
Abstract
Micropercutaneous nephrolithotomy (microperc) is the end point percutaneous nephrolithotomy (PCNL) technology for the present. In routine PCNL surgery, use of an Amplatz sheath is an important step, but in this technique, there is no Amplatz sheath. Some problems during surgery may occur because of the lack of an Amplatz sheath, which provides a tract between the skin and the collecting system. Therefore, we describe the smallest Amplatz sheath (6.6F) that is compatible with the microperc instrument and can be used during percutaneous surgery, especially in preschool pediatric patients.
Introduction
After enough evidence in the literature suggested that decreasing the tract size for standard PCNL could decrease bleeding and morbidity, 4 Bader and associates 1 developed the all-seeing needle, which permits visualization of the entire tract during percutaneous access, and Desai and colleagues 3 extended this concept to performing renal access and PCNL in a single step by using the all-seeing needle with a 4.85F tract size. They defined this technique as “micropercutaneous nephrolithotomy” (microperc). 3 Recently, Tepeler and coworkers 5 presented the feasibility of microperc in the management of symptomatic lower pole renal calculi, and Armagan and colleagues 6 presented the feasibility of microperc in the management of moderate-sized (1–3 cm) kidney stones.
In all kinds of PCNL procedures, first, a ureteral catheter is inserted into the ureter with the patient in the lithotomy position, and then access to the collecting system is performed, mostly with the patient in a prone position. After the placement of a guidewire to the renal collecting system, the tract is dilated, according to the operation's technique (standard PCNL or miniPCNL). At the end of the dilation, an Amplatz sheath is placed into the tract, and the operation is continued by using the Amplatz sheath. At the end of the operation, a catheter is usually inserted through the Amplatz sheath. The microperc technique has two fundamental differences from the standard PCNL techniques mentioned above. First, dilation is not needed, and second, the Amplatz sheath is not needed.
This is especially true in pediatric cases. Despite the short distance from the skin to the collecting system, a 200-mm length microperc puncture needle and needle working sheath are used. In pediatric cases, long needles have some disadvantages; therefore, shorter needles are preferred because of easier orientation and manipulation. 