
Abstract
Purpose:
To present the oncologic and functional outcomes of robot-assisted partial nephrectomy (RAPN) and analyze retroperitoneal and transperitoneal approaches.
Patients and Methods:
RAPN was performed on 103 patients; 44 patients underwent a retroperitoneal and 59 a transperitoneal approach. Demographic, operative, and postoperative data was collected and retrospectively analyzed on all patients.
Results:
Overall average warm ischemic time was 20.4 (0–48) minutes, total operative time was 175.3 (85–330) minutes, and estimated blood loss was 258.1 (20–3100) mL. When retroperitoneal and transperitoneal approaches were compared, there was no significant difference in warm ischemic time but a significant reduction in both estimated blood loss and total operative time in the retroperitoneal group.
Conclusion:
Our series would suggest that if performed by a surgeon familiar with a laparoscopic retroperitoneal approach to renal surgery, retroperitoneal RAPN is at least equivalent to the more common transperitoneal approach in the outcomes assessed.
Introduction
Laparoscopic partial nephrectomy (LPN), in appropriately selected patients and in the hands of an experienced laparoscopic renal surgeon, offers the same functional and oncologic outcomes as open partial nephrectomy with a reduction in blood loss and length of stay. 12,13 Despite this, LPN remains underutilized when compared with an open approach 14 because of technical challenges needing advanced laparoscopic skills. Robot-assisted partial nephrectomy (RAPN) is emerging as a viable, minimal access alternative to LPN, capitalizing on the benefits of the laparoscopic approach while significantly reducing the learning curve for the time critical step of warm ischemia (>200 vs 26 cases). 15
Retroperitoneal LPN is a rarely used technique because of difficulties associated with using laparoscopic instruments in a confined environment such as the retroperitoneum. The transperitoneal approach to RAPN has therefore become the norm, because minimal access surgeons are more familiar with this approach to the kidney. The da Vinci (Intuitive Surgical, Sunnyvale, CA) system mitigates for the disadvantages of the normal retroperitoneal laparoscopic approach because of the Endowrists® on the robotic instruments; these make it possible to operate with relative ease in confined spaces.
In this article, we present the largest series of retroperitoneal RAPNs to date and compare the technique with the more traditional transperitoneal technique.
Patients and Methods
Patient demographics, operative, perioperative, and oncologic and functional outcome data were retrospectively analyzed on all patients and recorded in an anonymized database. All patients had preoperative R.E.N.A.L (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry scores recorded. 16 Operative parameters were recorded, such as total operative time, warm ischemia time (WIT), and estimated blood loss (EBL). Perioperative data on transfusion requirement, complications, (according to Clavien-Dindo classification), 17 and length of stay (LOS) was also collected. Positive histologic margins were used as a marker of adequacy of resection. Where available, day 1 postoperative eGFR (estimated glomerular filtration rate) and eGFR at last follow-up were calculated and used as surrogate markers of renal function and postoperative hemoglobin (Hgb) as a marker of intraoperative blood loss. eGFR was calculated using the modification of diet in renal disease eGFR formula. 18
All console surgeons are experienced laparoscopic surgeons working in teaching units. Trainees with varying degrees of robotic experience undertook tableside assistance. The dataset includes the entire learning curve of all participating surgeons.
The procedure was performed by either a retroperitoneal or transperitoneal approach—two centers performing an exclusively transperitoneal approach and one using a trans or retroperitoneal approach, depending on tumor location. Early unclamping techniques similar to those previously described in the literature surrounding LPN were used by two of the participating surgeons 13,19 –21 ; the surgeon performing a largely retroperitoneal approach used no early unclamping technique. The retroperitoneal and transperitoneal approaches both used a four-port technique. Port placement is detailed in Figures 1 and 2.

Transperitoneal port placement.
