
Abstract
Background and Purpose:
Surgical outcomes depend on patient and disease-related factors, as well as the technical skill of the surgeon. Various distractions in the operating room (OR) environment have been shown to negatively impact a surgeon's performance. A survey was conducted with the objective to evaluate and characterize distractions during urologic surgery.
Methods:
An Internet-based survey was distributed to 2057 international urologists via email between April and October 2011; questions focused on a variety of disruptive factors postulated to have a negative impact on surgical performance.
Results:
Of the 523 (25%) respondents, 58% practiced in North America, 42% were from an academic institution, and 68% had completed a clinical fellowship. In an average year, 83% reported having operated at least once while sleep deprived, 84% when significantly ill, 55% with a musculoskeletal injury, and 65% under significant social stress. Up to 38% reported that on at least one occasion, such “internal distractions” had significantly affected surgical performance and 14% perceived that at least one surgical complication was caused mainly by an internal distraction. Less than 50% had ever cancelled surgery because of an internal distraction. Music was routinely played in the OR by 57% of respondents, >67% reported answering pages and discussing consults while operating, and 25% reported “commonly” working with scrub nurses/techs that were unfamiliar with the procedure and/or instruments. Only 44% had consistent individual(s) assisting, and 27% reported that the scrub nurse/tech would “commonly” scrub out during a critical portion of the procedure. Overall, 14.5% reported that at least one complication had occurred mainly because of such “external” or “interactive” distractions.
Conclusions:
Urologists face various distractions in the OR that can negatively impact surgical performance, potentially compromising patient outcomes and safety. Further studies are needed to elucidate the true impact of such distractions and to develop strategies to mitigate their effects.
Introduction
The operating room (OR) environment may seem quite different from that of an inpatient medical ward when taken at face value; however, both clinical settings involve the coordinated and cohesive efforts of several allied healthcare providers, a reliance on and understanding of certain individual competencies, a wide spectrum of patients and disease entities, and a dynamic environment that can change from calm to calamity within a short time.
The OR environment often necessitates faster decision-making and more efficient checks and balances vs an inpatient ward, creating the perfect milieu for adverse events. In addition to the already high-stakes, high-paced environment of the OR setting, distractions that deleteriously affect individual performances or systems-based protocols can have a significant impact on patient care outcomes. Studies specifically looking at adverse events in surgery have noted that up to 50% of events are highly preventable. 2,3 As such, it behooves us to carefully examine the various factors that may promote a working environment conducive to adverse surgical events.
To better understand the prevalence or scope of such distractions, we conducted a survey study to evaluate and characterize the current OR working environment among contemporary urologists.
Methods
An Internet-based survey was distributed to 2057 international urologists in June 2011. The survey was distributed via e-mail through the Endourological Society and the Canadian Urological Association membership lists. The survey consisted of 6 questions each on demographic data and clinical practice details, followed by 36 questions focused on various factors that have been theorized or demonstrated to have a negative impact on surgical performance of either cognitive and/or psychomotor skills. Urologists were able to anonymously provide responses through the Internet-based Web site, and Internet Protocol addresses were collected only to eliminate multiple responses from the same person.
Results
Respondent demographics
A total of 523 urologists responded to and completed the online survey (25% response rate). The international cohort of respondents consisted of 58% from North America, 23% from Europe, 8% from Asia, and another 10% from either Australia/New Zealand, South America, or Africa (Fig. 1). The majority of urologists worked at an academic institution, either full-time (42%) or as part of a combined academic and private/community practice (20%). Most were between the ages of 35 and 55 years (72%), male (93%), and had completed a clinical fellowship (68%). Forty-one percent of survey respondents had a predominantly “general urology” practice, while 27% saw mainly uro-oncology patients, 16% endourology patients, 4% female or reconstructive urology patients, 3% pediatric urology patients, and 1% infertility patients. Most urologists (70%) had an average of one to two OR days per week, and 50% reported operating at more than one hospital.
