
Abstract
Background and Purpose:
Surgical treatment of patients with prostate cancer currently involves laparoscopic radical prostatectomy (LRP) or robot-assisted LRP. Continence and nerve-sparing procedures in these techniques are supported by dissection and hemostatic surgical devices powered by different types of energy. The aim of this study was to assess recovery of continence and erectile function after laparoscopic extraperitoneal radical prostatectomy comparing two surgical devices for dissection and hemostasis—radiofrequency (RF) and ultrasound (US) scalpels.
Patients and Methods:
A total of 132 men with localized prostate cancer were prospectively enrolled and scheduled for extraperitoneal LRP. Patients were randomly assigned to the RF group (LigaSure; n=66) or the US group (UltraCision; n=66). Outcomes were measured by the self-administered questionnaires (International Consultation on Incontinence Questionnaire–Urinary Incontinence [ICIQ-UI] and International Index of Erectile Function 5 [IIEF 5]) 15 days before surgery, 90 and 180 days after prostatectomy to assess recovery of urinary continence and erectile function.
Results:
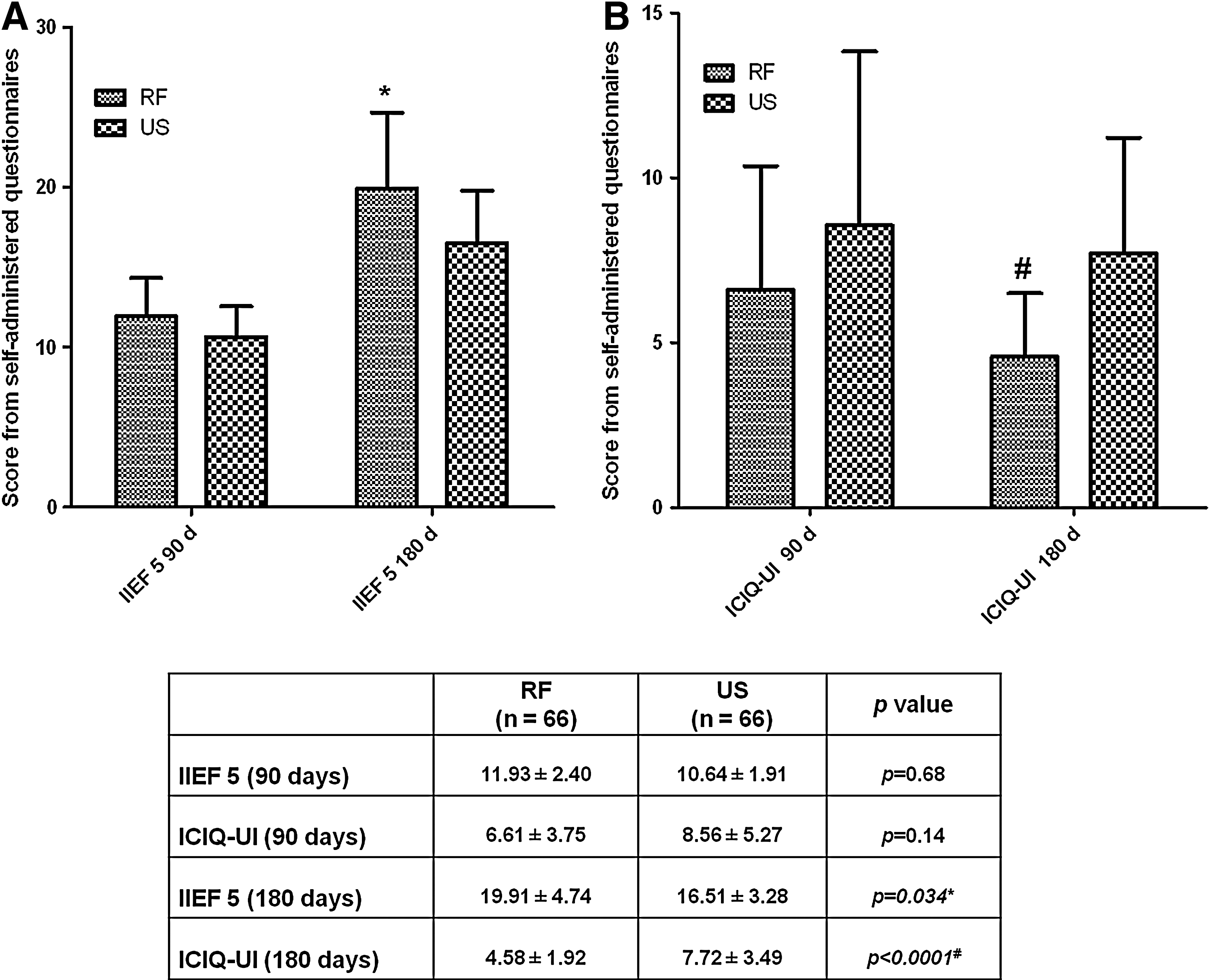
No significant difference was found between the two groups regarding operative time, intra- and perioperative complications, or time of hospital stay. At 180 days after surgery, patients in the RF-treated group showed better recovery in terms of continence and erectile function compared with patients in the US group (ICIQ-UI: p=0.0016; IIEF 5: p=0.0352).