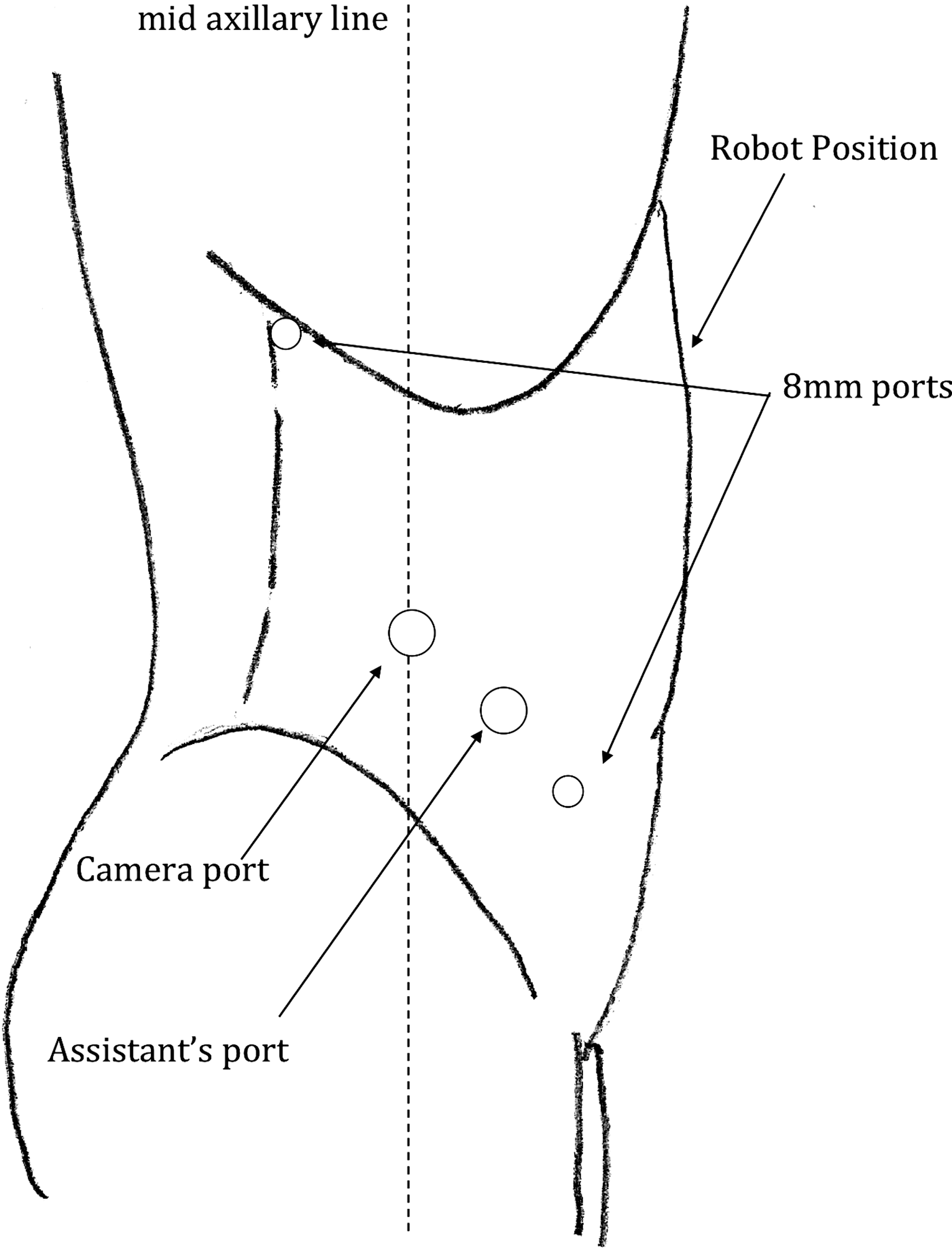
Retroperitoneal port placement.
The surgeon using both the trans and retroperitoneal approaches chose his approach largely based on tumor anatomy with all but anterior tumors approached via the retroperitoneum. Another important consideration when selecting an approach was whether the patient in question had had any previous abdominal surgery, with a retroperitoneal approach being preferred in those who had.
All statistical tests were performed using GraphPad. Unpaired t tests were used for the nephrometry scores, operative data, and LOS. Paired t tests were used for the laboratory data. The Fisher exact test was used for categorical data.
