
Abstract
Background and Purpose:
Radical cystectomy is the mainstay of the management of muscle invasive bladder cancer. Numerous centers have adopted a minimally invasive approach to replace the standard open procedure. The objective of the study was to review published literature comparing laparoscopic radical cystectomy (LRC) and open radical cystectomy (ORC).
Materials and Methods:
A systematic review of the literature according to Cochrane guidelines was conducted (1993 to 2012) for studies comparing LRC and ORC. All studies comparing the two procedures were included. The outcome measures were the patient demographics, operative time, blood loss, transfusion rates, time to oral intake, length of hospital stay, and complications. A meta-analysis was conducted. For continuous data, a Mantel-Haenszel chi-square test was used, and for dichotomous data, an inverse variance was used, each expressed as risk ratio with 95% confidence interval. P<0.05 was considered significant.
Results:
Four hundred twenty-seven patients were included—211 patients in the laparoscopic group and 216 patients in the open group (eight studies). There was no significant difference between the two groups in any of the demographic parameters except for age (age: P<0.0001; sex: P=0.1; body mass index: P=0.05). The laparoscopic group had significantly longer operative times (P<0.0001), but less blood loss (P<0.00001), less transfusion rates (P<0.0001), less time to oral intake (P<0.0001), less analgesic requirement (P=0.0009), and shorter length of hospital stay (P<0.0001). Significantly more minor complications developed in the ORC group than in the LRC group (P=0.02). There was no difference between the two groups regarding lymph node dissection yields, major complications, positive margins, pathologic results, local recurrence, or distant metastases (all P>0.05). There were significantly more positive nodes in the ORC group, however.
Conclusion:
In experienced hands, LRC is a feasible and safe alternative to ORC with less blood loss, transfusion and analgesic requirement, shorter lengths of hospital stay, and less complications. LRC does, however, have longer operative times.
Introduction
As it stands, almost 50% of patients who undergo ORC will have a tumor recurrence, while the 5-year survival rates have been reported to range between 73% and 89% in node-negative, organ-confined disease, reducing to 45% to 55% with extravesical disease, and 25% to 35% with nodal involvement. 1,5,7 These results are also echoed in reports of LRC series with short-term oncologic outcomes. 3 To try to improve survival, centers have adopted an extended pelvic lymph node dissection approach. 1 This has also been undertaken as part of the laparoscopic procedure; however, no long-term results are available. 8,9
The complication rate of ORC is in the range of 40% to 65% with a transfusion requirement of around 66%, while the major complication rates range between 10% and 12% with a mortality of 2% to 3%. 1,5 LRC can also provide an advantage of less blood loss, analgesic requirement, reduced scarring, and fewer complications. 2,10 –13 Despite these advantages, LRC is a technically challenging procedure that requires a high level of laparoscopic skills and has a long learning curve. 1,2 Numerous reports have emerged showing success with the procedure, however. 4 Furthermore, reports of head to head comparisons between ORC and LRC have also been reported. 11 –14
To this end, we conducted a systematic review of the literature with a meta-analysis to determine whether there were any differences between the operative and postoperative outcomes in addition to oncologic outcomes between these two approaches and whether or not LRC can be an appropriate alternative.
Materials and Methods
Literature review and article selection
The systematic review was conducted in line with both Cochrane and PRISMA guidelines. The following search engines were used: MEDLINE (1993–August 2012), EMBASE (1993–August 2012), Cochrane Central Register of Controlled Trials - CENTRAL (in The Cochrane Library - Issue 3, 2012), CINAHL (1993–August 2012), Clinicaltrials.gov, Google Scholar, and individual journals. The search was conducted on February 9, 2012.
Search terms used included: Cystectomy, Laparoscopic, Laparoscopy, Bladder Cancer, Bladder Neoplasm, Radical Cystectomy, Laparoscopic Radical Cystectomy, and Open Radical Cystectomy.
Mesh phrases included: (“Cystectomy”[Mesh]) AND “Laparoscopy”[Mesh]), ((“Comparative Study” [Publication Type]) AND “Cystectomy”[Mesh])), (((“Comparative Study” [Publication Type]) AND “Cystectomy”[Mesh]) AND “Laparoscopy”[Mesh]).
Non-English language articles were included if data were extractable; also, references of searched papers were evaluated for potential studies for inclusion. The contact author of the studies was e-mailed for clarification wherever the data were not clear or data were missing.
Data extraction and analysis
All types of studies comparing LRC with ORC were included. The main outcome was to assess the perioperative results in addition to the oncologic results between the outcomes of the two procedures. The cost analysis was set as a secondary outcome measure. Data extraction from each study included: Patient demographics, operative time, blood loss, and transfusion rates, time to oral intake, analgesic requirement, and length of hospital stay, positive surgical margins, lymph node yield, cystectomy pathology results, and complications. Only similar data were grouped into a pooled meta-analysis.
The Mantel-Haenszel test was used for continuous data and expressed as the mean difference while an inverse variance was used for dichotomous data and expressed as risk ratio, both of which, with 95% confidence interval (CI). P value for significance was set at <0.05.
Heterogeneity was analyzed using Review Manager (RevMan) 5.0.23. 15 Heterogeneity was considered low, medium or high if I 2 values were 25%, 50%, or 75%, respectively. A fixed-effect model was used in all analyses; however a random-effects model was used if heterogeneity existed.