Conclusions:
The use of the RF scalpel provided better functional outcomes compared with the US scalpel in patients undergoing extraperitoneal LRP. This might be attributed to the low contiguous damage of those tissues, which are not directly involved in dissection and hemostasis, achieved using the RF device.
Introduction
The current mean age of patients with a diagnosis of prostate cancer is significantly lower than in the past two decades. Therefore, it has become important to develop appropriate surgical procedures that ensure the greatest chance of recovery from urinary incontinence and erectile dysfunction. Both radiofrequency (RF) and ultrasound (US) scalpels are routinely used during LRP because they offer good support for dissection and hemostasis, minimizing operative time and blood loss. Despite the widespread use of these scalpels in laparoscopy, there are few studies comparing these devices in terms of functional outcomes after radical prostatectomy. The aim of the present study was to compare RF and US scalpels with respect to the recovery of urinary continence and erectile function in patients undergoing extraperitoneal LRP (ELRP).
Patients and Methods
A total of 132 men were prospectively enrolled during the period between September 2009 and December 2011. All patients provided written informed consent before enrollment in the study. This study was conducted in accordance with the Declaration of Helsinki and was approved by the local Medical Ethical Committee (ASL LT CE approval n.2009/09/119).
All patients had received a diagnosis of prostatic adenocarcinoma, as determined by transperineal ultrasonography-guided biopsy after preliminary clinical evaluation involving digital rectal examination (DRE) and assessment of serum prostate-specific antigen (PSA) levels (total PSA, free-PSA, and ratio). Clinical staging of the disease was determined in all patients by abdominopelvic magnetic resonance and whole-body bone scintigraphy. Baseline characteristics of the patients are summarized in Table 1. All patients satisfying the following preoperative criteria, according to European Association of Urology guidelines, 8 underwent bilateral nerve sparing (NS) ELRP: PSA ≤10 ng/mL; life expectancy >10 years; no extracapsular disease, negative DRE, IIEF score ≥22; ICIQ score <6, no more than two positive cores per lobe, primary Gleason pattern=3.
RF=radiofrequency; US=ultrasound; SD=standard deviation; PSA=prostate-specific antigen; BMI=body mass index.
Preoperative (15 days before ELRP) and postoperative (90 and 180 days after ELRP) evaluation of continence and erectile function was performed for all patients with the following two self-administered questionnaires: (1) the International Consultation on Incontinence Questionnaire–Urinary Incontinence Short Form (ICIQ-UI Short Form), 9 a condition-specific, quality of life questionnaire developed by the International Continence Society for patients with urinary incontinence, and (2) the International Index of Erectile Function 5 (IIEF 5), 10 a multidimensional scale developed to assess the five central domains of male sexual function (erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction). Preoperative urinary continence was defined as an ICIQ score <6, and normal erectile function was considered when an IIEF-EF domain score was ≥22; patients who did not meet these criteria were excluded from this study. The same score parameters were used to assess the recovery of postoperative continence and sexual function.
After stratified randomization to control for baseline covariates, the patients were randomly assigned to group A (RF; n=66) or group B (US; n=66). Both groups then underwent ELRP under general anesthesia. In group A, ELRP was performed with the use of an RF scalpel (LigaSure™-8 generator with LigaSure RF scalpel, vessel-sealing system V 5-mm forceps; ValleyLab, Tyco Healthcare). In group B, ELRP was performed with the use of a US scalpel (UltraCision® Harmonic scalpel generator 300 with 5-mm 36p Harmonic Ace forceps; Ethicon Endo-Surgery, Inc.). The same surgeon performed all operations using the bilateral standard (interfascial) NS technique. Only bilateral NS procedures were included in this study.
