
Abstract
Introduction:
Functional outcome and quality of life (QOL) domains are important outcomes after curative therapy for prostate cancer. Although useful for scientific purposes, QOL questionnaires may be too extensive for daily routine, and single questions or interview-assessed outcomes may be more practical alternatives. The QOL outcomes of these measures were compared.
Materials and Methods:
The QOL of patients undergoing Robot-Assisted Radical Prostatectomy (RARP) in our hospital was monitored before and after treatment using both brief standardized interview questions, as well as more extensive validated questionnaires. The interview questions address erectile function and urinary continence with only one question on each subject (both four response items). Questionnaires included a total of 74 questions (EORTC-QLQ-C30, EORTC-QLQ-PR25, international index of erectile function-15, and international consulation on incontinence questionnaire-short form).
Results:
In 925 RARP patients, pre- and postoperative interview and questionnaire QOL data were available with a median follow up of 20 months. Improvement in both erectile function and continence scores occurred up till 2 years after the RARP for both interview- and questionnaire-based evaluations. On an individual patient basis, interview scores poorly correlated with questionnaire-based domains for continence and erectile function. Single questions from the questionnaire showed better correlation with domain scores. Functional recovery of continence after 1 year was worse when assessed by questionnaire than by interview evaluation. A decrease in physical (8%) and overall QOL (12%) after prostatectomy as assessed by the EORTC-QLQ-C30 questionnaire was better predicted by questionnaire-based than interview-based scores. Continence scores had a greater impact on physical and overall QOL scores than on erectile function scores.
Conclusion:
Interview/assessed continence and erectile function outcome after RARP showed limited association with questionnaire-based evaluation and may overestimate functional recovery. Continence scores for both interviews and questionnaires were stronger correlated with physical and overall QOL than erectile function scores.
Introduction
Functional outcome after prostatectomy has been the subject of extensive studies. Most studies use validated questionnaires to objectively assess and compare outcomes on physical domain items such as continence and erectile function, and on quality of life (QOL) in general. 1,2 Many of these questionnaires contain numerous questions, making them less suitable for short evaluation in daily practice. Simplification and categorization of questionnaires may improve clinical applicability. 3,4 A single question on erectile function as proposed by Tal et al. 5 showed reasonable correlation with the international index of erectile function (IIEF)-15 score. Guiding patients through the months after a prostatectomy using simple QOL analysis provides an insight into the course and mechanisms of functional recovery.
In the present analysis, we studied three aspects of QOL after Robot-Assisted Radical Prostatectomy (RARP): (1) The interview- and questionnaire-based recovery patterns of continence, erectile function, and physical and overall QOL; (2) the correlation between interview-based and questionnaire-based QOL scores; and (3) the application of single questions from the questionnaires as surrogates.
Materials and Methods
In a consecutive group of men who underwent an RARP in our specialized oncological center within the study interval (2006–2012), both interview and questionnaire QOL data were obtained. Patients prospectively completed the interviews and questionnaires at set intervals. Outpatient visits were scheduled every 3 to 4 months the first 2 years postoperatively and yearly thereafter. Questionnaires were either mailed on paper or digitally through e-mail.
Interview-based questions
Preoperatively, and during each control follow-up visit after RARP, two standardized questions regarding erectile function and continence were addressed to the patient by either the urologist or the nurse practitioner. Erectile function was assessed as 1. normal (penetration possible), 2. weakened (erection present but with shorter duration), 3. PDE5i-use (erection sufficient only with PDE5 inhibitors), and 4. no or strongly reduced erection. Second, patients were asked whether incontinence was present. Continence was scored as: 1. normal (no pads and no involuntary urine loss), 2. loss of drops of urine but no pad use, 3. maximum one pad per 24 hours, or 4. more than one pad per 24 hours.