7 In addition, because of the absence of the Amplatz sheath, some of the surgical manipulations (such as taking the inner shaft, placement of the connector and laser fiber, cleaning of the optic and view, balancing the intrarenal pressure by draining the collecting system quickly, etc.) of the device are difficult. To overcome the above-mentioned disadvantages, we thought that an Amplatz sheath (14-gauge intravenous cannula or angiocath sheath) that does not affect the advantages of the microperc technique might be a useful device for us.
Technique
Patient preparation
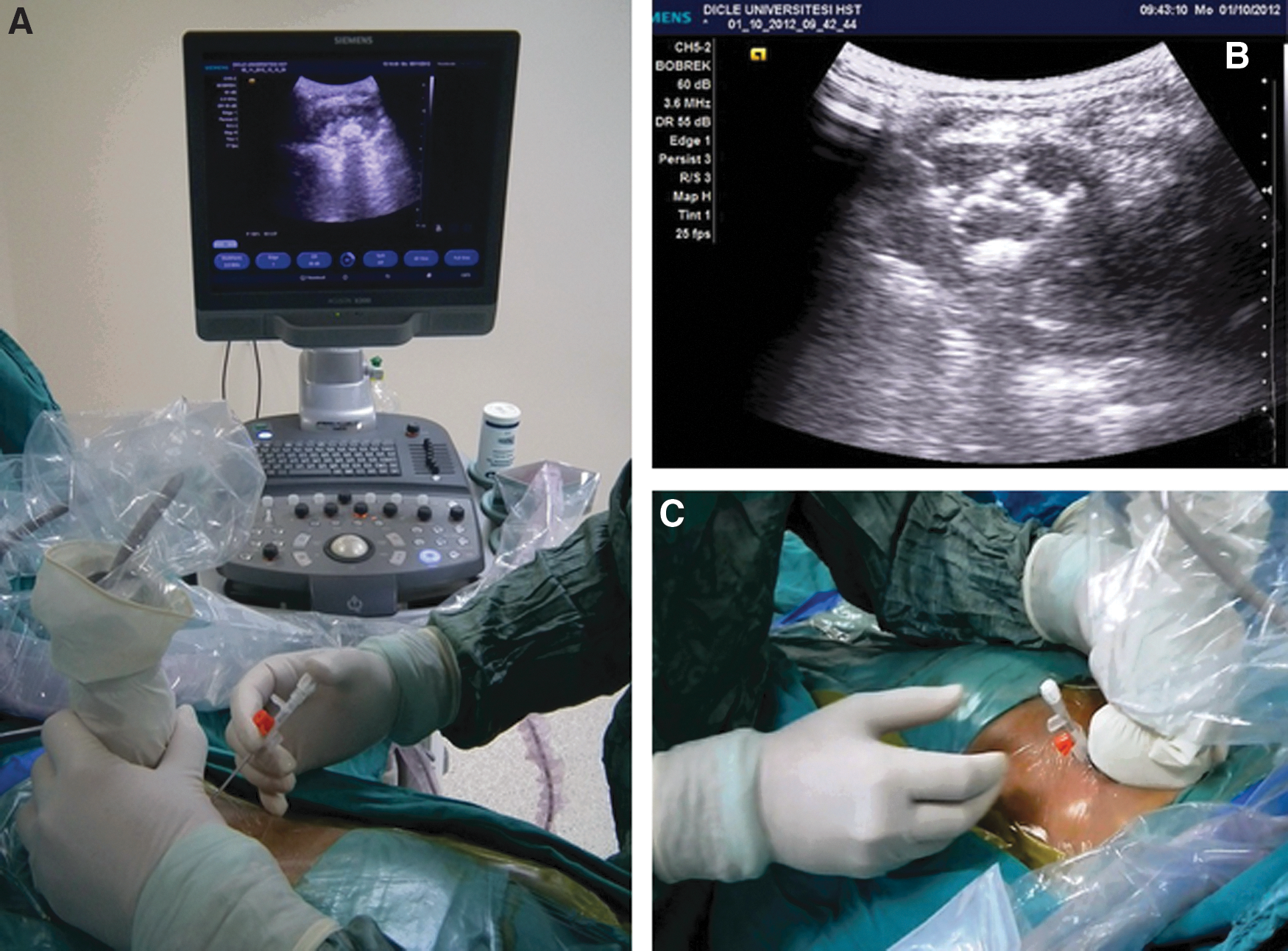
After the insertion of a ureteral catheter with the patient in the lithotomy position, the patient is placed in a prone position, and the targeted calix of the kidney is determined under ultrasonographic (US) guidance (Fig. 1). During this maneuver, the longest axis of the kidney is considered, and an attempt is made to visualize the posterior border (Brodel line). At this point, the distance between the skin and the targeted calix should be less than 45 mm, and this condition is usually true in preschool children.
The microperc system should be extracorporeally ready to use. The all-seeing needle consists of three parts. In this technique we do not use the first two parts of the needle (the puncture needle and the inner needle); we only use the working sheath of the needle. A three-way connector that allows the insertion of the optic, the laser fiber, and the irrigation system is attached to the proximal end of the working sheath. The micro-optic with integrated light lead, 270-μm laser fiber, and irrigation system are connected to the connector. The system is now ready for use.
Percutaneous access
Percutaneous access is achieved as we described previously. 7 After the targeted calix of the kidney is determined under ultrasonography (US) guidance, the US probe (without a puncture attachment) is immobilized at this position with the left hand. Using the right hand, percutaneous access is made with a 14-gauge angiocath inserted from the contact point between the probe and the skin (Fig. 1). The US shows the movement of the needle from the skin through the access tract. The angiocath with a needle is pushed through the appropriate calix under US guidance. After the entry of the needle tip into the appropriate calix is visualized, the plug at the external end of the angiocath is opened to observe urine flow. Afterward, while removing the metal needle from inside the angiocath, the sheath over the needle is pushed forward a few millimeters. If urine flow from the sheath persists, the sheath is ready for use (Fig. 2).