The methodologic quality of each study was assess using Cochrane guidelines. 15,16 We used RevMan 5.0.23 to analyze the meta-analysis.
Results
Literature search
The literature search yielded 342 studies, of which 301 were excluded because of nonrelevance based on titles and 13 excluded because of nonrelevance to this review by not comparing LRC with ORC, based on the abstracts (Fig. 1). Abstracts were evaluated in 41 studies, of which 13 were excluded because of nonrelevance, and full articles were evaluated in the remaining 28 studies, of which 8 were included into the systematic review. 11,13,14,17 –21 All of the included studies reported on various outcomes that were suitable to be pooled into a meta-analysis. The majority of the studies were published within the last 5 years, reflecting the increasing use of LRC.

Flowchart for article selection process of the review.
After reading the full manuscripts, we excluded 20 studies for reasons noted below. Eight of the studies were large case series of their institute's experience of LRC and did not compare LRC with ORC. 4,19,22 –27 Taylor and colleagues 28 compared hand-assisted LRC with ORC while Wang and coworkers 29 compared hand-assisted LRC with pure LRC. Neither study compared LRC with ORC, hence were excluded. Chlosta and associates 8 only compared the lymph node dissection of LRC and ORC with no other outcomes for this reviewl therefore, they was excluded. The remaining nine articles were either review articles or articles that reported on various aspects of LRC without comparison with ORC; hence, they also were excluded. 3,6,9,30 –35
Characteristics of the included studies
Although the literature search was conducted between 1993 (first reported cases of LRC) and 2012, comparison studies were published between 2004 and 2010. Two were conducted in Italy, two in the United States, one in Korea, one in China, one in India, and one in France. A total of 427 patients were included in this review—211 in the LRC group and 216 in the ORC group. The LRC group had an age range of 58.2 to 66.8 years with 189 men, while the ORC group's age range was between 55.9 and 71 years with 183 men.
All the included studies were cohort observational studies, with no randomization and all reported on their center's experience with LRC compared with ORC. All the studies reported on various outcome aspects of this review, which are plotted into Table 1, Figure 2, and Figure 3. All the studies reported on patient ages, sex, and type of urinary diversion. Seven studies reported patients' body mass index (BMI) status. 11,13,14,17 –19,21 Guillotreau and coworkers 11 mention which groups had patients with previous abdominal surgery, while Ha and colleagues 18 excluded those patients; otherwise, there was no mention from the other studies in this regard. The article from Haber and associates 19 referenced a published abstract; however, in the article, they provide further information that allowed for extraction of the data and analysis of risk of bias for their study and were therefore included.

Lap=laparoscopic; BMI=body mass index.
Five of the studies either mention their learning curve for the LRC procedure was surpassed and/or did not include those patients in their analysis, 11,13,18,19,21 while three studies did not. 14,17,20
All the studies reported on the operative times, blood loss, and lengths of hospital stay. Seven studies reported on time to oral intake. 11,13,14,18 –21 Six reported on the transfusion requirement. 11,13,14,18 –20 Six studies reported on the lymph node yield dissected. 11,13,17 –20 Four studies reported on the morphine analgesic requirement. 11,13,14,18 Five studies reported on the complication rates. 11,13,14,19,20 All the studies reported on the stage of the final pathology results. Six studies reported on whether or not nodes were positive, 11,13,14,18 –20 while five reported on positive margins. 11,13,14,18,19 Four studies reported on length of follow-up. 11,13,18,20 Two studies reported on local recurrence, 13,18 three on distant metastases, 13,18,20 two on overall survival, 13,18 two on disease-specific survival, 18,20 and two on disease-free survival rates. 13,18
The data of studies that were in means±standard deviation or rates, which allow for a meta-analysis, were pooled and analysed (Figs. 2 and 3).
Meta-analysis results
Table 1 depicts the demographics of the studies, including number of patients, age, sex, urinary diversion, and BMI. There was no significant difference between the two groups for any of the basic demographic parameters except for age where the ORC groups were significantly younger (age: P<0.00001; mean difference (MD): 7.65, 95% CI: 4.85, 10.45; male sex: P=0.1; odds ratio (OR): 1.66, 95% CI: 0.91, 3.02; female sex: P=0.1; OR: 0.60, 95% CI: 0.33, 1.10; BMI: P=0.05; MD: −0.16, 95% CI: −0.84, 0.51). Furthermore, the ORC group had significantly more ileal conduit formations than the LRC group: P=0.003; OR: 0.43, 95% CI: 0.25, 0.74. Conversely the LRC group had significantly more neobladder formations than the ORC group: P=0.002; OR: 2.36, 95% CI: 1.36, 4.10.
