
Abstract
Purpose:
To present an improvised method for repositioning a proximally displaced stent using only a cystoscope and a guidewire.
Methods:
A Glidewire guidewire (Boston Scientific) was passed through a cystoscope and into the distal ureter, and manipulated up the ureteral stent into the renal pelvis, reflected, and passed antegrade down the ureter and into the bladder. The guidewire was then grasped in the bladder, clamped at the penis, and retracted, pulling the stent back into the bladder.
Results:
The patient proceeded with lithotripsy, and the stent was removed in 2 weeks without complication.
Conclusion:
Methods at retrieving proximally displaced ureteral stents after deployment have been previously reported; however, these methods necessitated access to a ureteroscope and special graspers/baskets that may not be available in an outpatient surgical center setting. Here, an improvised method for stent repositioning using only a cystoscope and a guidewire allowed successful retrieval of a proximally migrated stent.
Introduction
During placement of a ureteral stent, the stent migrated proximally into the distal ureter.
Methods
The migrated stent (6.0F, Optima,® Bard) was identified on rigid cystoscopy and confirmed with fluoroscopy to have a distal ureteral location. The distal end of the stent remained parallel with the ureteral course without the pigtail curled. Flexible and semirigid ureteroscopes, as well as upper tract instrumentation devices, were unavailable in the outpatient surgery center. Subsequently, a 0.038 inch, angled, hydrophilic, Glidewire® guidewire encased by a 5F open-ended catheter (Boston Scientific) was passed through the cystoscope into the bladder. Through the open-ended catheter, the guidewire was manipulated into the stent's lumen under fluoroscopy. With the stent's lumen in parallel within a nondilated distal ureter, access was gained with minimal manipulation of the angle tip under fluoroscopy.
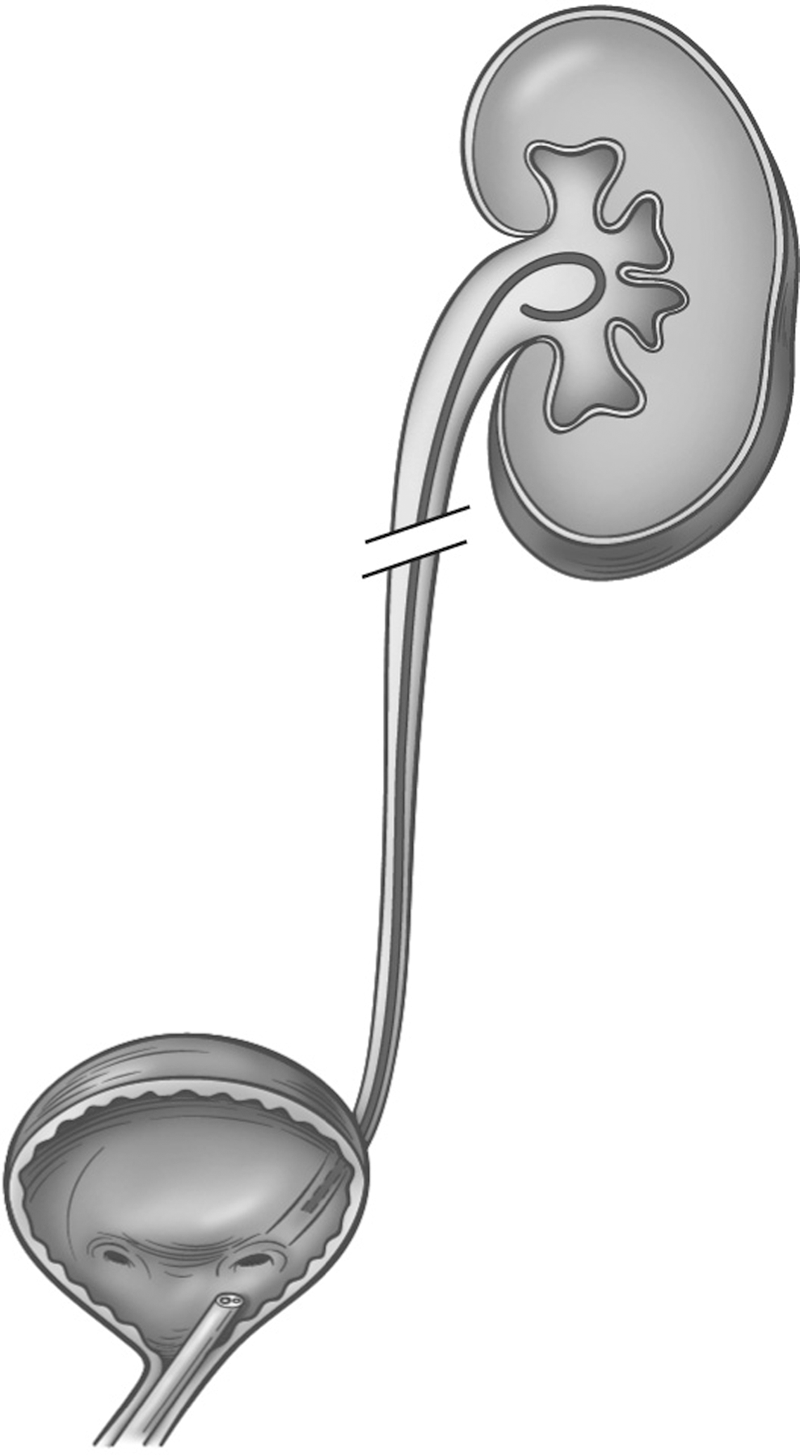
The wire was advanced into the renal pelvis and, under fluoroscopy, reflected and advanced in an antegrade fashion back into the bladder. The wire was then positioned to allow both wires to remain in the bladder with cystoscope removal. One end was clamped outside the meatus and, after reinserting the cystoscope, the remaining wire was grasped in the bladder and retracted until the stent was in adequate position for guidewire removal. This resulted in appropriate stent placement seen on cystoscopy and fluoroscopy with a curl in the renal pelvis and bladder (Fig. 2).

