located at the posterior aspect and the renal convexity were considered candidates for RPN with the intent of using the off-clamp technique described here. Data were recorded prospectively. Patient characteristics including age, sex, body mass index (BMI), and American Association of Anesthesiologists (ASA) score were analyzed. Tumors were classified according to the preoperative aspects and dimensions used for an anatomical classification system based on CT findings (PADUA) (Fig. 1). 12

CT cross-section showing posterior renal mass in the right kidney.
With regard to the surgical technique, we assessed operative time, type of arterial preparation and clamping, WIT, estimated blood loss (EBL), blood transfusion, complications (Clavien system), 13 and length of hospital stay. Pathologic data were also recorded, and serum creatinine levels and estimated glomerular filtration rate were analyzed preoperatively and at 6 months.
Surgical technique
Patient position
Patients underwent the procedure in the flank position.
Retroperitoneal access and port placement
After a 1.5-cm incision distally to the 12th rib and incision of the external oblique aponeurosis, blunt dissection of the three muscular layers was performed, gaining access to the retroperitoneal space. Blunt dissection permitted psoas muscle identification and lower renal pole dissection, while the peritoneum was displaced anteriorly. A Gaur balloon was placed in this space and filled with 400 mL of saline, leading to the formation of an ample retroperitoneal cavity adequate for placement of the remaining trocars.
Two 5-mm ports were aligned in a theoretical subcostal line, one at the level of the angle between the 12th rib and the paravertebral muscles and the other as anteriorly as possible without perforating the peritoneum. A third 12-mm port was placed above the iliac crest, slightly posterior to the line of the first incision. Ports were placed in a blind way, protecting its extremity with the index finger. Finally, to avoid CO2 leakage and to accelerate wound closure at the end of the procedure, a tobacco-pouch suture was made at the site of the first incision and a 12-mm port placed through it. Therefore, a four-port approach was available for the surgical procedure, with one port above the iliac crest for the scope, an anterior one for the assistant, and ports located at the 12th rib extremity and at the posterior costal angle through which the surgeon operated.
Renal pedicle access
Insufflation of the retroperitoneum was performed with working pressures of 14 mm Hg and maximum influx rate. After identification of the psoas muscle, the posterior renal surface was displaced anteriorly and a stepwise identification of the vena cava or aorta (depending on the side), ureter (in the case of lower pole tumors), and renal vein and artery was possible.
Renal artery branch microdissection
After identification and dissection of the main renal artery, a modified Rumel tourniquet 14 fixed with a Hem-o-lok® XL clip (Weck Closure Systems, Triangle Park, NC) to avoid its displacement was left unfastened (Fig. 2). Dissection of the artery was performed in the distal direction until its posterior or retropelvic branch (posterior segmental artery) was identified. The latter describes an arch that passes at the base of the infundibulum of the superior pyelocaliceal group and then descends toward the lower renal pole, giving origin to branches supplying the posterior renal surface. 11 An additional Rumel tourniquet was left unfastened in this arterial branch, with clamping being reserved for cases of profuse bleeding during tumor excision.