Questionnaires
In addition to the interview-based questions during outpatient visits, preoperatively and at 6 months intervals postoperatively, patients also received an extensive set of QOL questionnaires. Patients filled out the questionnaires at home either using an online system or a paper version. The questionnaires evaluated general QOL using the EORTC-QLQ-C30 6 (30 questions with 4 response items each), the prostate specific QOL using the EORTC-QLQ-PR25 7 (25 questions with 4 response items each), the erectile function using the IIEF-15 (15 questions with 5 response items each), and continence using the international consulation on incontinence questionnaire-short form (ICIQ-SF) (4 questions with different number of response items). To assess whether a single written question or interview question had similar correlation with overall QOL, question 23 (Did you have difficulty getting or maintaining an erection?) and question 6 (Have you had any unintentional release [leakage] of urine?) from the EORTC-QLQ-PR25 were separately analyzed.
Comparison
We aimed at evaluating whether interview-based–assessment of erectile function and continence score correlated with questionnaire-based assessment. The answers on the QOL questionnaires were categorized into the commonly used domains as described in the official questionnaire manuals. For purposes of comparison, two questions, one addressing erectile function (EORTC-QLQ-PR25 question 23; ‘Did you have difficulty getting or maintaining an erection?’) and the other addressing urinary continence (EORTC-QLQ-PR25 question 6: ‘Have you had any unintentional release (leakage) of urine?) were separately analyzed. The correlation of these questions with the complete questionnaire scores as well as with physical and overall QOL (EORTC-QLQ-C30 domain 1 and 15) were also assessed.
Statistical analysis
Intervals were divided into year quarters. A per-quarter comparison of QOL interview- and questionnaire-based scores was done using nonparametric tests (Kruskal–Wallis test). For correlations of scores, the Spearman rho nonparametric correlations were calculated. For statistical significance, a p<0.05 was taken. SPSS version 19 was used for data analysis.
Results
For analysis, 925 men with at least two questionnaires were included. The mean number of questionnaires per patient was 3.7 (SD 2.5). The mean number of interview assessments was 6.3 (SD 4.1). Median follow up after prostatectomy was 20 months. General patient characteristics as well as preoperative interview- and questionnaire-based QoL scores are presented in (Table 1).