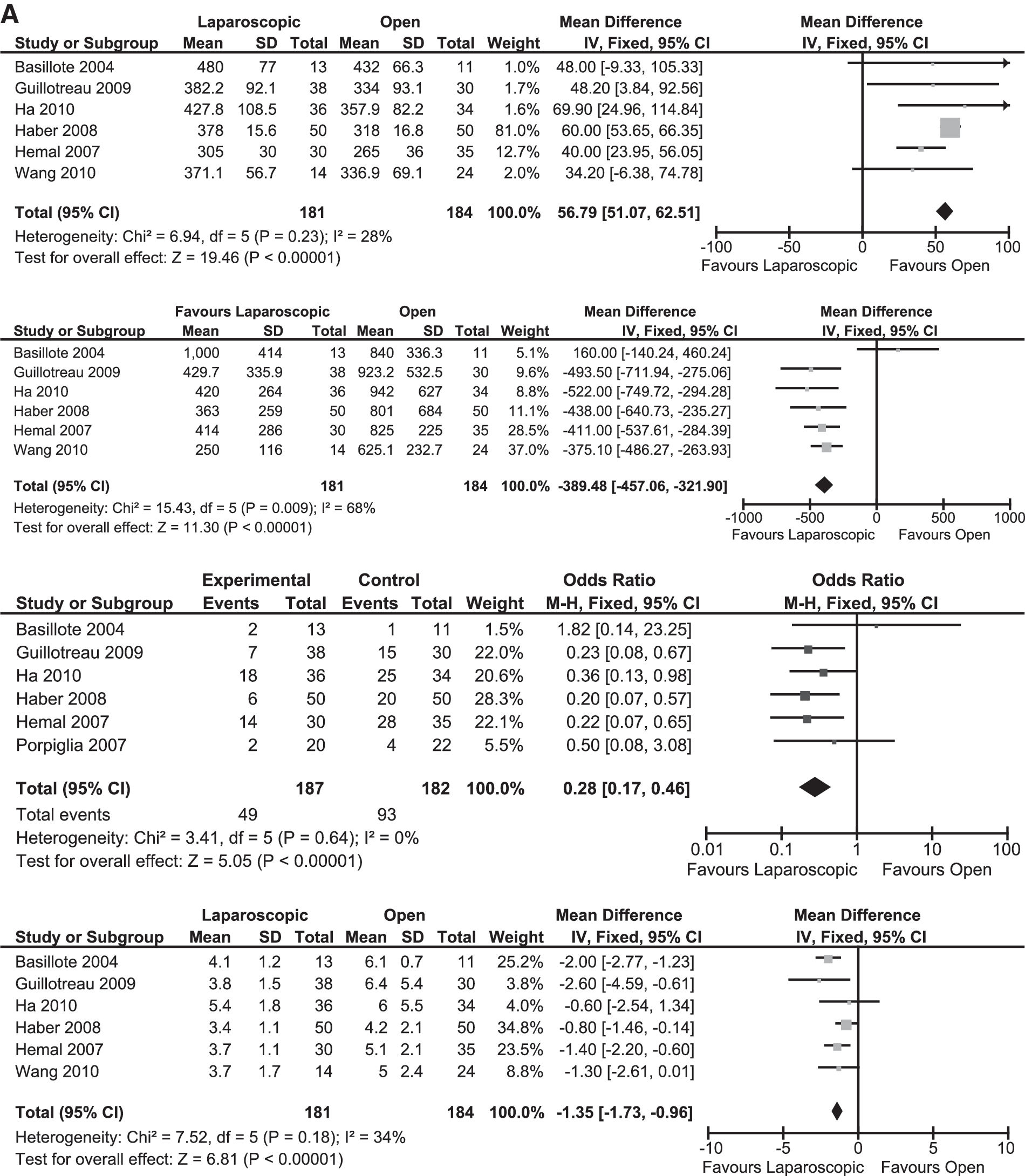
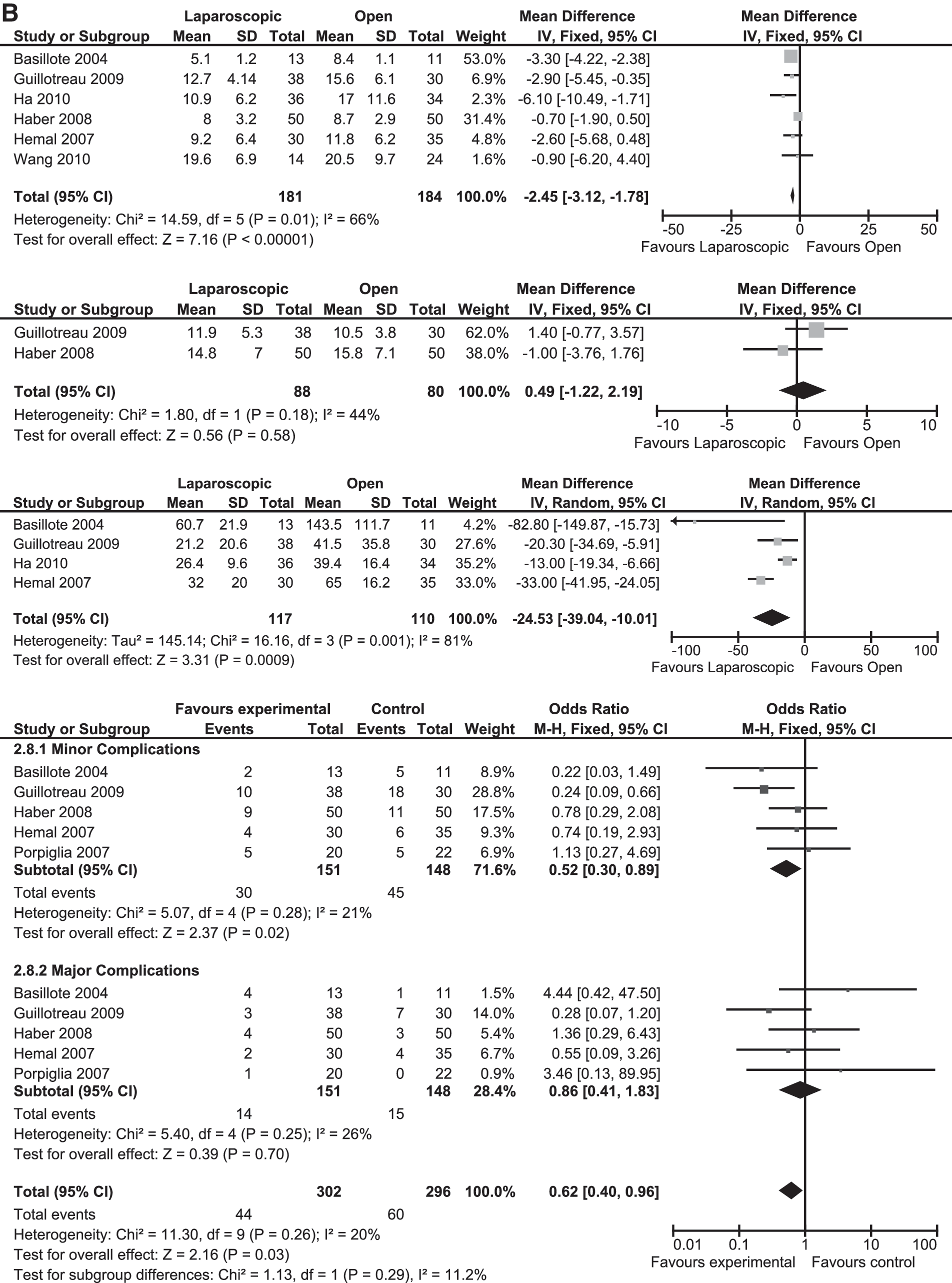
The LRC group had significantly longer operative times than the ORC group (P<0.00001; MD: 56.79, 95% CI: 51.07, 62.51). The LRC group, however, had significantly less blood loss, less transfusion requirement, less time to oral intake, less length of postoperative hospital stay, and significantly less analgesic requirement (blood loss: P<0.00001; MD: −389.48, 95% CI: −457.06, −321.90; transfusion rate: P<0.00001; OR: 0.28, 95% CI: 0.17, 0.46; oral intake: P<0.00001; MD: −1.35, 95% CI: −1.73, −0.96; length of hospital stay: P<0.00001; MD: −2.45, 95% CI: −3.12, −1.78; analgesic requirement: P=0.0009; MD: −24.53, 95% CI: −39.04, −10.01). No difference was found regarding the lymph node dissection yields between the two groups P=0.58; MD: 0.49, 95% CI: −1.22, 2.19) (Fig. 2).
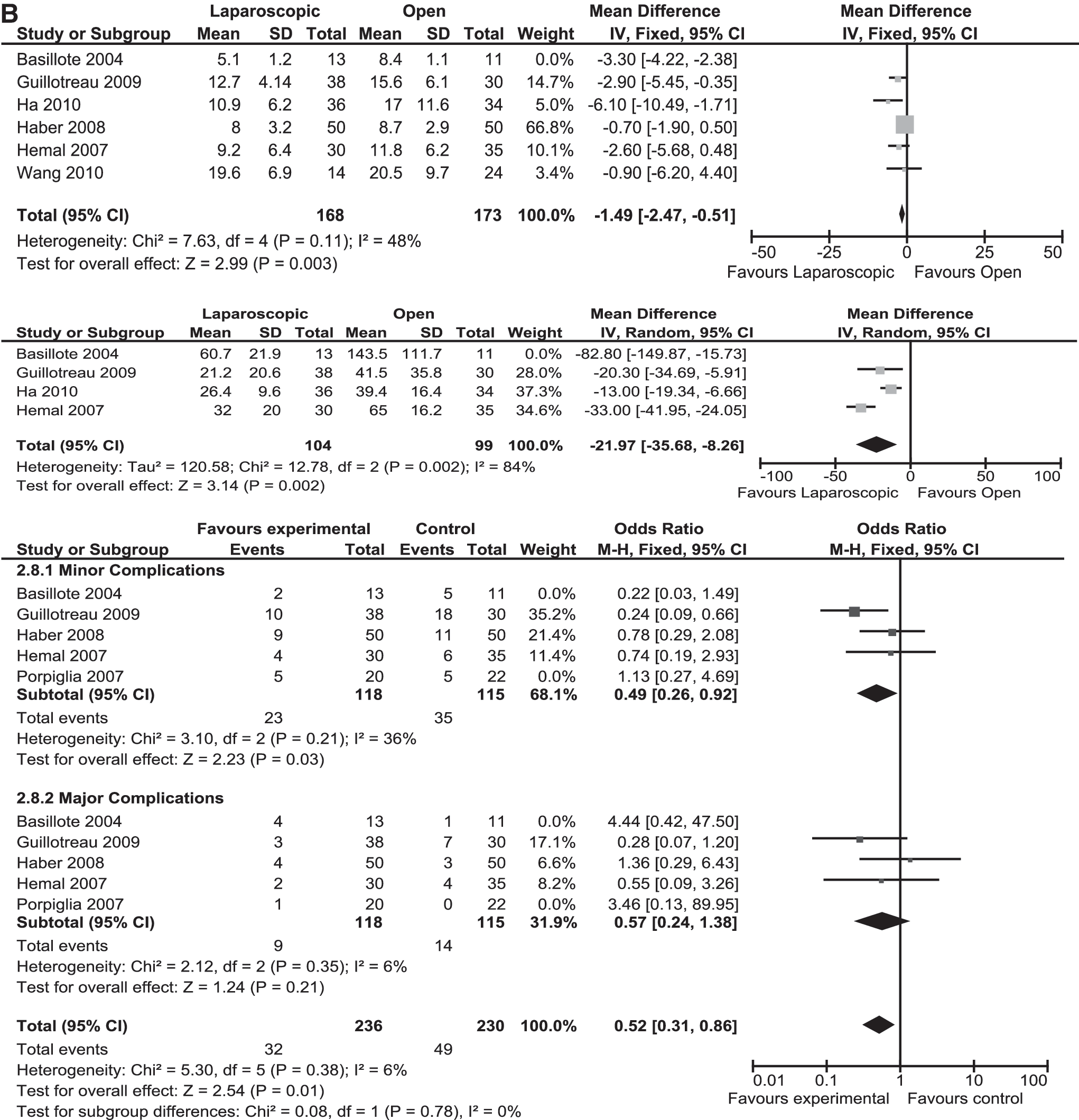
There was no statistical difference between the two groups regarding occurrence of major complications (P=0.70; OR: 0.86, 95% CI: 0.41, 1.83); however, significantly more minor complications developed in the ORC groups than in the LRC group (P=0.02; OR: 0.52, 95% CI: 0.30, 0.89) (Fig. 2).
