
Abstract
Background and Purpose:
Ascertaining the optimal depth of dilator progression is a crucial factor during tract dilation in percutaneous nephrolithotomy. Dilation is generally guided under fluoroscopy, ultrasonography, or combination of both techniques, and it is still difficult to prevent overdilation causing perforation and vascular injury or underdilation causing difficulty in establishment of access. Thus, improvements in dilation technique bears clinical significance. Our aim was to evaluate the feasibility in an animal model of using the “visual dilator system” for optimal percutaneous tract dilation under real-time visual guidance.
Materials and Methods:
The visual dilator system consisted of a transparent hollow dilator made of polyvinyl chloride and a rigid ureteroscope inserted within its lumen. The ureteroscope was connected to a standard endoscopic camera system. The dilator system backloaded with an access sheath was passed over a guidewire to dilate the tract and position the access sheath under visual guidance. Saline was used as irrigation to maintain clarity during dilation. The dilation technique was implemented to establish percutaneous access tract in six PCNL simulator models made from fresh porcine kidney placed inside an eviscerated chicken carcass and four female swine (eight kidneys) to experimentally evaluate its feasibility and efficacy.
Results:
All tracts were successfully established with dilation through the intervening tissue layers, approach into the target calix, as well as access sheath placement being visually monitored through the dilator wall to confirm accuracy. All procedures were free of dilation-related complications such as collecting system perforation, excessive bleeding (in-vivo model), or loss of access. The limited number of animal models and lack of randomized comparative study with other dilator modalities were major drawbacks of the study.
Conclusions:
The study demonstrates feasibility of precutaneous access tract dilation using a Visual dilator system. This technique can provide visual confirmation of accuracy in dilation to improve safety and efficacy of the procedure.
Introduction
Access to the renal collecting system can be achieved under guidance of fluoroscopy, Ultrasonography (US), or a combined method. US provides quick, accurate, and radiation-free guidance during initial puncture. 3,5 During tract dilation in complete US-guided PCNL, however, the echogenicity of the guidewire and the dilator may not be good enough to accurately monitor the dilator progression into the target calyx. 6,7 This increases the chances of overadvancement of the dilator or access sheath into the collecting system, which leads to related complications such as collecting system perforation, hemorrhage, and extravagation. In addition, because of kidney hypermobility with the patient in the supine or semisupine position and kidney displacement from longitudinal force applied during use of Amplatz or Alken type dilators, underdilation makes successful establishment of the access tract in a single attempt strenuous.
In this study, we describe and evaluate the initial feasibility of using the novel “visual dilator system” for real-time, on-board visual monitoring of percutaneous access dilation.
Materials and Methods
Design and settings
The “visual dilator system” consists of a transparent hollow dilator made of polyvinyl chloride (China Medical Device Industry Co. Ltd., Zhang jiang, China) and a 8/9.8F rigid ureteroscope (Wolf Co., Knittlingen, Germany) which can be inserted into the dilator's hollow shaft and positioned at its conical tapered end. The ureteroscope is connected to a standard endoscopic camera system and light source. During dilation, the working guidewire can be inserted through a 1-mm opening located at the dilator tip and along the working channel of the ureteroscope. The irrigation system (laparo pump 2215, Wolf, Knittlingen, Germany) is used to move saline through the working channel of the scope to maintain optimum clarity of vision during dilation (Fig. 1). The dilator system is backloaded with an Amplatz peel-away sheath for positioning into the target calix under visual guidance after confirmation of optimal dilation. The specification of the transparent dilator is given in Table 1.