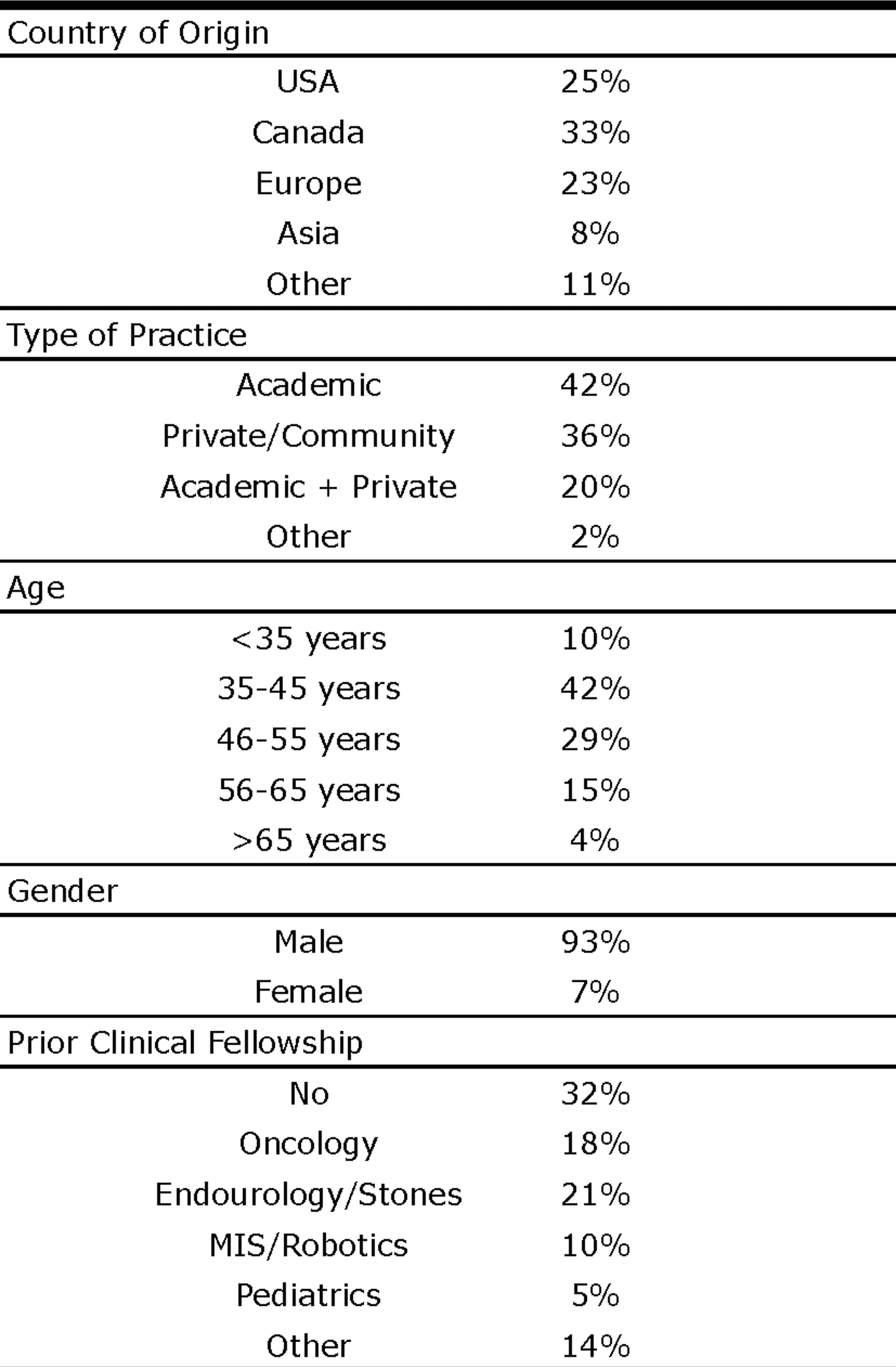
Demographic data of survey respondents. MIS=minimally invasive surgery.
Distractions
Over the course of an average year, 83% of respondents reported operating while sleep deprived (defined as <6 hours of sleep the night before) on at least one occasion. Of these urologists, approximately one in five reported that this occurred in >20% of cases. Interestingly, 19% of urologists reported that sleep deprivation had significantly affected their performance in the OR (“significantly affected” defined as slower operative times, complications, or the need to scrub out), but 80% of them reported that they had never cancelled an OR case because of fatigue (Fig. 2).