Ureteral stent inadvertently retracted into the distal ureter during placement;
Results
Access and reflection back into the bladder were obtained in approximately 15 minutes with less than 2 minutes of intermittent fluoroscopy. In total, the cystoscopy portion of the case occupied approximately 30 minutes. Repositioning the stent allowed the patient to proceed with lithotripsy, and the stent was removed in 2 weeks in the office without complication. Renal ultrasonography at 6 weeks demonstrated normal upper tracts and stone free status.
Discussion
There are multiple factors that may lead to positioning of the distal stent within the ureter. First, during placement, the distal end can be advanced into the ureter either under direct vision or while advancing under fluoroscopy. In our case, an unexpected movement in a lightly sedated patient resulted in the distal ureteral stent within the ureter. Once placed, risk factors for migration are inadequate stent length, distal curls within the bladder of less than 180 degrees, and a proximal curl positioned in the upper calix vs the renal pelvis. 1 Furthermore, stent coil strength weakens over time, and this may lead to proximal migration. 2
Proximal stent migration retrieval in the distal ureter has been previously described using various techniques, with ureteroscopic retrieval being the most effective. 3 Katske and Celis 4 described retrieval with a 3F Fogarty catheter with a 0.2 cc balloon. 4 Ureteral balloon dilators, stone baskets, and grasping forceps have also been used to manipulate stents from the distal ureter into the bladder. 5,6 These techniques rely on the availability of ureteroscopes and specific endoscopic instruments that may be absent from surgery centers, offices, or lithotripsy suites. We offer an alternative, improvised, method to retrieving a proximally migrated stent that needs only a guidewire. The technique is inexpensive, requires minimal time, and may offer a chance at stent retrieval, thus avoiding transferring a patient to a facility with a ureteroscope, special ureteral instruments, and necessitating additional anesthetic.
The last decade has demonstrated increased use of outpatient treatment centers for ureterolithiasis. 7 In these remote settings, surgeons may not have access to the normal armamentarium of instruments and devices and thus must be prepared to adapt to changing conditions and situations. In the event that a ureteroscope is available, the technique described in this report could be modified with the wire being placed via the ureteroscope if traditional methods fail.
The main limitation of this technique is the ability to cannulate the stent with the guidewire, which may be challenging and influenced by many factors. First, the distal portion of the stent needs to be parallel to the ureter for this technique. Remaining in parallel is most dependent on the degree of dilation of the distal ureter and the coil strength of the stent, a property of high variability among different medical device companies and even among the different types of stents made by a company. 2
In our case of a proximal stone and no previous stent, we suspect the distal ureter was not dilated before insertion, and this may have helped prevent distal stent curling. Furthermore, the inherent, relatively modest coil properties of the Bard Optima stent 2 (less coil strength than many Cook stents, but similar coil strength to Microinvasive stents) may have contributed to the success of our technique. Our stent was a 6.0F stent, but a smaller 4.8F stent may be more difficult to assess with the wire. Moreover, with a proximally obstructed stone, once the stent is cannulated, it may be quite difficult to get the guidewire to return in the antegrade fashion because it may curl in the renal pelvis or become obstructed by an impacted stone.
We believe the Glidewire® guidewire (Boston Scientific) may have contributed to our success; with an angle tip and resilience to bending/kinking, this wire can be highly manipulated under fluoroscopy. This technique may be more applicable to the migrated stent during placement where the lumen is still patent. It should be acknowledged that if the string is not removed before stent insertion, then the intact string allows for the easiest retrieval of a migrated stent; however, stents may migrate after string and wire removal.
Finally, this technique used skills commonly used in urology and well within most urologists' armamentarium. Cannulating the stent was similar to accessing a difficult ureteral orifice that necessitated manipulating an angle wire tip. Reflecting the wire back down the ureter needed skills similar to repositioning the wire from one calix to another during stent placement, skills used during antegrade manipulation of the wire down the ureter during percutaneous access, and mimics a wire reflecting off a ureteral stone and exiting the ureteral orifice. As is the case with many difficult endoscopic cases, good fortune can aid in completing the task in a timely manner, but a fortuitous bounce must be coupled with endoscopic principles to complete the task.
Conclusion
According to Menezes and colleagues, 8 up to 4.2% of ureteral stents may migrate proximally. There are several options described in the literature for retrieval, but these necessitate ureteroscopes and other instrumentations that may not be available and are expensive. In the event of a migrated stent with limited ureteral access options, the described technique may allow for recovery of the migrated stent using the instrumentation initially used on stent insertion. This article serves as an initial report of an improvised method, but because of the rarity of the event from any one surgeon, further experience with this technique would need to be collectively reported among multiple institutes.
Footnotes
Disclosure Statement
No competing financial interests exist.