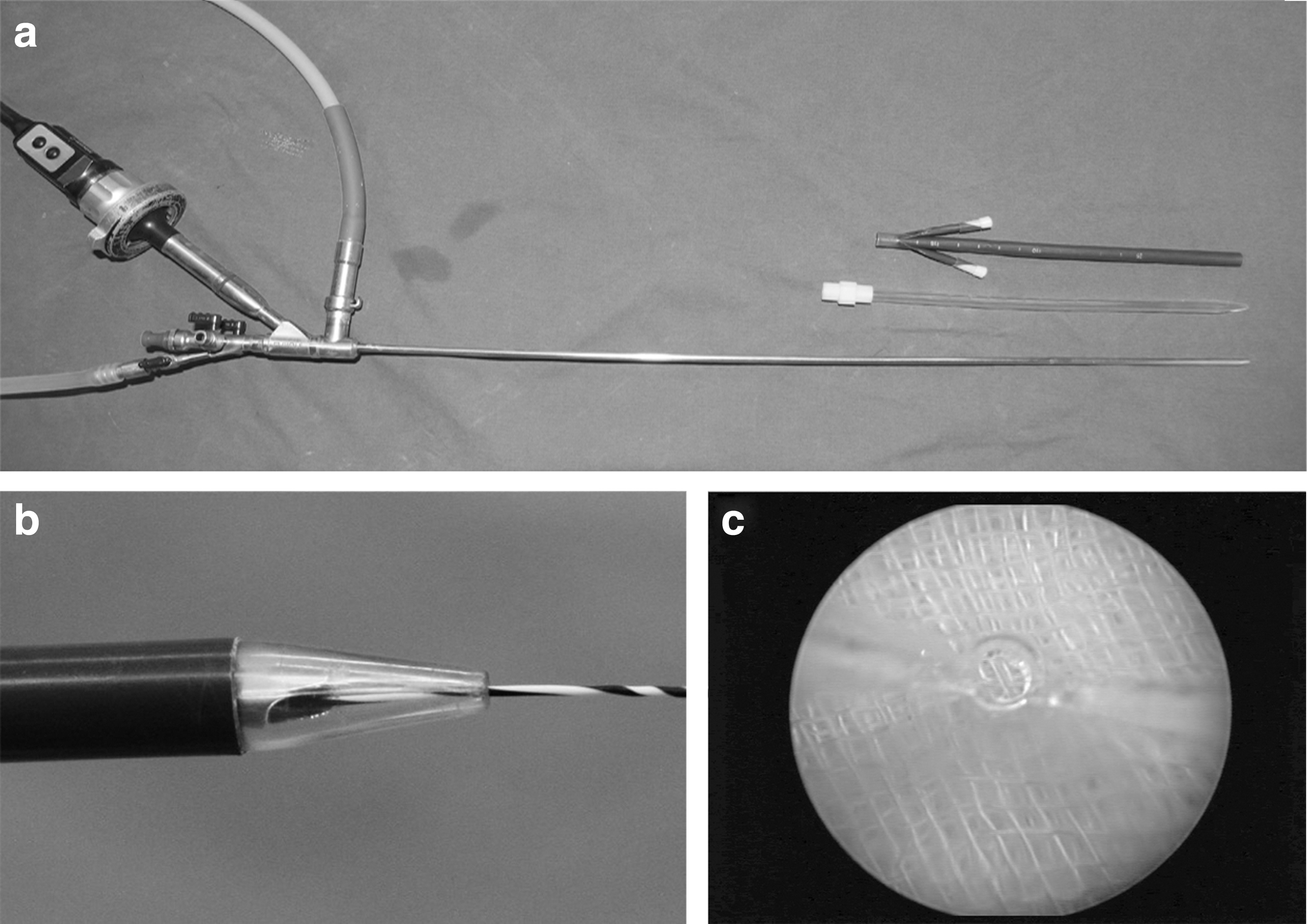
The visual dilator system.
Assessment of visibility
To ascertain the quality of visibility through the visual dilator system, the conical tapered tip of the dilator system was positioned at about 1 cm from a cotton gauze piece immersed in a tray containing saline. The knitting pattern of the gauze piece was visualized through different portions of the dilator tip wall to check out any distortion of the image and narrowing of the field of vision so obtained.
Test in ex-vivo animal model
The feasibility of the visual dilator system in dilation of the percutaneous access tract was initially tested in six biologic training models as described by Häcker and associates. 8
Fresh porcine kidneys including the ureter (4–5 cm length) were obtained from a commercial slaughterhouse. An open end ureteral catheter (5F) was inserted into the renal pelvis through the ureter and fixed with silk suture. To simulate the different tissue layers in human, the prepared porcine kidney was placed inside an eviscerated chicken carcass (obtained from a supermarket) and fixed within so that the plane of the calices aligned along the flank region of the chicken carcass.
The prepared model was placed in a flat tray in a lateral position and fixed externally to avoid any displacement of the model during the procedure (Fig. 2a). Then, 50 mL saline was perfused into the renal pelvis through the ureteral catheter to create hydronephrosis. US-guided puncture was made between the costal margin and lower extremities of the chicken using the standard 18-gauge two-part trocar needle through a needle guide system attached to 3.5-MHz probe (Aloka Ultrasound System, Tokyo, Japan). During this step, the distance between puncture-site and renal capsule was measured to ascertain the depth of fascial dilation needed before use of the visual dilator system.