Results
Data were collected on 103 patients with a mean age of 61.7 years (Table 1). Of these, 59 underwent a transperitoneal and 44 a retroperitoneal RAPN. The tumors had an average nephrometry score of 5.5, with no significant difference in score seen between the trans and the retroperitoneal groups (P=0.83), with 74% of patients having a low score (4–6), 25% having a medium score (7–9). and 1% having a high score (10–12).
In the patient with a length of stay numbering 50 days, abdominal compartment syndrome developed postoperatively necessitating laparostomy; the healing of the laparostomy wound required a protracted admission.
WIT=warm ischemia time; EBL=estimated blood loss; LOS=length of stay.
The majority of tumors were posterior (59%), 29% were anterior, and in 12%, anterior or posterior designation was not possible. When examining the data of the surgeon performing a trans or retroperitoneal approach, 75% of the tumors were posterior in the retroperitoneal group compared with 0% in the transperitoneal group (Table 3).
Of the 103 patients in the series, 10 (9.7%) had postoperative complications. These were scored according to the Clavien-Dindo classification; there were seven grade I and II complications, one grade IIIa complication (selective embolization of the renal artery from postoperative bleeding), and two grade IIIb complications (insertion of an ureteral stent because of postoperative urinoma and retrieval of a retained swab). Of the six (5.7%) patients in the series for whom conversion to an open operation was needed, three were because of bleeding, one because of equipment failure, one because of difficult hilar identification, and one because of swab migration posterior to the liver. There was no significant difference in the number of complications between the trans and retroperitoneal groups.
The series accounts for the entire learning curve of all surgeons, and most conversions occurred toward the start of this learning curve with the majority (66%) occurring in the operating surgeon's first 12 cases.
Oncologic outcome data were recorded for all patients with a positive margin rate of 5.8% (n=6) and were distributed through the series; pathologic subtypes are detailed in Table 2. No significant difference in positive margin rates was observed between the trans and retroperitoneal groups (P=0.66). At last follow-up, there were no instances of local or metastatic recurrence in either the transperitoneal or retroperitoneal group.
AML=acute myeloid leukemia.
Average total operative time for all patients was 175.3 minutes, average WIT 20.4 minutes, and EBL was 258.1 mL.
When a comparative analysis of outcomes in the trans and retroperitoneal groups was performed (Table 1), no significant difference was seen in WIT (P=0.09), and a significant reduction in both EBL and total operative time was seen in the retroperitoneal group. Although there was a reduction in EBL, there was no significant difference in transfusion requirement between the two groups. No significant difference was seen in the last known eGFR in either the retroperitoneal group or the transperitoneal group (Table 4).
When only the transperitoneal approaches of the surgeon performing retro and transperitoneal approaches was compared with his colleagues performing only a transperitoneal approach, there was no significant difference in WIT (P=0.07), operative time (P=0.72), or EBL (P=0.10).
When the data for the surgeon who was performing the operation via the retroperitoneal and transperitoneal approaches were analyzed separately comparing the two approaches, no significant difference was seen in WIT or EBL; operative times were significantly shorter in the retroperitoneal group.
Discussion
RAPN is fast becoming an accepted modality for the resection of small renal masses with multiple cases series having been published demonstrating the safety of the procedure and its ability to achieve short-term oncologic outcomes similar to those of its conventional laparoscopic counterpart. 22 Because of its reduced learning curve, the robotic approach to partial nephrectomy potentially enables surgeons, without the requisite training to perform the conventional laparoscopic operation, access to a minimal access partial nephrectomy. 15
In this series, we have presented a comparison of 44 retroperitoneal and 59 transperitoneal RAPNs. We saw no significant difference in WIT between the two groups but a reduction in total blood loss and operative time favoring the retroperitoneal approach. Although only an indicator of significance, the retroperitoneal approach was being performed by one surgeon with a larger proportion of benign cases (22% vs 37%); the outcome data would suggest that retroperitoneal RAPN is at least equivalent (in the perioperative and immediate postoperative period) to the more common transperitoneal approach, with no significant difference seen in WIT or positive margin rates and a significant decrease in operative time and EBL.