Patient Characteristics
IIEF-EF, international index of erectile function-erectile function; ICIQ-SF, international consulation on incontinence questionnaire-short form; PSA, prostate specific antigen.
Erectile function
When IIEF-erectile function (IIEF-EF) scores and interview scores are plotted over time, both show an initial sharp decline after prostatectomy with a recovery during the first 2 years after surgery, but none of the mean scores returned to baseline (Fig. 1).
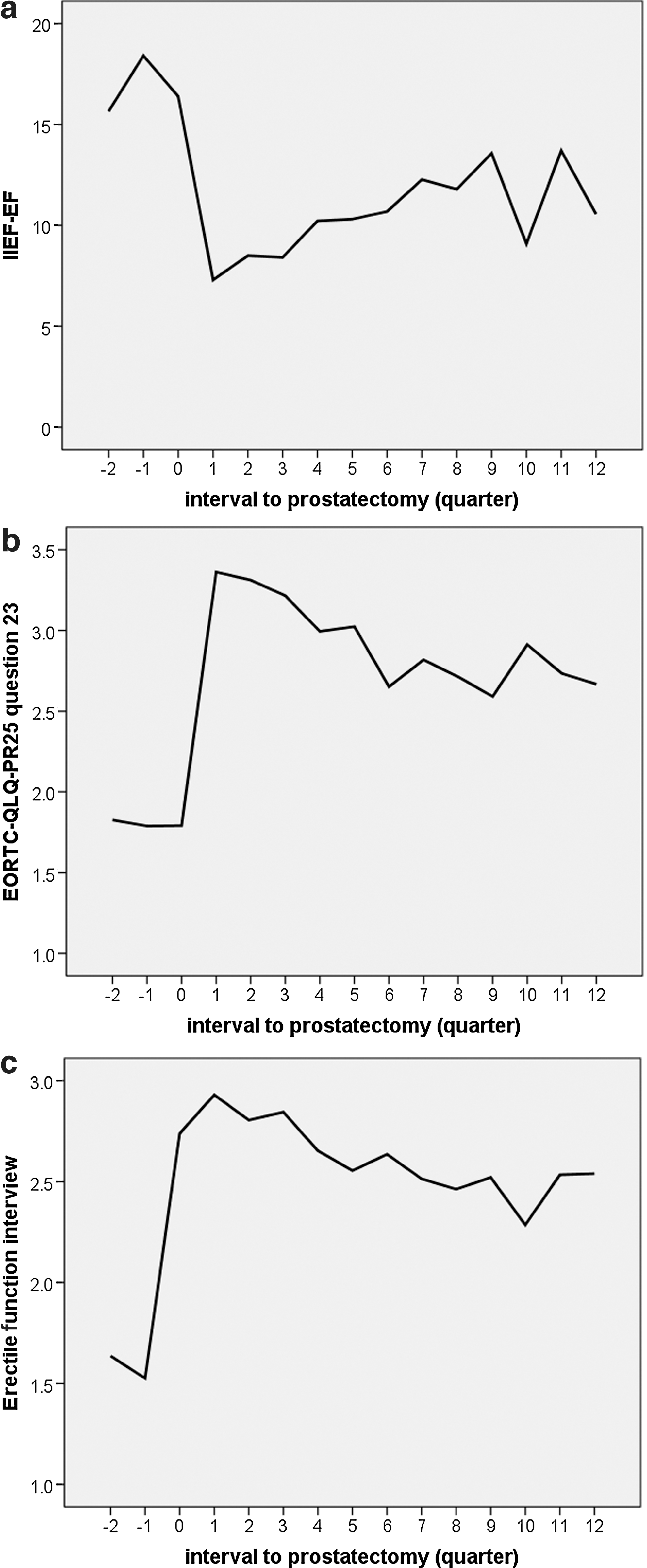
Pre- and postoperative erectile function
Continence
Continence ICIQ-SF scores, EORTC-QLQ-Pr25 question 6 scores, and interview-assessed continence scores declined sharply after prostatectomy but improved up till 2 years postoperatively.
Correlation between interview and questionnaire scores: erectile function
The IIEF-EF scores correlated with interview results but in both pre- and postprostatectomy evaluation, IIEF-EF score showed a higher correlation with the written single question (EORTC-QLQ-Pr25 question 23) than with the single interview question score (Table 2a).
Spearman Rho Correlations Between Interview and Questionnaire-Based Erectile Function Scores
Correlations between erectile function IIEF-EF domain scores and PR25 single question 23 assessments were always stronger than between domain scores and interview scores for both pre- and post-prostatectomy analyses. IIEF-EF scores showed at least a five time higher correlation with overall QOL than interview question results. (Correlations marked with an asterix showed a p<0.01 at two-sided testing.)
QOL, quality of life.
Correlation between interview and questionnaire scores: urinary continence
The ICIQ-SF scores did not show a correlation with the interview score in the preoperative setting but showed a significant correlation with the interview question after the RARP (Table 2b). When compared with the written single question on continence (EORTC-QLQ-Pr25 question 6), however, the correlation was always lower for the interview score. When median scores were compared at the 1 year postoperative interval, a higher percentage of men according to the interview question (95%) than according to the questionnaire scores (ICIQ-SF: 89%, Pr25 question 6: 90%) returned to baseline score (p=0.024, Kruskal Wallis, Fig. 2).