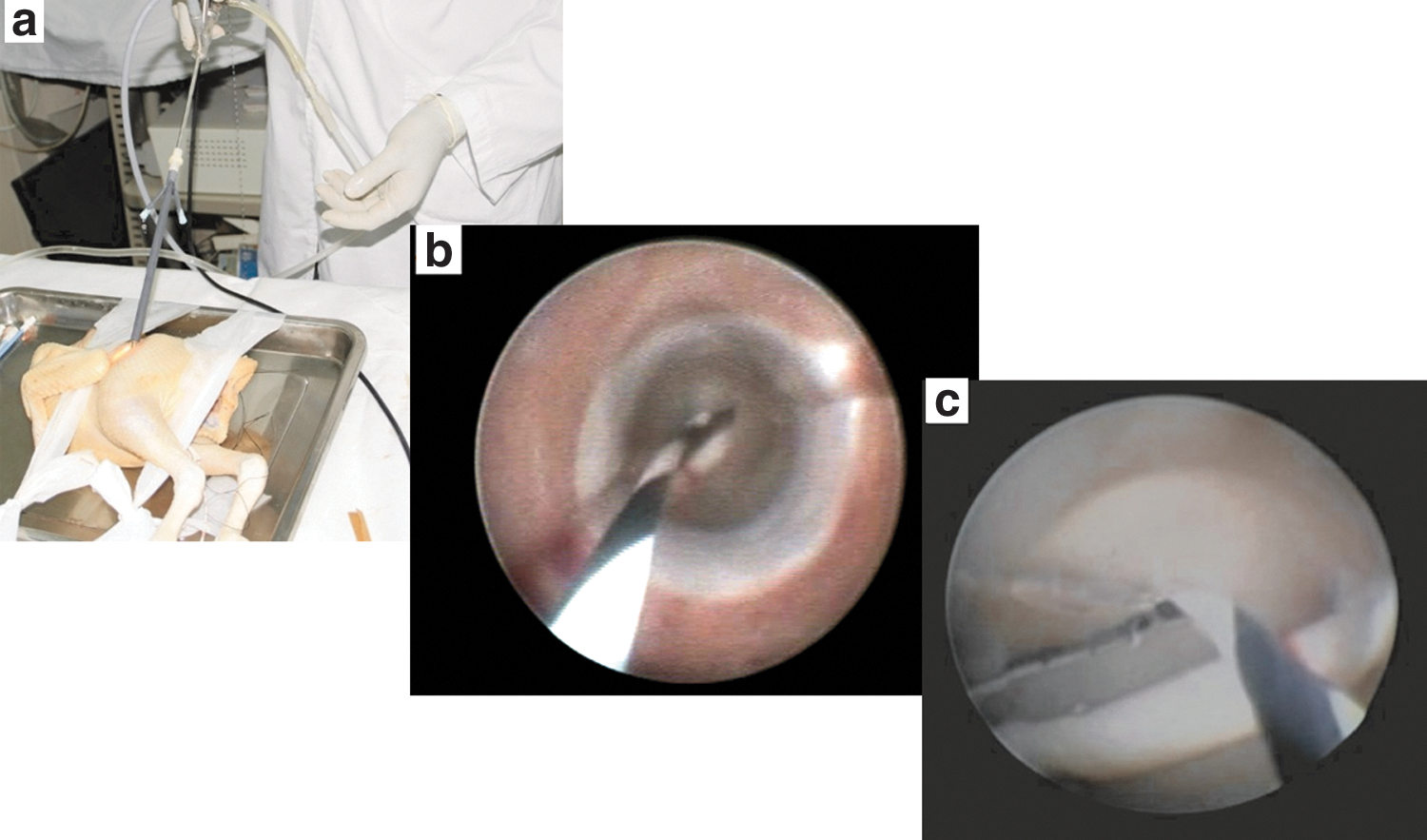
Test in ex-vivo animal model.
After the accuracy of puncture was confirmed from the backflow of saline through the needle, a 0.032-inch (0.81-mm) Nitinol guidewire (OptiMed Medizinische Insturmente GmbH, Ettlingen, Germany) was introduced into the renal pelvis. Then 10F, 16F, and 22F Amplatz dilators (ADs) were sequentially passed to dilate the subcutaneous tissue and muscle layers of the chicken carcass. The visual dilator system backloaded with a 22F Amplatz sheath was then passed over the guidewire with clockwise rotation of the dilator to dilate through the renal parenchyma into the targeted calyx in one step, while holding the scope in the nondominant hand.