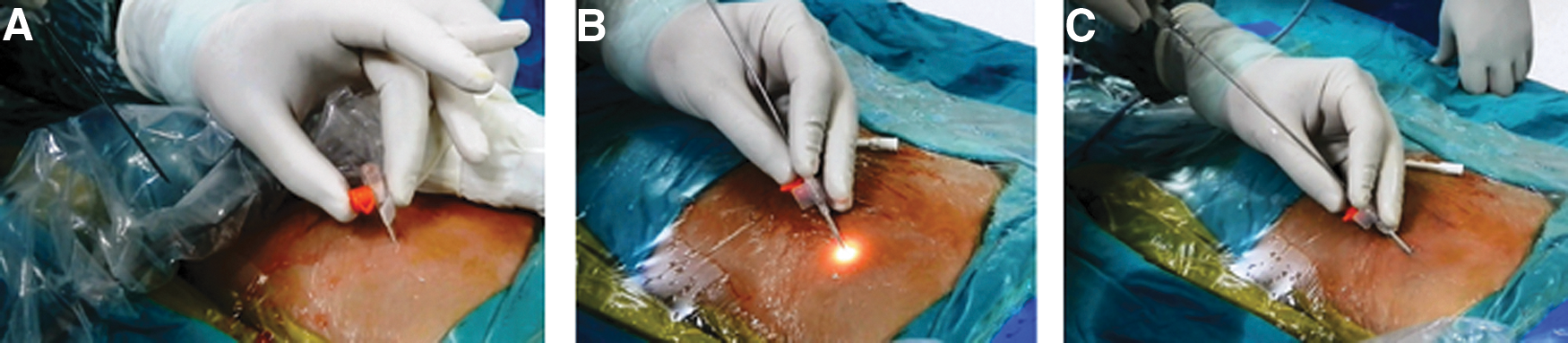
The next stage of the intervention is to continue the operation through the sheath like a standard microperc. The inner diameter of the microsheath is 1.74 mm, and the outer diameter of the microperc working sheath is 1.6 mm; therefore, there will not be any difficulty during the process. Thus, between the skin and the collecting system a safety tract has been ensured, which can let us easily and safely go in and out to the kidney.
Equipment
We have found that this technique is best achieved with the following instruments (Fig. 3). Also, some detailed information can be seen in Table 1.

• 14 gauge angiocath (B-Cat2 I.V. Cannula, Istanbul, Turkey)
• All-seeing needle 16 gauge (PolyDiagnost, Pfaffenhofen, Germany)
• Puncture stylet (will not be necessary)
• Working sheath
• Micro-optic (0.9 mm, 10,000 pixels)
• 3-way connector
• Laser fiber (270 μm)
• Irrigation system
• Ultrasound probe or C-arm fluoroscope
Role in Urologic Practice
To our knowledge, this sheath is the smallest sheath that can be feasibly used in PCNL. We will mention some of the advantages of the microsheath and this technique. Performing access with an angiocath under US guidance provides direct access to the kidney in the shortest possible distance through the cup of the calix. In addition, during access, there is no need to use fluoroscopy, which is a significant advantage, especially in pediatric cases.
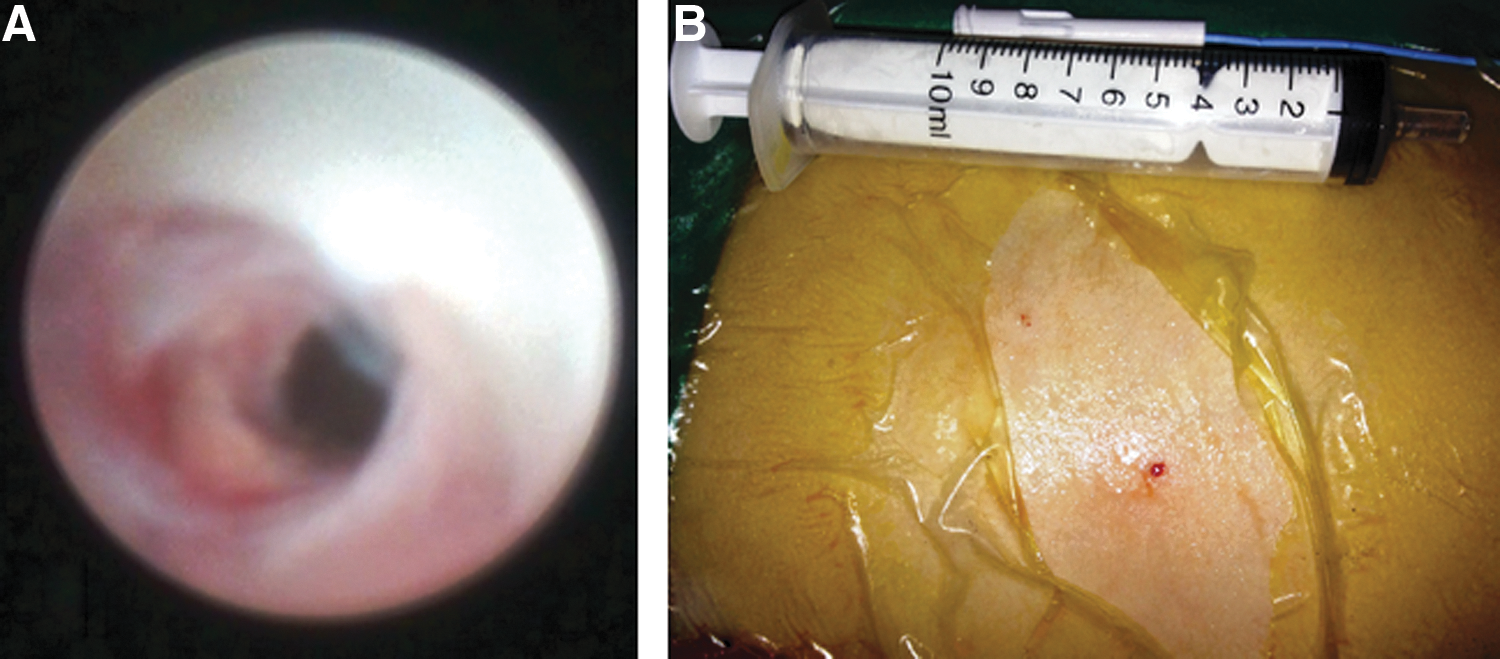
Use of a 45-mm long needle to perform percutaneous access instead of the 200-mm long needle is an easy, safe, cheap, and practical access method that is readily available. 7 The microsheath is made from fluorinated ethylene propylene, a soft and malleable material that does not damage the tissue during operation. Microperc system-related technical problems (eg, impairment of vision) may arise; this can be easily solved by taking out the microperc working sheath. In this method, telescopes are needed during stone fragmentation but not for access. Therefore, the life expectancy of the microperc instrument (especially the optical system) can be prolonged by using an angiocath to pass the resistant tissues, such as fascia, during access. The subcutaneous tissue, muscle layer, fatty tissue, renal