In all procedures, the dissection of the neurovascular bundles was started at the base of the prostate and continued toward the apex. Two small arteries entering at the prostate base are usually identified at the beginning of the dissection; the two hemostatic devices were used to ensure hemostasis of the vessels. After the correct plane was opened, the dissection occurred on an essentially avascular plane. RF or US was used to seal the pelvic lymphatic tissues and dorsal vein complex and to dissect the bladder neck, vasa deferentia, seminal vesicles, lateral pedicles from the base to the apex of the prostate, and the puboprostatic ligaments. No other energies, such as monopolar or bipolar cautery, or hemostatic (metallic or Hem-o-lok) clips, were used. Urethrovesical anastomosis was performed according to Simone and associates. 11 Cystography was performed for all patients 6 days postoperatively, and if satisfactory, the catheter was removed. In case of leakage from the anastomosis, the catheter was retained for an additional 5 to 10 days, after which cystography was repeated.
All patients were clinically evaluated 30 days after removal of the catheter. Patients who did not spontaneously recover continence underwent a pelvic floor rehabilitation protocol (three sessions/week, up to 8 weeks). Patients who did not spontaneously recover erectile function received sildenafil (100 mg; twice a week, up to 8 weeks). Patients who had not recovered erectile function with sildenafil were treated with intracavernous prostaglandin therapy.
Statistical analyses
Statistical analysis (Student t test) was performed to compare self-administered questionnaire scores using SPSS (version 12.0; SPSS Inc., Chicago, IL). P values <0.05 were considered statistically significant.
Results
Age and body mass index were similar in both groups. Perioperative data did not differ significantly between the two groups. All perioperative data are summarized in Table 1.
Surgical complications were evaluated basing on Clavien classification. 12 The rates were 7.5% (grade 1), 10.5% (grade 2), and 1.5% (grade 3), and 7.5% (grade 1), 12% (grade 2), and 3% (grade 3), for groups A and group B, respectively (Table 2).
Bladder neck strictures rate was 3.2% (four patients) in group A and 3.9% (six patients) in group B. All patients were treated with transurethral incision of the bladder neck 3 months postoperatively. In group A, 28 (42%) patients reported spontaneous recovery of continence (0–1 pads/day) 30 days postoperatively, 37 (56%) patients at 90 days, and 53 (80%) patients at 180 days (Table 3). At the end of the follow-up, 13 (19%) patients still needed to use two pads per day. In group B, 25 (37%) patients reported spontaneous recovery of continence at 30 days, 34 (51%) patients after a course of pelvic floor rehabilitation at 90 days, and 41 (62%) patients at 180 days.
There were 45 and 55 patients who received supportive therapy (sildenafil and prostaglandin) after the first evaluation at 30 days after surgery, in groups A and group B, respectively.
Statistically significant P value.
RF=radiofrequency; US=ultrasound.
At 30 days after surgery, spontaneous recovery of erectile function was reported by 21 (32%) patients in group A and 11 (17%) patients in group B. After the first evaluation, 45 and 55 patients received supportive therapy (sildenafil and prostaglandin) in groups A and group B, respectively.
At 90 days, 38 (58%) patients in group A and 34 (52%) patients in group B reported recovery of erectile function. At the last follow-up evaluation at 180 days, 56 (84%) patients in group A and 41 (62%) patients in group B reported normal erectile function (Table 3).
Scores on the ICIQ-UI and IIEF 5 showed no significant differences between groups at postoperative day 90 (Fig. 1). Significant differences between groups, however, were observed at postoperative day 180, both for the recovery of continence and erectile function (P<0.0001, P=0.034 respectively).
Discussion
Results of the present study showed that the RF and US scalpels were similar with respect to operative time, blood loss, catheterization time, and postoperative hospital stay. At the 180-day follow-up, however, a better functional outcome was demonstrated for patients in the RF group (LigaSure), as shown by significantly improved ICIQ-UI and IIEF-5 scores compared with the US group (UltraCision), while no significant difference was observed at an earlier time point (90 days).
The ELRP method is a safe, standardized surgical technique with satisfactory oncologic and functional results. 13 Blood loss is minimal compared with the open approach, and transfusion is rarely needed. Stolzenburg and colleagues 13,14 reported a series of 2400 ELRPs with a mean blood loss of 255 mL and a transfusion rate of <1%. In addition, recovery of continence was reported by 71.7% of patients in that series 3 months postoperatively, reaching 94.7% by 12 months. In the first postoperative year, 44% of the patients who underwent unilateral or bilateral NS prostatectomy reported recovery of erectile function at 3 months, reaching 72% by 12 months. 14 Therefore, results reported in our study are consistent with the data in the literature.