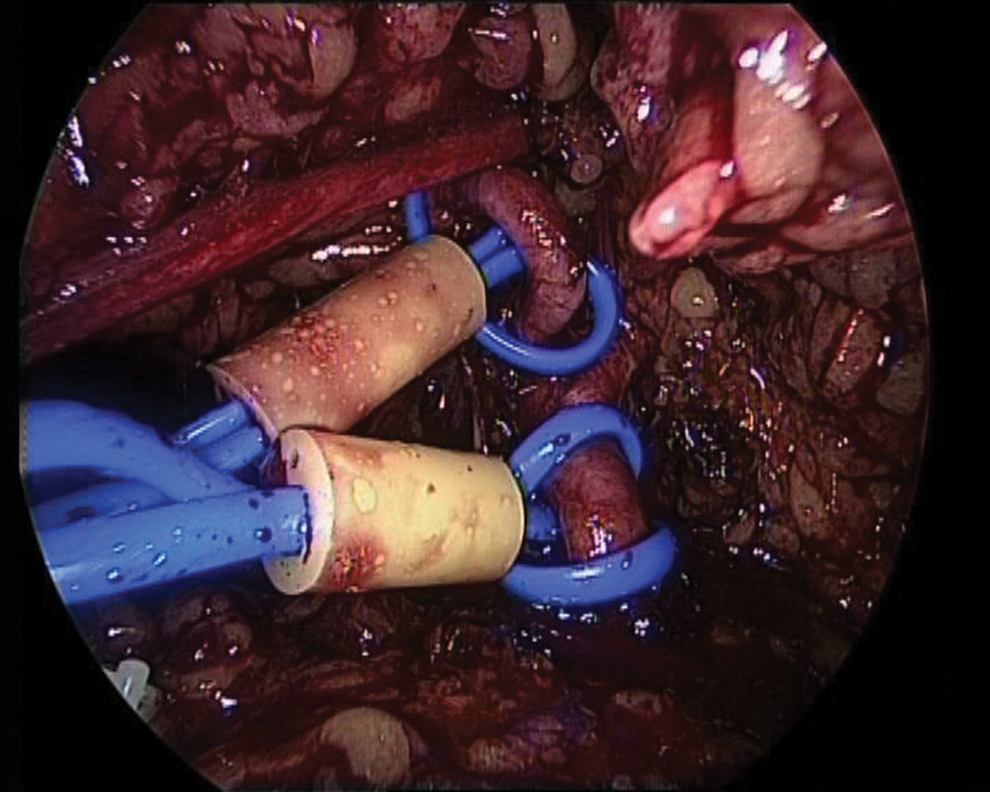
Unfastened Rumel tourniquets in renal (below) and retropyelic (above) arteries (laparoscopic retroperitoneal access).
Tumorectomy/PN
After endocavitary ultrasonography-assisted tumor location, the peritumoral adipose tissue was dissected and the external limit of excision marked on the renal capsule using electrocoagulation. Moreover, artery dissection was performed in a distal direction and, when a small direct branch to the tumoral surface was observed, a 5-mm Hem-o-lok ligation clip was applied. Finally, cold-scissor tumor excision was performed, seeking the proper enucleating plane and applying only selective electrocoagulation. Importantly, all enucleations started without fastening the tourniquets; fastening only took place if bleeding was considered uncontrollable or impaired visibility. Occasionally, an increase in pressure up to 20 mm Hg was used during this phase. If a blood vessel was clearly identified in the resection bed, a 5-mm Hem-o-lok was applied.
If necessary, closure of the urinary tract was achieved by using a 3/0 monofilament reabsorbable running suture, anchored in the renal capsule with a Hem-o-lok clip. To enhance hemostasis, human thrombin was often applied at the tumor base (FloSeal,® Baxter Inc, Deerfield, IL). Renal parenchyma was closed using reabsorbable suture with the “sliding clip” technique. Once the specimen had been placed in an endobag and hemostasis revised, a Jackson-Pratt drain was placed through a 5-mm port and the tissue retrieval bag extracted by extension of the incision of one of the 12-mm ports. Finally, wound closure was performed.
Postoperative care
An oral diet was initiated 12 hours after the operation, and bed rest was maintained during the first 24 hours. Abdominal drainage was retained as a precaution for 3 days, and the patient was usually discharged on the fourth postoperative day.
Results
Mean patient age was 60 years (37–81 years), and the majority of the patients were men (15 men, 4 women). Mean BMI was 27.8 kg/m2 (25–34 kg/m2). Patients were classified as ASA 3 in 37% and ASA 2 in 63% of the cases. Mean tumor size was 35 mm (20–50 mm) and the PADUA score was 9.0 (7–11).
