
Abstract
Background and Purpose:
Digital Light Processing hyperspectral imaging (HsI) produces a highly sensitive, real-time tissue oxygenation map to monitor renal perfusion/oxygenation during partial nephrectomy (PN). Our initial experience with HsI revealed considerable variation in the baseline renal oxygenation, and we sought to correlate these differences with postoperative renal function.
Patients and Methods:
Hyperspectral images were collected intraoperatively in patients undergoing PN for cortical tumors. The kidney was illuminated with visible light (520–645 nm), the spectrum corresponding to that of oxyhemoglobin. Reflectance images were captured and digitally processed to determine the percentage of oxyhemoglobin (HbO2) at each image pixel. Images were taken before hilar occlusion; these %HbO2 values were used to categorize patients as high (>75% HbO2) or low (<75% HbO2) oxygenation, and postoperative eGFR was assessed.
Results:
There were 26 patients who underwent PN with ice cooling and HsI imaging. Nineteen patients had a “low” preclamp oxygenation (mean 69%) while the other 7 had a “high” HbO2 (mean 77%). There was no difference in tumor size, hematocrit value, clamp time, or preoperative eGFR between the two groups. Patients with a higher baseline %HbO2 had no significant postoperative change in their eGFR (mean 0 mL/min/1.73m2, +4%), while those with the lower baseline %HbO2 had a significant acute decline (mean 15 mL/min/1.73m2, −20%, P=0.02, 0.006).
Conclusions:
Baseline renal oxygenation, as measured with HsI, may help predict risk of postoperative renal insufficiency and may distinguish between patients with otherwise similar baseline characteristics, such as eGFR. HsI may provide individualized assessment of renal function to influence intraoperative decision-making to help preserve renal function.
Introduction
We have recently begun using a technology called hyperspectral imaging (HsI) to measure oxyhemoglobin (HbO2) during kidney surgery in both humans and a porcine model. 6 –8 This technology uses a programmable DLP® (Digital Light Processing, Texas Instruments, Dallas, TX) spectral illuminator and a highly sensitive camera to detect the visible spectral properties of oxyhemoglobin and deoxyhemoglobin, generating a real-time image of cortical tissue oxygenation and thereby parenchymal perfusion. We have used HsI to assess the degree and rate of hemoglobin desaturation of the human kidney during open partial nephrectomy 7 as well as to demonstrate that differences in hilar occlusion technique affect renal oxygenation and function in a porcine model. 6,8
While reviewing hyperspectral images of human kidneys undergoing PN, 7 we noted substantial variation in the percentage of oxyhemoglobin (%HbO2) between kidneys before any renal vasculature occlusion and tumor excision. We hypothesized that these variations in hemoglobin saturation reflect baseline renal perfusion and may reflect susceptibility to ischemic injury. We studied whether noninvasive, noncontact HsI assessment of baseline renal %HbO2 could predict susceptibility to ischemic injury as reflected by acute postoperative renal functional recovery in patients undergoing PN.
Patients and Methods
With Institutional Review Board approval, HsI was used in consenting patients undergoing open PN for renal cortical tumors. All kidneys were accessed via a flank incision, and ice slush was used to cool the kidney during the ischemic interval. As previously reported, 7 after the kidney had been adequately mobilized and the hilum isolated, an HsI camera was used to capture baseline %HbO2 maps of the kidney. Both the artery and the vein were clamped during the PN and HsI images periodically obtained during the procedure. Data such as patient age, sex, race, tumor size, ischemia time, and laboratory values such as creatinine and hematocrit were recorded.