Internal distractions with potential impact on operating room performance. MSK=musculoskeletal.
In an average year, 84% reported having operated at least once while feeling unwell (cold, flu, nausea/vomiting, diarrhea, etc). While 38% of urologists reported that an illness had significantly affected their OR performance (Fig. 2), only half of them had ever cancelled an OR day because of illness.
Fifty-five percent reported having operated at least once with a significant musculoskeletal (MSK) injury (broken bone, pulled muscle, strained ligament, chronic back pain) in any given year, with 27% stating that the MSK injury significantly affected OR performance. Of the urologists who have operated with a significant MSK injury, only 27% had ever cancelled an OR day because of the injury.
Operating at least once while under significant social stress (severely ill child/spouse, domestic problems, financial problems, depression, etc) was reported by 65% of urologists, 27% of whom stated that it negatively affected performance in the OR. Only 23% of respondents had ever cancelled an OR day because of significant social stress.
With respect to environmental factors (external distractions) that may affect OR performance, 57% reported listening to music routinely in the OR, 68% routinely answered pages while operating, 72% commonly discussed consults with trainees while in the OR, and 54% reported being distracted routinely by loud talking between the scrub team and circulating nurses.
When asked specifically about preventable intraoperative complications, 13% of respondents believed that at least one surgical adverse event had been caused mainly by an internal distraction (fatigue, illness, injury, stress) while 15% thought that at least one surgical complication had occurred mainly because of an external distraction (music, pager, discussing consults, loud talking in OR, etc).
Distractions relating to the interaction between healthcare providers also seemed common. Fewer than half of respondents (47%) worked with a dedicated urology OR scrub team and 25% reported that it was common to work with a scrub nurse who was neither familiar with the surgical procedure nor the technique/instruments used. While 40% of urologists reported that it never or rarely happened, 27% reported that it was common for the main scrub nurse/tech to change shifts or take a break during the most critical portion of the surgery (Fig. 3). Seventy percent (70%) of urologists had never before participated in a “team-based” OR training event, and 81% believed changes to their current working environment in the OR were needed to improve their ability to concentrate during surgery.

Interactive distractions with potential impact on OR performance.
Routine performance of a preoperative “time-out” was reported by 89% of respondents with patient identification (91%), proposed surgical procedure (94%), and side/location of surgery (87%) being the most commonly discussed items. Among urologists who routinely performed preoperative time-outs, only 4% reported any discussion of internal distractions that may affect OR performance (surgeon fatigue, illness, MSK injury, social stress), while only 5% mentioned any discussion of other external or interactive factors that could potentially affect OR performance.
Discussion
Surgeons have often been compared to airline pilots and the surgical field equated to the aviation industry. Both require a team of highly trained individuals, working together in a high-stakes environment in which the ultimate goal is to use cutting-edge technologic equipment to ensure that passengers/patients arrive safely at their destination—be it another country or the recovery room.
A core difference exists between the two industries, however, that may explain major differences in industry policies with respect to the way adverse events are approached, managed, and studied; pilots are also passengers on the very airplanes they fly. Disasters in the aviation industry are relatively rare, but surgical complications are common. This is partly a result of the many “quality control” mechanisms that are in place in the aviation industry, where accidents, adverse events, and even near misses are systematically scrutinized. In contrast, surgical morbidity and mortality rounds and patient safety systems are often deficient. 4,5 lacking the exhaustive attention to detail seen in the aviation industry.