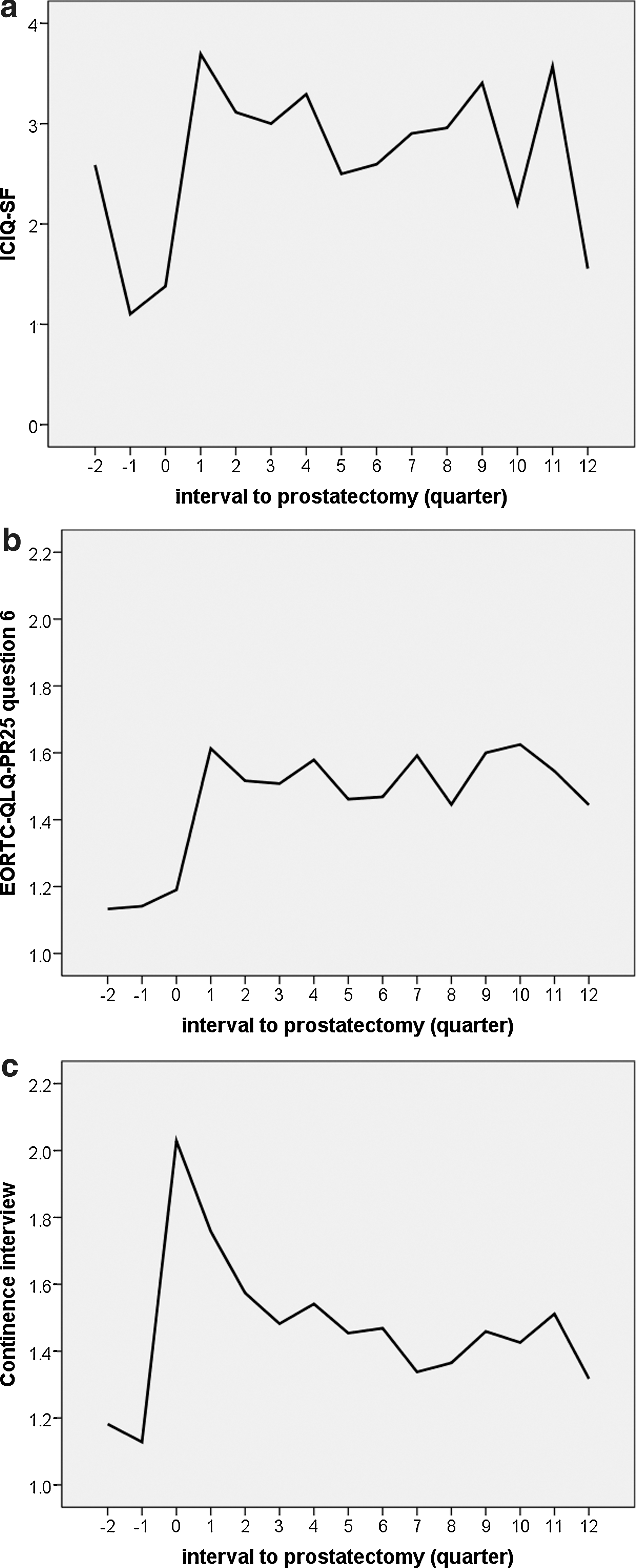
Pre- and postoperative urinary continence
Spearman Rho Correlations Between Interview and Questionnaire-Based Continence Scores
Correlations between ICIQ-SF domain scores and PR25 single question 6 assessments were always stronger than between domain scores and interview scores for both pre- and post-prostatectomy analyses. ICIQ-SF score showed a stronger correlation with overall QOL than interview question score. (Correlations marked with an asterix showed a p<0.01 at two-sided testing.)
Quality of life
Although postoperative median EORTC-QLQ-C30 domain 1 (physical QOL) and domain 15 (overall QOL) scores did not change significantly from preoperative scores, 74 (8%) and 110 (12%) of men reported a decreased QOL 1 year after prostatectomy, respectively (Fig. 3).