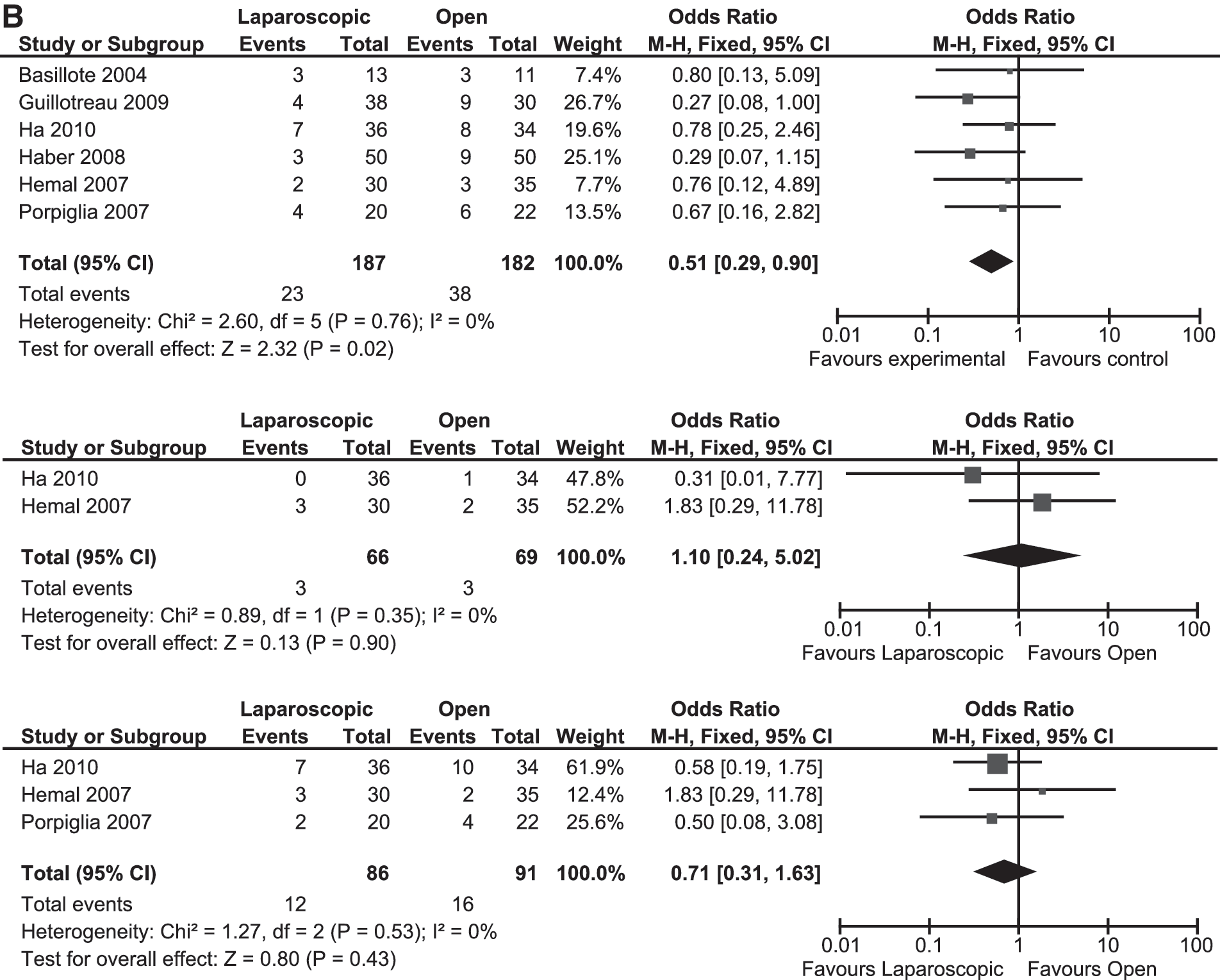
There was no difference between the LRC and the ORC groups regarding oncologic outcomes, except the nodal positive rate was significantly more in the ORC group (positive margins: P=0.12; OR: 0.43, 95% CI: 0.15, 1.25; at least pT2N0: P=0.31; OR: 1.23, 95% CI: 0.83, 1.82; pT3–4N0: P=0.61; OR: 0.90, 95% CI: 0.60, 1.35; node positive: P=0.02; OR: 0.51, 95% CI: 0.29, 0.90; local recurrence: P=0.9; OR: 1.10, 95% CI: 0.24, 5.02; distant metastases: P=0.05; OR: 0.43, 95% CI: 0.31, 1.63) (Fig. 3).