After confirmation of successful dilation, the Amplatz sheath was visually guided into the collecting system, and the dilator was removed (Fig. 3). Nephroscopy was performed through the sheath to thoroughly examine all portions of the pelvicaliceal system and rule out any parenchymal laceration or perforation induced during the procedure.

Diagramatic representation of dilation steps using the visual dilator system.
Test in in-vivo animal models
After the successful trial of the visual dilator system in an ex-vivo animal model, we used the dilator system to dilate the nephrostomy tract in eight kidneys of four female farm swine with an average weight of 25 kg. We selected female farm swine in this experimental study to facilitate the retrograde placement of the ureteral catheter and to create a model similar to humans. All procedures were performed under general anesthesia.
With swine in the lateral position, bilateral ureters were catheterized using an open-ended 5F catheter under direct cystoscopy and were secured to a 14F Foley catheter that was placed inside the bladder. The subsequent procedural steps of puncture and dilation were similar as explained above in the ex-vivo animal model (Fig. 4).
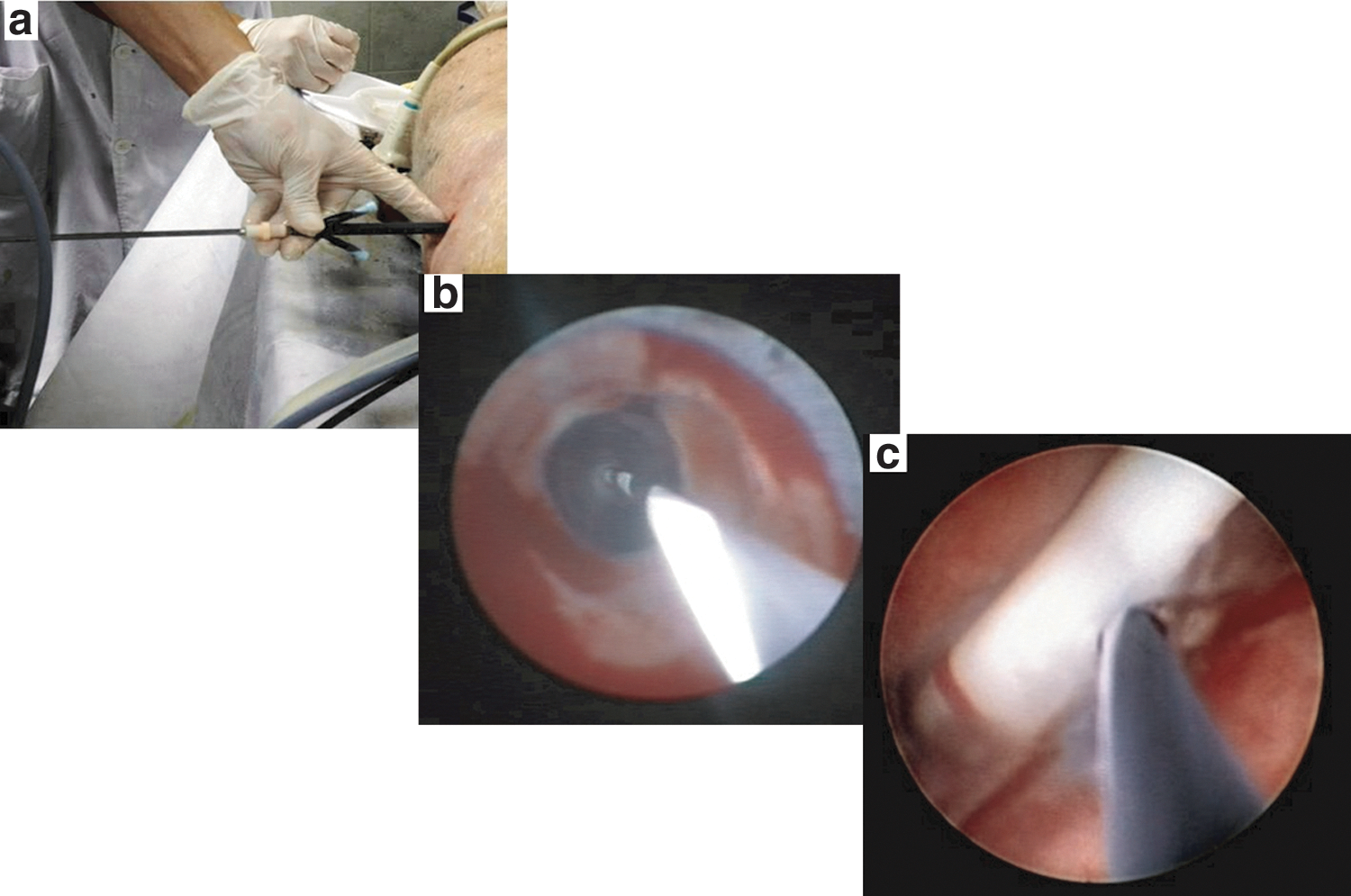
Test in in-vivo animal model.