This equivalence is further supported by the fact that when reviewing data for the surgeon performing both trans and retroperitoneal RAPNs, data for transperitoneal RAPN was compared with that of his colleagues; no significant difference was seen in any of the operative parameters. The retroperitoneal approach also afforded a minimally invasive procedure to be performed on posteriorly placed tumors; that would not have been attempted transperitoneally by the surgeons in this study.
The average nephrometry score for the series was 5.5 with no significant difference seen between the two groups. A R.E.N.A.L nephrometry score of this magnitude represents a low complexity of resection. 16 This level of resection difficulty reflects the patients who presented themselves over the course of the series but makes extrapolating our findings to complex small renal masses difficult.
When considering the retroperitoneal group specifically, we observed a significant reduction in operative time and EBL. The reduction in operative time may well have been because of a more direct approach to the kidney leading to more rapid identification of the hilar anatomy with the retroperitoneal approach.
The reduction in blood loss in the retroperitoneal group was thought to be related to the reduction in surgical dissection and may also have been a refection of occasional, but clearly important, blood loss associated with the early unclamping technique used by the surgeons performing a solely transperitoneal approach.
The improvement in ergonomics when comparing laparoscopic and robot-assisted retroperitoneal partial nephrectomy is due in large part to the articulating EndoWrists of the da Vinci system. The increased range of movement mitigates for the difficulties in instrument manipulation encountered in a conventional retroperitoneal laparoscopic approach. Although the retroperitoneal technique has previously received criticism because of difficulty of assistance, 23 our experience has been that this is not the case, with no reported difficulties of robotic assistance in any of the 44 cases.
To date, there have been three comparative studies of more than 50 patients looking at RAPN and LPN comparing oncologic and functional outcomes; not only do these show no negative impact on oncologic outcome, but they also they show a decrease in WIT, intraoperative bleeding, and hospital stay in the RAPN group and no significant difference in perioperative or postoperative complications. 24 –26 When our series is viewed as a whole and compared with the comparative series of 1,800 patients undergoing LPN or open partial nephrectomy by Gill and associates, 12 we see an improvement in WIT and EBL in both groups (Table 5). Our WITs are comparable to those seen in the 235 patients in the single surgeon laparoscopic series, published by Gill and colleauges, 13 in which an early unclamping technique was used.
WIT=warm ischemia time; EBL=estimated blood loss; LOS=length of stay.
Alongside these improvements in operative and functional parameters, there is no evidence of an increase in positive margin rates in RAPN, with our series demonstrating a rate of 5.8%. Previous RAPN series have demonstrated a range of 0% to 5.7%, 23 –35 which is comparable to the 2.85% in the largest LPN series to date. 12 The slightly higher rate of 5.8% in our series is most likely to be because the series accounts for the entirety of the surgeons' learning curve, and we would expect to see this number decrease over time.
There have been concerns raised in the past about the reliance of the operating surgeon in RAPN on their patient-side assistant. 29,36 We have not found this to be a problem, with no reported adverse events that could be put down to the assistant. It is important to mention that all assistants were operating with experienced renal surgeons and had received appropriate tableside training/mentoring before assisting with an RAPN.
This study is not without its limitations. The small sample size makes commenting on rare occurrences, such as positive margin rates and major complications, difficult, and although inferences can be made from the data presented in this article, larger data sets are needed before these inferences can be confirmed. A further limitation relates to the lack of randomization; this opens the series up to potential selection bias.
Conclusion
NSS has become the recommended treatment for amenable T1 RCC. 1 This series adds to the growing body of evidence that RAPN offers a minimal access approach to partial nephrectomy with a shorter learning curve than the traditional laparoscopic approach and with no apparent adverse effects on functional and oncologic outcome.
When a comparative analysis between retroperitoneal and transperitoneal approaches was performed, no significant difference in WIT was seen, along with a significant reduction in total operative time and EBL in the retroperitoneal group. More work is needed further comparing the two techniques, but if this trend is confirmed by subsequent series, it opens up the possibility of varying surgical approach, depending on tumor location, thereby optimizing minimal access surgery for all renal masses.
Footnotes
Disclosure Statement
No competing financial interests exist.