Our technique for obtaining hyperspectral images of the kidney has been described previously. 6 –8 Integration of DLP technology with currently available HsI systems significantly speeds image acquisition and processing time to less than 30 seconds using conventional 126 successive band-passes of light. 6 DLP chips are optical semiconductors that contain an array of potentially millions of tiny micromirrors that can each move independently to reflect a complex, high-quality image, controlled electronically. While this technology sounds complex, it is already used commercially in many familiar products, including most digital cinema projectors. Non-DLP HSI systems rely on technology that requires at least 40 seconds to capture and project images. 9,10 Furthermore, the active spectral illumination capability of the DLP hyperspectral camera requires the acquisition of only three spectral illumination images (“three-shot mode”), further shortening the time for producing chemically encoded images to a rapid three to four frames per second. 6,10
The DLP HsI camera is tripod-mounted and illuminates the kidney from a fixed distance with a known spectrum of wavelengths between 520 nm and 645 nm. 6 These spectra incorporate the reflectance values of both oxyhemoglobin and deoxyhemoglobin. Reflectance images are then captured by a charge-coupled device (CCD) focal plane array, and the data are formatted into a three-dimensional cube consisting of a spectral wavelength assessment and a two-dimensional spatial image. Collected data are then deconvoluted to assess numerical %HbO2. The relative percent contributions of both oxyhemoglobin and deoxyhemoglobin are color-encoded, with various colors representing the relative %HbO2 as seen in Figure 1. 10,11
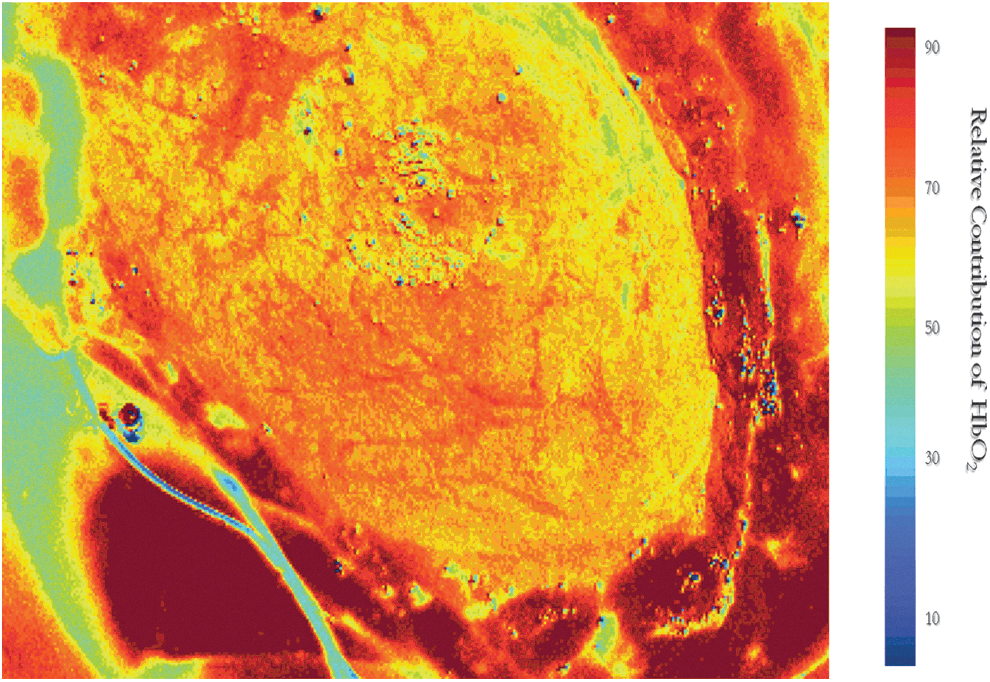
Renal hemoglobin oxygenation color encoded as the percentage of oxyhemoglobin (%HbO2) detected by hyperspectral imaging. As indicated by the color bar, right, a darker maroon represents high values for %HbO2 while the lighter yellows and greens indicate lower values.
From the oxymetric visualization an “optical biopsy” area consisting of a 10×10 pixel square is sampled from the center of the kidney image and assessed analytically. Briefly, the relative percent contribution of each component (oxyhemoglobin and deoxyhemoglobin) is determined at each detector pixel by use of a multivariate least squares regression. While such assessment is similar to pulse oximetry, HsI is fundamentally different in that it samples the organ of interest as a whole at the microvascular (parenchyma) level and directly measures oxyhemoglobin saturation.
Estimated glomerular filtration rate (eGFR) was calculated using the Modification of Diet in Renal Disease study equation and was compared between the most recent preoperative value and that of postoperative day 2. eGFR was also calculated at the most recent follow-up visit. Statistical comparison was performed with Microsoft Excel® using a two-tailed, two-sample t test, after confirming the eGFR data was normally distributed.
Results
Twenty-six patients underwent open PN with cold ischemia and assessment of %HbO2 with HsI. Mean patient age was 59 years, and mean tumor size was 3.8 cm. Fifteen (58%) patients were male. Mean renal cortex baseline (before hilar occlusion) %HbO2 was 71.1%. Of the 26 patients, 7 were found to have a baseline %HbO2 above 75% (mean 77.1%). The average %HbO2 of these 7 patients was significantly higher than that of the other 19 patients (mean 68.9%, P=0.0001). Other parameters concerning these patients, such as age, tumor size, preoperative hematocrit, preoperative GFR, ischemia time, and estimated blood loss, were not significantly different between the two groups (P>0.05, Table 1).
Reported as means.
HbO2=oxyhemoglobin; GFR=glomerular filtration rate; HCT=hematocrit; POD=postoperative day.
Despite these similarities between the two groups, when the change in eGFR between baseline and postoperative day 2 was calculated (both absolute change and percent change), renal functional outcomes appeared significantly better in the patients with the higher baseline %HbO2 (P=0.02 and 0.006, respectively). Patients with a higher baseline %HbO2 appeared to have no significant change in their eGFR (mean 0 mL/min/1.73m2, +4%), while those with the lower baseline %HbO2 had a significant acute decline in their eGFR (mean −15 mL/min/1.73m2, −20%). This difference was no longer statistically significant at the most recent follow-up (mean 179 days, P=0.46)
Discussion
As an imaging technology using light from the visible spectrum, HsI is a noninvasive, safe tool that can measure %HbO2 and thereby assess microvascular tissue perfusion. While renal injury and CKD risk-stratification systems use factors such as the presence of hypertension and diabetes (diseases thought to create end-organ microvascular disease), 4,5 interpersonal variation may reduce the reliability of the scoring system when applied on the individual level. For example, one patient may have mild, well-controlled hypertension while another may have poorly controlled disease, yet they would receive the same score in these stratification systems.