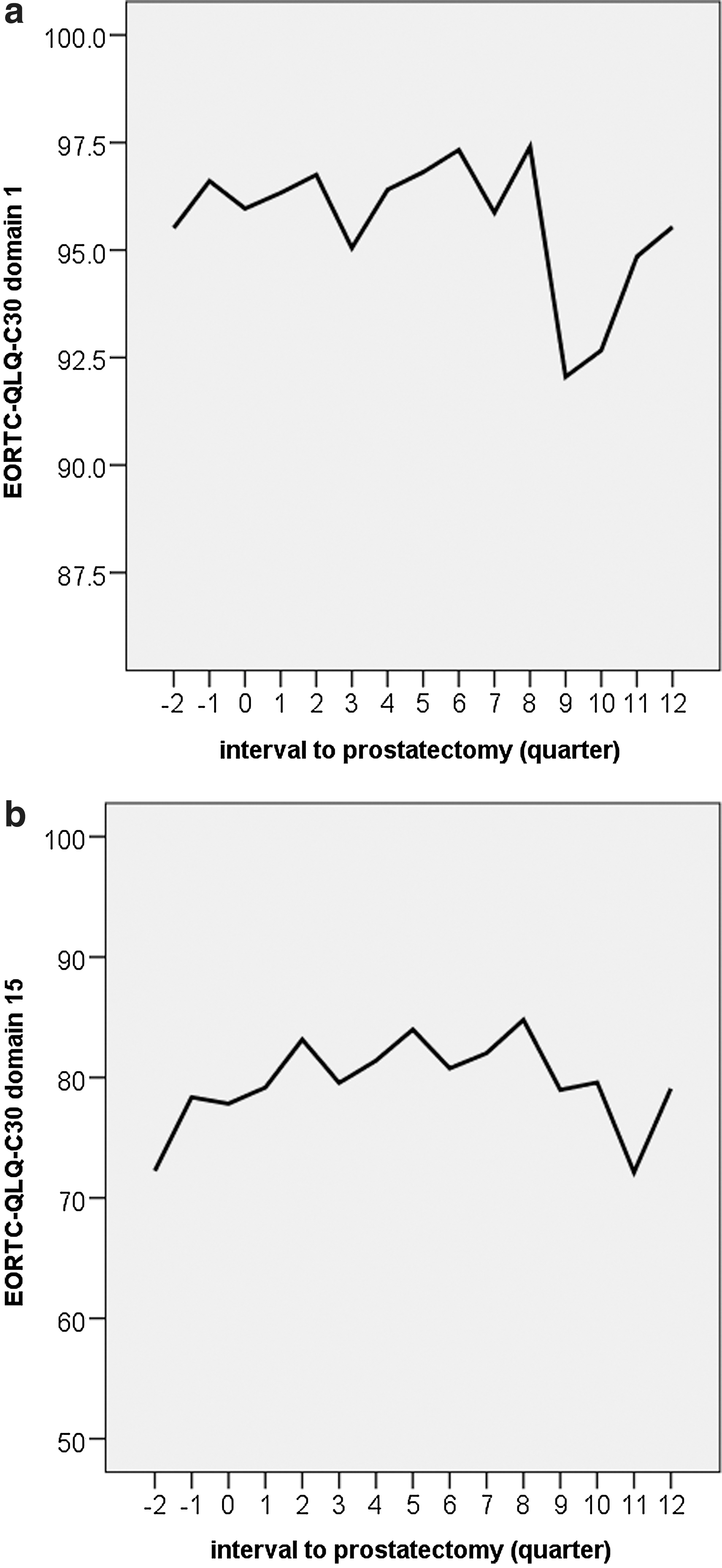
To assess the effects of erectile dysfunction and continence on more general QOL measures, the scores for erectile function and continence scores were compared with the pre- and postoperative EORTC-QLQ-C30 domain 1 (physical QOL) and domain 15 (overall QOL).
IIEF-EF scores showed a weak but statistically significant correlation with physical QOL and overall QOL in both the pre- and postoperative evaluation (Table 2a). Men with better scores for IIEF-EF had higher scores for both physical and overall QOL. Erectile function as assessed by interview score was not significantly correlated with physical and overall QOL neither in the pre- nor in the postoperative evaluation (Table 2a).
The ICIQ-SF incontinence score correlated with physical QOL score and overall QOL in both the pre- and postoperative analysis. Overall QOL (EORTC-QLQ-C30 domain 15) was not correlated with interview continence scores. Comparing the answers on EORTC-QLQ-PR25 question number 6: ‘do you experience involuntary urine loss' with physical QOL showed a gradual statistically significant decrease of QOL score with an increase in urine loss bother with a Spearman rho correlation similar to the correlation of the ICIQ-SF score (Table 2b). This suggests that a single written question may be a substitute for the three questions domain in the ICIQ-SF questionnaire.