A similar procedure was performed on the contralateral kidney of the animal. At the end of the experiment, the animal was euthanized by injecting air into the venous system. The dilation time, defined as the time from guidewire insertion to positioning of the working sheath, was recorded for all procedure in both ex-vivo and in-vivo animal models.
Results
During visual assessment of the visual dilator, the pattern of gauze could be clearly observed through different parts of the dilator wall. No significant distortion of the image or narrowing in the field of vision was found (Fig. 1c).
An access tract was established in all in-vivo and ex-vivo animal models with good position in a single attempt. During the dilation process, the dilator passage through the extrarenal tissue layers, renal parenchyma, entry into the target renal calyx, and finally positioning of the Amplatz sheath could be clearly visualized in real time through the dilator wall (Fig. 2b, 2c, 4b, 4c). Entry into the renal pelvis could be confirmed by vision of the pelvicaliceal wall or indwelling ureteral catheter. Initial nephroscopy through the access sheath confirmed optimal dilation and minimal bleeding (in the in-vivo model). No pelvicaliceal system injury was recorded in any of the procedures. The average dilation time in ex-vivo was 6 minutes (range 7.4–5.2 min) and in in-vivo animal models, it was 6.3 minutes (range 8.1–4.2 min).
Discussion
Accurately ascertaining the extent of dilator progression needed for atraumatic tract dilation is crucial, as well as a challenging aspect during establishment of an access tract in PCNL.
Percutaneous access can be guided either by fluoroscopy, US, or a combination of both techniques, depending on surgeon preference, experience, and its availability. To avoid exposure to harmful ionizing radiation, the US-guided percutaneous technique is emerging among endourologists as a reasonable alternative over conventional fluoroscopy-guidance techniques. 5,7,9 –11 Its other advantages include quick procedure, possibility of real-time monitoring of needle and collecting system in the same plane, identification of the organs and structures intervening between the puncture site and kidney to avoid injury, the nonrequirement of contrast agent administration, and intraoperative use in detection of residual fragments, particularly radiolucent calculi. 5,6,10,12,13
Nephrostomy tract dilation is commonly performed with ADs, Alken type metallic telescopic dilators (MTDs), and balloon dilators. AD and MTD are commonly used methods during complete US-guided PCNL because dye/air inflation can only be monitored well under fluoroscopy.
The efficacy and safety of US-guided initial puncture has been well documented. 5,9,11,14 The echogenicity of the guidewire and the dilator during US-guided tract dilation using an Amplatz dilator and Alken metallic telescopic dilator, however, may not be good enough to accurately monitor the dilator progression into the target calix. Thus, it makes the dilation of the access tract in complete US-guided PCNL rely on surgeon experience and “feel” during the procedure. 6,7 Other common methods of assessing the dilator progression by either comparing the length of dilator inserted to the measured length of the puncture needle from skin to renal collecting system or from free flow of saline through the dilators when infused through the ureteral catheter might still compromise the accuracy and safety of the procedure.
The complications related to tract dilation are mainly perforation or tear of the collecting system, bleeding, and loss of access. Bleeding is the most common and worrisome complication during PCNL. It can occur during initial puncture, tract dilation, stone manipulation, and even during the postoperative period. Overadvanced dilation can cause tear or perforation of the infundibulum, renal pelvis, or ureteropelvic junction, either directly by the dilator or indirectly by the stone pushed aside by the dilator. Parenchymal laceration or injury to interlobular arteries so caused can lead to bleeding. It might even cause extravasation, infundibular stenosis, ureteral stricture, or avulsion. Overadvancement of the sheath into the renal parenchyma as well can be potentially traumatic causing intraoperative bleeding. 2,5,15 –17 In contrast, underadvancement of the dilator results in “short” dilation necessitating redilation or maneuvering of the access sheath into the target calix under direct nephroscopy. Also, the sheath when advanced over an incompletely dilated calix can tear the renal parenchyma trapped between the dilator and the sheath.