parenchyma, and entrance of the collecting system can be visualized via the transparent structure of the sheath (Figs. 4 and 5). Like these visualized layers, adjacent organ injuries also can be seen via the transparent structure of this sheath. We never experienced an injury neither clinically nor during operation, however, so it is difficult to make a decision about injuries to other organs that can be prevented by this sheath because of lacking lacking in this study.

There is no study in the literature about elevation of pressure during microperc surgery; however, Desai and associates 3 and Desai and Mishra 8 warned about the elevation of intrarenal pressure during microperc operations, and they were working on reducing it. The same problem was experienced in retrograde intrarenal surgery, and Auge and coworkers 9 solved the problem by using the ureteral access sheath. Here we have a similar solution by using a microsheath.
Contrary to the standard microperc technique, during this procedure, in the presence of the elevation of intrarenal pressure, the microperc working sheath can be pulled back and fluid in the pelvicaliceal system can be discharged easily. Already the inner diameter of the microsheath is wider than the outer diameter of the microperc working sheath, and this situation may contribute to reducing the intrarenal pressure because of leakage from the edge of the working sheath. Furthermore, intraoperative bleeding (leading to impairment of vision) may occur because of needle insertion or movement of the working sheath, and a sheath may diminish parenchymal bleeding.
This technique has some limitations. First, the sheath is ineffective for use in older children and adults because of the increased distance from the skin to the calix. This problem can be solved with the production of longer angiocath or sheaths. Second, the all-seeing needle feature of this instrument is not used. It did not create any problem for this technique during access, however.
Conclusion
Microperc is the smallest size PCNL technique, and a microsheath is the smallest size sheath used for PCNL. The use of microsheaths in microperc operations appears feasible, safe, and efficacious, especially in preschool patients.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.