Only few studies have compared the transperitoneal vs the extraperitoneal approach for video LRP. Cathelineau and colleagues 15 reviewed 200 consecutive radical prostatectomies with transperitoneal and extraperitoneal approaches performed by two surgeons. Results showed no significant difference in terms of operative, functional, or pathologic data, and the authors concluded that each surgeon should choose his or her preferred route. In contrast, Eden and coworkers 16 reported superiority of the extraperitoneal over the transperitoneal approach with respect to operative time, hospitalization time, and recovery of continence. Cohen and associates 17 retrospectively evaluated 265 patients undergoing transperitoneal or extraperitoneal radical prostatectomy by a single surgeon. The extraperitoneal approach was found to be superior with regard to operative time, hospitalization time, recovery of urinary continence, and complication rate. In a study involving 160 consecutive patients undergoing radical prostatectomy, Porpiglia and colleagues 18 compared the transperitoneal and extraperitoneal approaches and concluded that the extraperitoneal approach needed less operative time and resulted in a faster recovery of continence.
Few studies compared the functional outcomes of energy free ELRP with those obtained using various hemostatic devices. 19,20 Gill and Ukimura 19 compared potency outcomes in 76 patients undergoing either the harmonic scalpel-based (group 1) or the energy-free technique (group 2). Within the entire group, the overall 1-year intercourse rates were better in group 2 (36% vs 70%; P=0.04). In patients completely potent before LRP (Sexual Health in Men score ≥22), the 1-year intercourse rates in group 1 vs 2 were 71% vs 88%, respectively (P=0.4), and erectile function recovered faster in group 2.
There are presently no studies comparing the effects of different surgical devices with respect to dissection and hemostasis in ELRP. This study is the first prospective randomized comparative evaluation of the devices in ELRP.
Most surgeons select a device based on practical aspects, particularly their confidence with the instrument and its simplicity of use. Ideally, the preference of one device over another should depend on technical aspects and objective data. The LigaSure and UltraCision devices present different technical features. The LigaSure vessel-sealing device uses both electrical energy and pressure to liquefy and reform collagen and elastin in the vessel walls and tissues (up to 7 mm in diameter) to provide hemostasis. 21 The device incorporates feedback control, which automatically terminates energy transmission once a seal has been achieved. In contrast, the UltraCision scalpel uses US technology to denature proteins within vessel walls and tissues (up to 5 mm thick), leading to coagulation. 22
Both the LigaSure device and UltraCision scalpel have been demonstrated to be safe and effective in numerous studies. 23 –26 Both devices reduce operative time and make tasks easier for the surgeon. A theoretical assumption of low lateral RF spread of the LigaSure scalpel, however, might be considered a determining factor for more precise surgical dissection and hemostatic steps and lacking involvement of adjacent structures that could be damaged (especially muscle fibers and nerves) by high temperature. 25 It is well known that a thermal effect can be highly detrimental, particularly to nerve fibers, inducing necrotic phenomena and an irreparable process of coagulation necrosis. 26
Currently, we can, and are necessarily required to differentiate decisions concerning some of the surgical steps in radical prostatectomy, especially during dissection of the neurovascular bundles, depending on specific cancer risk. We have to choose whether to perform prostatectomy, whether to perform NS, whether it should be monolateral or bilateral, and finally whether the dissection should be inter-, intra- or extrafascial. Every procedure is customized to the patient.
The main limit of this study could be represented by the sample size and by the mean range of follow-up; however, the prospective design, the execution of all surgical procedures by the same surgeon, and the homogeneous characteristics of the patient groups may balance this study limitation. Additional larger prospective randomized studies with a longer follow-up are necessary to assess other scalpel devices and to encourage surgeons to select a particular device based on an objective demonstration of its superiority.
Conclusion
At postoperative day 180, better functional outcomes (recovery of continence and erectile function) were found in the RF group of patients (LigaSure) compared with the US group (UltraCision). This might result from characteristics of the RF device that maintain a very controlled target during hemostasis and dissection, thus helping to avoid the involvement of adjacent tissues.
Footnotes
Disclosure Statement
No competing financial interests exist.