Concerning the surgical details (Table 1), mean operative time was 182 minutes (110–255 min), and the mean WIT of the whole series was 4.9 minutes (0–28 min). The operation was performed avoiding clamping of the main renal artery in 16 (84%) patients. Moreover, pure off-clamp surgery was possible in 15 (79%) patients. Mean EBL was 414 mL (100–1600 mL), with two (10.5%) patients needing blood transfusion. In one of the latter cases, conversion to open surgery was necessary because of persistent hemorrhage after unclamping of the main renal artery after 10 minutes of ischemia. In the other case, reoperation and renorraphy were necessary because of major postoperative bleeding. Mean hospital stay was 4.5 days (range 3–11 days).
Arterial preparation refers to dissection and placement of an unfastened Rumel clamp. Whenever the Rumel clamp remained loose, warm ischemia time (WIT) is displayed as zero. Anatomopathologic features are also displayed.
ASA=American Association of Anesthesiologists; BMI=body mass index; EBL=estimated blood loss; CCC=clear-cell carcinoma; papilar 1=type 1 papilar carcinoma; papilar 2=type 2 papilar carcinoma.
Pathologic examination reported oncocytoma in four cases and renal-cell carcinoma in the remaining 15 (Table 1). One (5.3%) case of positive margins was reported. Concerning renal function before operation and at 6 months of follow-up (available in seven patients), the mean serum creatinine level and estimated glomerular filtration rate (Modification of Diet in Renal Disease formula) altered from 86 to 94 μmol/L and from 77 to 70 mL/min/1.73 m2, respectively.
If the evolution and learning curve of the technique is considered (Fig. 3) and the initial 9 and last 10 cases are analyzed separately, it is observed that while tumors presented similar characteristics (size 33 vs 37 mm; PADUA score 8.8 vs 9.2), off-clamp surgery was possible in every case in the later group, which presented lower EBL (544 vs 297 mL), reduced surgical time (207 vs 159 min), and shorter hospital stay (5 vs 4 days).

Distribution of tumor size (cm), PADUA score, and evolution of warm ischemia time (min) in our series. Chronologic representation is shown.
Discussion
Nephron-sparing surgery has become the treatment of choice for masses less than 7 cm in diameter. Nonetheless, its implementation, particularly when a laparoscopic approach is chosen, may entail a longer WIT and consequently affect the postoperative renal function. 1,3
In this study, we report our preliminary experience of RPN in tumors of the posterior renal surface and renal convexity, evolving from an initially modified technique of delayed superselective clamping to a pure off-clamp excision as our increasing experience indicated the latter's feasibility. The rapid and excellent visualization and dissection of the renal artery and its branches permitted by this approach gave us the necessary on-demand control of the renal vascular supply. While allowing us to dramatically decrease the WIT, the approach also permitted the off-clamp procedure to be performed in 79% of the patients. Interestingly, after the ninth patient, all cases were performed off-clamp, with reduced bleeding (297 mL), shorter surgical time (159 min), and shorter hospital stay (4 days).
Several publications have previously compared PN performed by transperitoneal and retroperitoneal approaches. While similar oncologic outcomes were described, it was found that the retroperitoneal approach might result in decreased operative time, bleeding, ileus, and hospital stay in selected tumors located in posterior or posteriomedial areas. 15 In anteriorly or laterally located tumors, however, as well as in large masses necessitating extensive resections (even if in a posterior location), the transperitoneal approach seems preferable. 16 In fact, the lack of space and triangulation makes the retroperitoneal approach technically more demanding. Retroperitoneoscopy is particularly attractive in cases of posterior renal masses, especially if some type of selective clamping is considered, because it circumvents the need to completely dissect the kidney in order to flip it, while simultaneously providing an excellent approach to the arterial network of the kidney.