Subgroup analysis
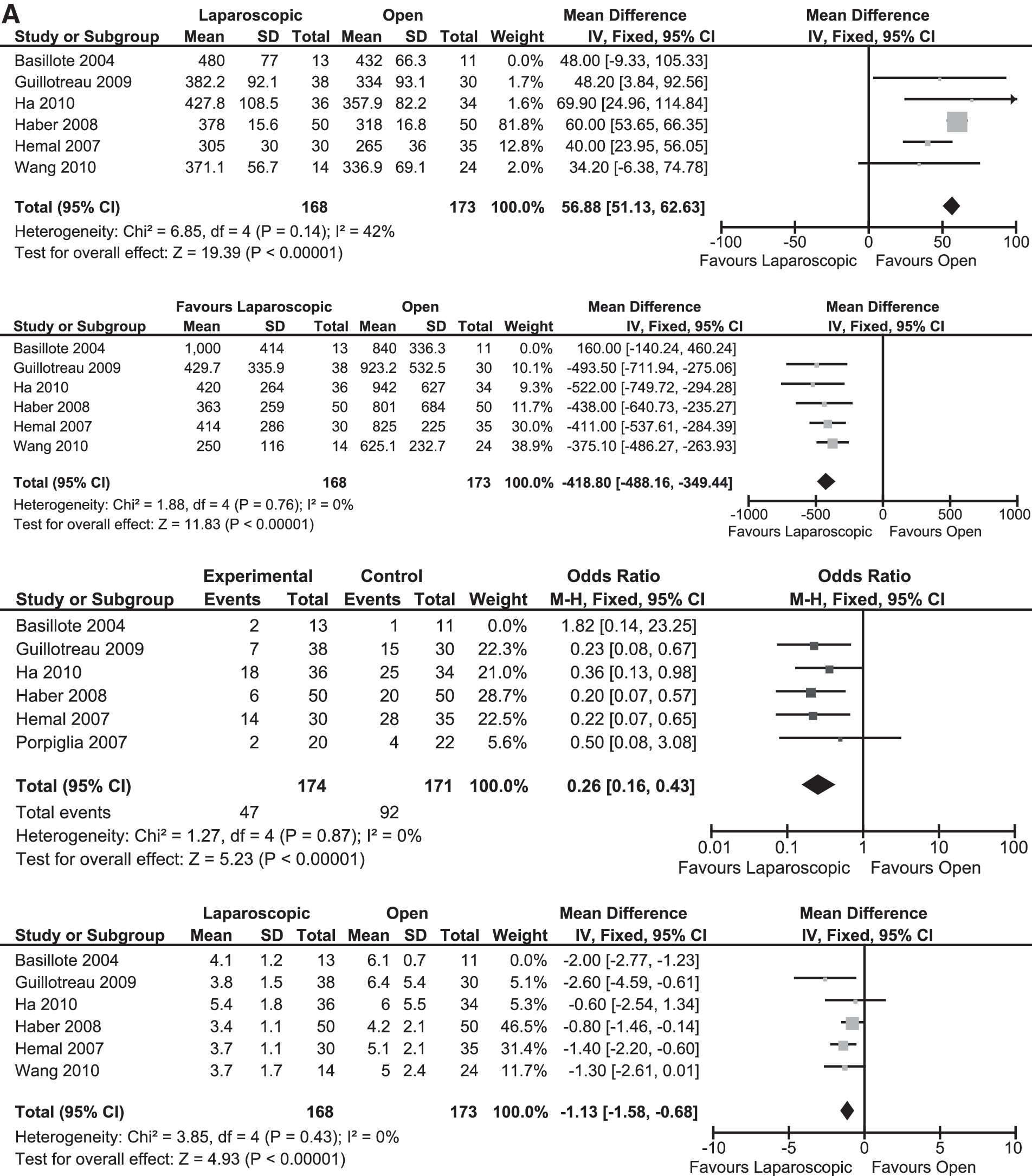
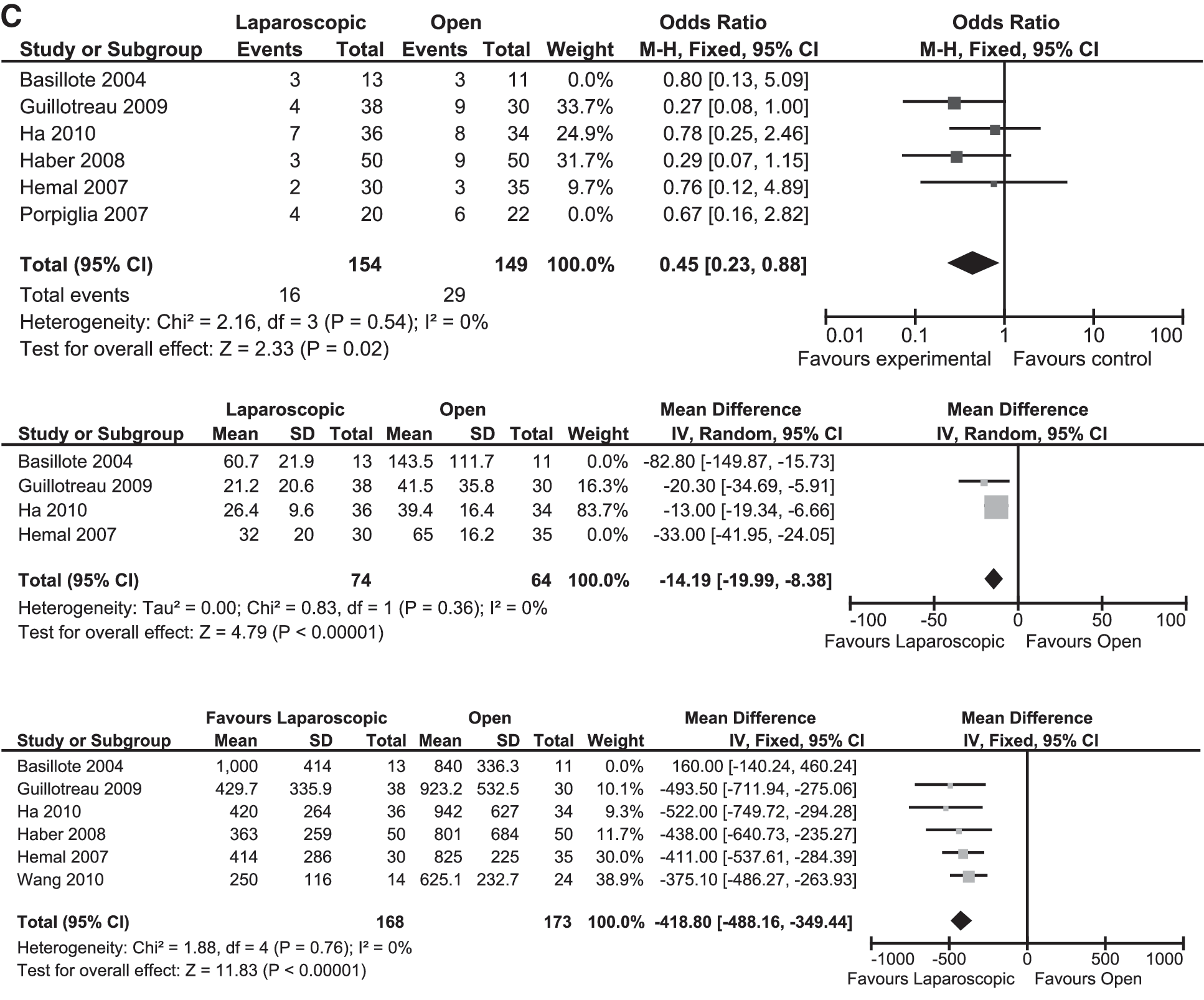
Excluding the studies that included patients within their learning curve (Fig. 4), we found that the LRC group still had significantly longer operative times than the ORC group (P<0.00001; MD: 56.88, 95% CI: 51.13, 62.63), in addition to significantly less blood loss (P<0.00001; MD: −418.8, 95% CI: −488.16, −349.44), less transfusion requirement (P<0.00001; OR: 0.25, 95% CI: 0.15, 0.42), less time to oral intake (P<0.00001; MD: −1.13, 95% CI: − 1.58, −0.68), less analgesic requirement (P<0.002; MD: −21.97, 95% CI: −35.68, −8.26), and less length of postoperative hospital stay (P<0.003; MD: −1.49, 95% CI: −2.47, −0.51). Significantly more minor complications developed in the ORC group than in the LRC group (P<0.003; OR: 0.49, 95% CI: 0.26, 0.92). There were more positive nodes in the ORC group than in the LRC group (P<0.02; OR: 0.45, 95% CI: 0.23, 0.88).
Methodologic quality assessment
All the studies were observational controlled studies, four of which were conducted in a retrospective manner comparing the results of the two groups in a historic manner 14,17 –19 while the other four were prospectively conducted with the two comparative arms running compared prospectively. 11,13,20,21 Figure 5 depicts the methodology quality assessment based on the authors' judgments of risks of bias.

Quality assessment (risk of bias summary: review authors' judgments about each risk of bias item for each included study).
Three of the studies had a high risk of selection bias based on a significant difference between the two groups from the start of the study. Guillotreau and colleagues 11 had more patients in the ORC group with previous abdominal operations, while Ha and associates 18 had an older age group in the LRC group, and Porpiglia and coworkers 20 had an older age group of patients in the ORC. A subgroup analysis was conducted by removing the results of the studies with high risk of selection bias; however, this did not yield any changes to the end results. Therefore, a report of the final analysis was not necessary.