An intraoperative real-time technology such as a DLP HsI camera able to predict renal susceptibility to ischemic injury and acute renal functional recovery would avoid these inaccuracies and objectively report the actual individual kidney risk. Specifically, we hypothesized that a lower renal %HbO2 at baseline (preocclusion) may reflect microvascular disease such that more oxygen is disassociated from the hemoglobin molecule to meet cellular requirements. The inferred poorer perfusion in these kidneys would then make them more susceptible to ischemic insult. If true, intraoperative DLP HsI measures of %HbO2 before hilar occlusion may allow the surgeon to individually tailor or modify the procedure to maximize renal protection.
In our study, the HsI-determined measure of renal cortical %HbO2 taken before vascular occlusion did correlate with a patient's acute postoperative eGFR decline. Even when other factors that might be expected to influence postoperative renal function were considered, such as patient age, tumor size, and ischemia time, baseline %HbO2 predicted the kidney's tolerance of prolonged ischemia (mean>30 min in both groups in this study) and its acute functional recovery. Such real time recognition of this measure may allow surgeons to modify their surgical technique to maximize renal preservation. Possible maneuvers include artery-only occlusion, early unclamping of the hilar vessels, superselective arterial branch occlusion, or zero-ischemia techniques.
While review of available eGFR data suggests that the eGFR difference resolved within the first few months postoperatively, we have limited follow-up data on these patients, because of the novelty of this technology. Furthermore, because all patients had a normal contralateral kidney wherein compensatory filtration is expected in the short term, the improvement in eGFR was not unexpected. We believe the immediate (postoperative day 2) change in eGFR more accurately reflects the degree of ipsilateral renal injury before the contralateral compensatory response. It stands to reason that whatever predisposed these patients to experience greater acute kidney injury (presumably, microvascular disease resulting in decreased cortical perfusion as reflected by the greater disassociation of oxygen from circulating hemoglobin) may also place them at higher risk for later decline in GFR, although it remains to be determined.
Certainly the literature suggests that patients who have even a minor and transient insult to their kidney function, such as from myocardial infarction, are at higher risk for later development of CKD and even death. 12 –14 Longer follow-up of a larger cohort will help clarify whether renal cortical percent HbO2 saturation will predict this risk.
Interestingly, as described by Holzer and associates, 7 the relative drop in %HbO2 after hilar occlusion is immediate and consistent for all kidneys and not predictive of eGFR (data not presented). In that investigation, our group found that the %HbO2 dropped 20% on hilar clamping and reached nadir quickly within the ice slush cooling period in all kidneys, regardless of preocclusion baseline %Hb02. Further work to assess whether a specific nadir %HbO2 during the ischemic interval explains or contributes to the greater decline in eGFR experienced by patients with lower preocclusion %HbO2 is needed and the subject of future work.
Our study certainly has several limitations. First, this is the first investigational use of this technology. While HsI technology has a long history of use in astronomy, mineralogy, agriculture, and even military surveillance, its application in medicine is relatively recent. The development of rapid image acquisition HsI technology (DLP-based camera), as reported in this article, is particularly new and important for many medical applications. Second, the DLP HsI camera we used is tripod-mounted and, as such, only applicable to open surgery. Work is under way to develop a system capable of providing images during laparoscopic or robot-assisted surgery, which will be important as use of minimally invasive PN increases.
Third, we have limited follow-up on patients whose kidneys were imaged with HsI, as well as a limited overall sample size. We, like many investigators, used eGFR for our comparison of renal function, and there may be certain inaccuracies inherent to the use of these types of formulaic estimations. Finally, while we attempted to identify factors other than renal perfusion that might influence postoperative renal function, such as patient age, tumor size, ischemia time, and preoperative renal function, there may exist other factors that could explain the differences seen between our two patient groups. These data represent our initial experience, and these findings will help us steer our efforts using this technology. With further patient recruitment, we plan to perform a multivariate analysis to better elucidate the relative contribution of baseline %HbO2 in predicting postoperative renal function recovery.
Conclusion
HsI may provide a powerful tool for noninvasive, individualized intraoperative assessment of a patient's risk for postoperative decline in renal function after open PN. Use of this technology may allow surgeons to modify their surgical technique to maximize renal preservation in patients found to be at higher risk for deterioration.
Footnotes
Disclosure Statement
K. Zuzak is a patent inventor for hyperspectral imager and received grant support from Texas Instruments, Inc. For the remaining authors, no competing financial interests exist.