Renal ischemia decreases intraoperative bleeding, improves access to the collecting system and visualization of the tumor during resection, and eases the closure of the renal parenchyma. The duration of clamping is, however, the main predictive factor for postoperative recovery of renal function. 3 After experimental studies suggesting that renal damage starts 20 to 30 minutes after clamping in the human kidney, a WIT of up to 30 minutes was for many years considered satisfactory in that it would allow complete recovery of renal function. 2 Today, however, a WIT of up to 20 minutes is recommended. 3 In fact, in a retrospective study of 362 patients with a solitary kidney who underwent PN, the authors found that each additional minute of warm ischemia was associated with a 5% increase in the odds ratio of development of acute renal failure in the immediate postoperative period and a 6% increase in the likelihood of development of chronic renal failure during follow-up. These observations suggest that “each minute of warm ischemia counts.” 4
Consequently, technical modifications related to clamping have been proposed, aimed at a reduction in WIT. Bollens and colleagues 7 described clamping on demand with a mean WIT of 9 minutes, while Nguyen and Gill 6 presented the technique of early unclamping, decreasing its mean WIT to 14 minutes. Finally, Ng and associates 8 and Gill and coworkers 9 published the technique of “zero ischemia” in transperitoneal LPN by combining pharmacologically induced hypotension with a demanding microdissection and superselective clamping of renal artery branches, alongside endocavitary Doppler ultrasonography assistance.
Despite these important advances, it is reasonable to consider that these techniques still induce at least some degree of renal injury and that an off-clamp technique would be less deleterious. In fact, the quest for a real zero ischemia technique is highlighted by recent work by Novak and colleagues 10 that reports the feasibility of off-clamp robot-assisted transperitoneal PN in a series of 22 of 57 consecutive patients. Although a slightly lower EBL was observed (274 mL) compared with our global series, similar surgical time and rate of transfusion were reported. It is also to be noted that the patients who underwent off-clamp procedures presented smaller renal masses (21 mm) than those of our series.
Some previous series, mostly on transperitoneal LPN, have likewise suggested that in selected cases, an off-clamp technique may be used without serious additional complications. 17,18 It is noteworthy that the majority of the patients treated without ischemia in both of the cited series 17,18 presented low-complexity tumors. In this respect, in the series from the University of Michigan, a decision algorithm restricted use of the pure off-clamp technique to tumors with less than 5 mm penetration into the renal parenchyma, 17 while in the Long Island series, 68% of cases were low-complexity tumors, with a mean tumor size of 2.7 cm. 18 In contrast, in our initial series, a zero ischemia technique was applied in more complex lesions, as shown by the elevated PADUA scores and greater tumor size. In the future, as the technique becomes reproducible, well-defined criteria could eventually be used to decide whether arterial network dissection can be avoided.
In our center, we adapted the technical modifications described by Bollens and Gill 7 –9 to the retroperitoneal approach. It should be highlighted, however, that in all cases needing vascular control, on-demand clamping and early unclamping were performed independently of the arterial structure. Thus, in our initial experience, among the 19 PNs performed by retroperitoneoscopy, we were able to achieve an average WIT below 5 minutes without clamping the main artery in 84% of cases (n=16). In addition, real zero ischemia was attained in 15 (79%) cases by only performing selective dissection and ligation of blood vessels supplying nutrients to the tumor. It is notable that experience with the technique had an obvious impact on its applicability, because in the last 10 cases, off-clamp surgery was possible in every patient.
The ease of vascular access permitted by the retroperitoneoscopic approach, along with the characteristic arterial anatomy of the posterior renal surface, where the posterior segmental artery supplies up to 50% of the renal parenchyma, 11 render this approach ideal for the management of posteriorly located tumors. Possibly, the combination of this approach with an optimized enucleation technique, whose oncologic equivalence with standard PN has been previously reported, 19 –21 may contribute to the feasibility of off-clamp surgery in patients with posterior renal masses.