Discussion
First, this analysis of questionnaire- and interview-assessed erectile and continence function after RARP showed comparable trends with an initial decrease and subsequent gradual improvement in function. Recovery of both continence and erectile function was observed up till 2 years after RARP. Continence scores for both interviews and questionnaires were stronger correlated with physical and overall QOL than erectile function scores. Second, interview-assessed continence and erectile function were poorly correlated with questionnaire-based assessment. Third, a single questionnaire item may provide a surrogate for compound questionnaire domains, but interview-based assessment for incontinence at 1 year may underestimate incontinence when compared with questionnaire-based assessment.
Functional outcome after prostatectomy is the subject of many studies. Often, questionnaires are used to assess and compare outcomes. For daily practice, questionnaires are less useful to compare alterations in outcome over time at frequent follow-up visits. Our analysis showed that similar to earlier studies, erectile function and continence deteriorate mainly in the first 1 year after prostatectomy and subsequently show improvement, but for the entire population, they never return to baseline, 1,2 Interestingly, interview scores for erectile function correlated with questionnaire scores differently in the preoperative and postoperative setting. Preoperative interview scores of poorer erectile function were associated with higher IIEF-EF scores than in the postoperative setting, suggesting that the interview scores in the postoperative setting may overestimate the actual erectile function. Patients in the postoperative setting reported better functional outcome using interview assessment when compared with questionnaires, and we, therefore, consider questionnaires a better tool for assessing erectile function, in particular in the postoperative period.
To study whether the fact that only a single question addressed continence and erectile function in the interview assessment accounted for this poor correlation with domain scores, we also studied results from a single questionnaire item on these topics from the EORTC-QLQ-Pr25 (question 6 and 23 for urinary continence and erectile function, respectively). A single question on erectile function (EORTC-QLQ-PR25 question 23: ‘did you experience problems maintaining an erection?’) from the questionnaire showed a better correlation with IIEF-EF domain score than the single interview question, suggesting that indeed the written form of evaluation rather than the single question accounted for the better correlation with the domain scores. 5
The underreporting of function loss in the postoperative period using interview scores was also observed in the continence assessment. Similar interview continence scores showed higher ICIQ-SF incontinence scores in the postoperative period compared with the preoperative period. Again, this observation suggests that patients in the postoperative period underreport incontinence by interview assessment. Although general QOL assessment showed reasonable agreement with interview scores 8 others found underreporting of functional 9 and satisfaction 10 outcome when using interview versus questionnaire methods. Functional outcome is particularly subject to interpretation, and patients may underreport dysfunction when assessed by interview. Our findings, therefore, stress the importance of self-administered questionnaires to assess postoperative functional outcome, whereas baseline functions can be more reliably assessed using interview methods.
Earlier studies showed that sexual function is not always correlated to sexual and overall satisfaction. 11 Therefore, we studied the effects of erectile function alterations on the physical and overall QOL scores of the EORTC-QLQ-C30 questionnaire (domain 1 and domain 15, respectively). Although a weak correlation between physical and overall QOL scores and questionnaire- and interview-based erectile function was observed, most men maintained baseline QOL scores after prostatectomy despite a reduction in erectile function in the majority of men.
Continence scores showed a stronger correlation with physical and overall QOL scores than erectile function scores. Postoperative physical and overall QOL were negatively affected by postoperative incontinence. These findings are in line with the observations 12 that showed continence function to be predictive of regret after RARP, whereas sexual function was not predictive. Maintenance of urinary continence function should be an important aspect in prostatectomy treatment. 13,14
Conclusion
Interviews as well as questionnaires showed that both erectile function and continence scores deteriorate after prostatectomy with some improvement during the first 2 years. Interview scores seem to underestimate the effects of prostatectomy on continence and erectile function. Physical and overall QOL scores after prostatectomy decreased in ∼1 out of 10 men and were more dependent on continence outcome than erectile function outcome. Although single interview questions outcomes were not accurately correlated with questionnaire domain scores, single written questions from the applied questionnaires may substitute for more extensive domain scores, although validation for the questionnaire simplification is needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.