In addition, far too medially directed dilation could cause injury to hilar vessels (segmental arterial branch) and develop arteriovenous fistula or pseudoaneurysm necessitating selective angioembolization or even nephrectomy.
Thus, even after successful initial puncture, tract dilation when not performed accurately can potentially be traumatic leading to complications such as perforation, bleeding, and loss of access. Because these complications can, as well, occur during puncture, stone manipulation, or even postoperatively (blood loss), it is difficult to predict their individual relation to tract dilation separately and is seldom mentioned in the literature. 18 Perforation has been associated with two-fold increase in intraoperative bleeding, however. 14 In the literature, different pelvic perforation rates as high as 16.6% using an Amplatz dilator and 11.2% using a balloon dilator have been reported. 2,7,13,17 –20 Renal pelvis perforation during dilation or sheath placement may also cause small bowel or colon injury. 2,17,21
Anteromedial excursion of the kidney during dilation further increases difficulty in correct assessment of dilator progression, making nephrostomy tract creation particularly challenging. This situation can therefore increase the possibility of perforation and loss of access. Researchers have appreciated a higher incidence of kidney hypermobility and related difficulty during tract dilation in supine or semisupine PCNL. 22 –27
This study represents the “proof of concept” of using a novel technique of performing percutaneous access tract dilation under direct vision through the dilator. The technique was successfully administered during tract dilation and positioning of the access sheath in both in-vivo and ex-vivo animal models without any perforation, excessive bleeding (in the in-vivo model), or loss of tract. We believe our good results in this experimental study depend on a number of reasons:
First, the initial puncture was performed through the infundibulum of the target calix under US guidance, which provided real-time monitoring of needle progression and the collecting system in the same plane to prevent injury to major vessels or renal parenchyma.
Second, the visual dilator system provided direct visual monitoring of the entire process of dilator progression from the puncture site, through tissue layers outside the renal capsule, renal parenchyma, and finally into the pelvicaliceal system. This real-time visual control associated with retained tactile sensation of dilator progression over the guidewire promoted effective dilation avoiding both overadvancement (thereby potentially reducing the risk of pelvicaliceal perforation or vascular lesion) and underdilation (thereby potentially improving the efficacy).
Third, the dilation through the renal parenchyma was performed in one step to minimize tract bleeding. Past studies have shown that one-step dilation is safe, efficient, and, in addition, overcomes the possibility of increased bleeding from loss of the temponading effect during exchange of sequential dilators. 22,27,28
Fourth, the access sheath was advanced under visual guidance into the target calix only after confirming that the dilator tip was completely inside the infundibulum, thereby avoiding parenchymal tear trapped between the sheath and dilator.
Finally, all procedures were performed by a single surgeon experienced in US-guided PCNL.
The most challenging aspect of PCNL for urologists during their learning curve is the initial puncture and controlled tract dilation needed to gain optimal access to the collecting system. Inadvertent and inaccurate dilator progression can cause traumatic dilation jeopardizing the safety and efficacy of the procedure. As such, we believe that US-guided optimal initial puncture associated with direct visual control on dilator progression into the calix as well as the placement of an access sheath using the visual dilator system could prove helpful to overcome tract dilation-related difficulty and hence to gain competence in performing complete US-guided PCNL.
This study demonstrates our preliminary experience with the technique and has a number of limitations. First, the study was performed only in a limited number of animal models. Second, it lacks comparison of this technique with other available dilation modalities. A randomized study of this technique in a larger sample of clinical cases with comparison with other contemporary methods is warranted to clearly evaluate its actual strengths, weaknesses, and relative efficacy. Third, the procedure was conducted by only one endourologist. In spite of the device being simple and easy to use, a generalized endourologic experience is needed. Finally, the visual dilator system in this study was used to create US-guided percutaneous access. The dilator being radiolucent, its tip cannot be visualized clearly under fluoroscopy. In our opinion, a radiopaque marker incorporated at the tip of the dilator will allow its better fluoroscopic visualization and hence can be used during fluoroscopy-guided access tract creation to visually confirm the approach of the dilator tip into the collecting system to further improve the safety and efficacy of the procedure. This needs to be confirmed in future trials, however.
Conclusion
The novel “visual dilator system” tested in animal models proved to be feasible, safe, and effective. It could be considered as an option to perform visually guided percutaneous access tract dilation and further improve the safety and efficacy in accomplishing the most crucial step in PCNL.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.