According to our experience, tumor location close to the renal pedicle facilitates the identification of small-caliber tertiary blood vessels that directly supply the mass, allowing a near-bloodless tumor excision. In the case of tumors more distant from the pedicle, an unfastened Rumel tourniquet was placed and selective or total clamping performed if necessary. Delayed clamping and early unclamping were used to reduce the impact of ischemia in the remaining renal parenchyma. Thus, no significant impact on glomerular filtration rate was observed on follow-up, although data on renal function at 6 months were available for fewer than half the patients.
The PADUA score predicts the risk of complications in a PN. 12 The score obtained from preoperative anatomic data allows classification of patients into low-, intermediate-, and high-risk groups (scores below 8, between 8 and 9, and above 9, respectively). In our series, patients were categorized in the intermediate-risk group, with a mean score of 9.
Although no major complications were observed in our series, three modified Clavien scores of I, IIa, and IIIb were verified. One of the noteworthy complications was the need for conversion to open surgery and transfusion in a patient in whom active bleeding persisted after 10 minutes of selective posterior segmental artery clamping plus 10 additional minutes of clamping of the main renal artery. Another was the need for reoperation and renorraphy because of postoperative major bleeding. Postoperative transient fever that remitted with antipyretics developed in a third patient. Although our series presented higher mean blood loss than has been reported by other authors (Bollens and coworkers 7 reported 150 mL with a transfusion rate of 20% in the context of on-demand clamping while Ng and colleagues 8 described EBL of 300 mL with early unclamping and 200 mL when using the zero ischemia plus microdissection technique without specification of the transfusion rate), only two (10.5%) patients needed transfusion.
Considering the limitations of this initial series, it should be emphasized that in our center, we usually do not perform a selective vascular study before renal-sparing operations. As a consequence, before the procedure, no consideration is given to whether selective clamping of the posterior segmental artery or one of its branches will be adequate to achieve optimal vascular control (the tumor may in any case receive irrigation from other arterial territories). Furthermore, we are unaware of the extension of the ischemia resulting from ligature of tertiary arteries. We attempted to overcome these possible handicaps by always placing a safety tourniquet at the level of the main artery (whose fastening was necessary in only three of the cases) and by performing only selective ligature of the small-caliber direct branches to the tumor in three cases.
On the other hand, it should be stated that while the retroperitoneoscopic approach offers an obvious advantage in dissection of the vascular pedicle, the suture of the parenchyma is particularly complex and demanding. Thus, the use of hemostatic agents and tricks such as the exchange of ports between the scope and one of the surgeon's instruments to facilitate triangulation (depending on the tumor location) are of critical value in this approach.
A further handicap of the present work is that in our series, we did not combine the selective vascular dissection with pharmacologically induced hypotension as described by Gill and associates. 9 This aspect could be considered in future procedures and might further improve our results. Future prospective randomized studies comparing off-clamp laparoscopic transperitoneal and retroperitoneal PN would also be of relevance.
A final limitation of the present study is that follow-up renal function at 6 months was available in fewer than half of the cases (seven patients), which limits our conclusions on the real impact of the technique on renal function. Nonetheless, mean serum creatinine levels and estimated glomerular filtration rate (Modification of Diet in Renal Disease formula) altered from 86 to 94 μmol/L and from 77 to 70 mL/min/1.73 m2, respectively.
Conclusions
Consensus guidelines recommend nephron-sparing surgery in T1 renal tumors. The WIT may affect renal function after the procedure. The retroperitoneoscopic approach permits direct access and straightforward dissection of the renal artery and its posterior branch, often the exclusive arterial supply to the posterior renal surface. According to our initial series, the retroperitoneoscopic approach combined with enucleation may allow off-clamp excision of tumors of the posterior kidney with a relatively short learning curve, thus avoiding ischemia of healthy tissue. Further studies are needed to confirm these preliminary results, which could pave the way for real zero ischemia nephron-sparing procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.