In addition to the rigorous evaluation of adverse events, the aviation industry also takes great care in ensuring pilots are well prepared and that they have the best chance to succeed in delivering their precious cargo. Before licensing, all pilots are required to log a minimum number of hours on validated flight simulators. While further in-flight training does occur, simulation-based training is a core principle in the instruction and certification of many pilots. Although the effect of mistakes during flight and surgery differ tremendously, the complexity of surgery may exceed that seen during flight and the number of unexpected, unsimulatable situations is far greater during surgery. In contrast to flight, there is no “autopilot” for surgery. Surgical training does not follow a similar model of certification as flight training, and implementation of surgical simulation has been slow. For example, while the da Vinci surgical robot was introduced into clinical practice more than a decade ago, only recently has there been a movement toward implementing simulation-based training for robot-assisted surgery certification. 6 –10
Maximum daily flight hour regulations, minimum preflight rest period requirements, and preflight alcohol consumption policies 11 are strictly enforced in the aviation industry; however, no similar regulations apply to faculty surgeons. While OR systems-based policies, such as the preoperative surgical checklist, have been successfully implemented, 12 regulations aimed at the individual level have not been as commonplace. Literature documenting the physiologic changes associated with sleep deprivation and the deleterious effects of fatigue on decision-making 13 –16 and surgical performance are emerging. 17 –20
Rothschild and colleagues 18 compared 3552 surgical and 3945 obstetric control procedures with a total of 919 surgical and 957 obstetric procedures performed after the physician had been awake overnight, performing other procedure(s). The authors demonstrated an increased rate of complications among postnighttime surgical procedures performed by physicians with sleep opportunities of less than 6 hours (6.2% vs 3.4%, odds ratio 1.72, 95% confidence interval 1.02–2.89). Literature has also emerged demonstrating the negative effects of drinking modest amounts of alcohol before surgery, not only immediately before, but even the night before. 21 –23 In addition to this growing body of literature, and despite what seems to be common sense, most regulation bodies do not have any explicit policies in place limiting the consumption of alcohol before surgery.
Recently, several studies have looked at the impact of distractions on surgical performance and patient safety. 24 –26 Commensurate with literature in the aviation industry, 27,28 Persoon and associates 26 demonstrated the deleterious effects of distractions during the performance of endourologic skills. They found that trainees completing three separate endourologic tasks while being required to answer questions about a clinical case that had been presented before the hands-on training performed significantly worse than those who did not have to deal with such cognitive distractions. Interestingly, fewer than 10% of trainees in the distraction group noticed the burden of the distraction.
Our survey study demonstrates that various internal, external, and interactive factors may act as distractions, negatively impacting surgical performance and perhaps even patient safety. What is worrisome is not the mere fact that these distractions are more prevalent than most would believe, but that they are not resulting in the appropriate reactions required to improve patient safety. While one of three urologists admitted that sleep deprivation had significantly affected surgical performance during an operative case and 13% had attributed at least one intraoperative complication directly to an internal distraction, only 20% of respondents had ever cancelled surgery because of such distractions. While clinical demands and resource limitations may not make it feasible for surgeons to cancel surgical procedures routinely, it behooves us to study further the various factors that may negatively impact surgical performance and search for methods of mitigating such effects.
More than one-quarter of study participants reported that it was common for the main scrub nurse/tech to change shifts or take a break during the most critical portion of the surgery. This highlights the importance of communication between the surgeon and the rest of the operative team to note critical steps during a procedure (for example, during clamp time for a partial nephrectomy) to help minimize external distractors that may disrupt the surgeon's concentration and the flow of the surgical procedure. There are potential distractors, however, that are out of the surgeon's control (ie, pages, telephone calls into the operating room, etc).
This study has several limitations. First, there may be a significant self-selection bias because urologists who chose to respond to the survey may be very different from those who chose not to respond. Second, the survey was distributed only in an electronic format, which limits the population sampled to those with e-mail and Internet access. Third, many questions involved the use of a “strength-of-choice” response scale (eg, never, rarely, sometimes, always), which can lead to very subjective and vague data sets. Finally, several of the questions may introduce recall bias (eg, In any given year, roughly how many times have you operated while feeling unwell?), potentially compromising the validity of the data set. The true incidence of the various distractive factors is unknown, because data were not collected prospectively, and the relative importance of each factor has yet to be studied.
Conclusions
Urologists face various forms of distractions while in the OR, many of which may negatively impact their surgical performance, potentially compromising outcomes and patient safety. Evaluation of surgeon-related distractions and optimization of the surgical environment are timely topics of discussion as we move toward the delivery of optimized patient care. Further studies are needed to better elucidate the true incidence and impact of such negative distractions and to develop strategies that may mitigate their effects, both at the individual and systems-based levels.
Disclosure Statement
No competing financial interests exist.
Footnotes
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.