Furthermore, none of the studies was randomized or blinded with the ORC group considered the control group. Otherwise, the studies had low risk of bias in all other categories.
Discussion
Summary of the main results
This review found that patients who underwent ORC had a significantly shorter operative time; however, they had more blood loss, more transfusion requirement, took longer time to oral intake, had a longer length of hospital stay, and needed more analgesics to control pain when compared with patients who underwent LRC (Fig. 2). Furthermore, ORC patients were at risk of the development of significantly more minor complications than those undergoing LRC (Fig. 2). Patients undergoing ORC were significantly younger than those undergoing LRC, which indicates that LRC can safely accommodate a wider age range than its open counterpart. Furthermore, the ORC group had significantly more ileal conduit formation despite no difference between the two groups regarding cancer staging (Figs. 2 and 3). This could possibly explain why LRC procedures had longer operative times, because it is well established that neobladder formation takes longer to fashion than ileal conduits. 36 –38
To further evaluate the outcomes based on experience and removing the learning curve factor, we conducted a subgroup analysis whereby all studies that included their learning curve patients were excluded and only those that mention that the learning curve was surpassed or patients in the initial curve period were not included into the comparison were pooled. 11,13,18,19,21 We did not find any change to the final comparative outcome (Fig. 4). The LRC group still had significantly longer operative times than the ORC group, in addition to significantly less blood loss, less transfusion requirement, less time to oral intake, less length of postoperative hospital stay, and the ORC group still developed significantly more minor complications than the LRC group (Fig. 4).
There was no significant heterogeneity (>75%) found in any of the comparisons other than analgesic requirement (I 2 =84%). We attributed this to the significantly higher dosages of analgesics used by Hemal and associates 13 as opposed to Ha and colleagues 18 and Giullotreau and coworkers 11 (Fig. 3). This was confirmed by removing Hemal and associates 11 from the analysis, which reduced the heterogeneity to 0% with no change in the significance of analgesic requirement favoring LRC patients (Fig. 4).
Medium leveled heterogeneity (50%–75%) was seen in the blood loss analysis, which was attributed to one study and included their learning curve patients. 14 When removed from the analysis, the heterogeneity reduced to 0% with no change in the significance outcome (Fig. 4). Furthermore, the length of hospital stay analysis had a medium leveled heterogeneity; however, no cause was found for this. The remaining analysis had either no or low leveled heterogeneity, and no further subgroup analysis was performed.
Although all the studies had a subtle variation with their findings, the pooled meta-analysis results emulated the majority of the studies in most outcomes and gave a more precise collective impression for each comparative outcome. Five of the studies reported LRC had less blood loss 11,13,18,19,29 and four reported less transfusion requirement, 11,13,18,19 while only one study reported that the ORC group had less blood loss. 14 Four studies found there was shorter hospital stay in the LRC groups, 11,14,17,18 and a further four found the LRC group needed less time to oral intake. 11,14,19,20 Five studies found the LRC group needed less opioid analgesics. 11,13,14,18,20 Five studies found the ORC group had shorter operative time. 11,13,17 –19 Otherwise, there was no significant difference between other parameters in each of the studies (Figs. 3 and 4).
These findings suggest that the natural progression of surgical intervention leans toward minimally invasive surgery; however, to date only short- to medium-term (1–5 years) oncologic results have been reported. With no long-term oncologic data reported, validation to whether or not laparoscopic surgery is superior to open and can replace it cannot be determined. Nonetheless, the evolution of surgery is to progress forward, and time will establish which technique is superior.
Cost analysis
Of the studies that compare LRC and ORC procedures, the study by Gregori and colleagues 17 was the only study to report the cost analysis between the two procedures. Hence, we were unable to conduct a further meta-analysis on cost. Nonetheless, we report their findings. At their institute, the cost for surgery, hospital stay, and surgical consumables per patient per day for the LRC procedures was 637 Euros (about $816) and 270 Euros (about $345) for the open group. taking into account various postoperative costs, however, Gregori and associates 17 actually found that the LRC groups were cheaper. They reported that, on average, the total costs for the LRC procedure were 10,626 Euros (about $13,615) while the ORC procedure cost 14,465 Euros (about $18,534). The shortened postoperative hospital stay accounted for less expenditure for the LRC group, which gave it a cost advantage over the ORC group. As with the lack of long-term oncologic data, however, costs of further investigations, procedures, and follow-ups need to be taken into consideration.
Future implications
With the emergence of robot-assisted surgery, robot-assisted radical cystectomy (RRC) has emerged as not only an alternative for LRC but also for ORC. In an observational study, Benito and coworkers 39 compared LRC and RRC and reported that RRC had significantly less blood loss, fewer transfusion requirements, and less days to oral intake. Furthermore, they report that RRC had less intraoperative (1 vs 3) and postoperative (3 vs 11) complications than the LRC counterpart. Otherwise, no significant difference was found between the two procedures regarding operative times and length of hospital stay.
While in the only randomized trial reported in the literature that compares ORC and RRC, Nix and associates 40 reported that RRC had significantly less blood loss, time required to passing flatus and bowel motion, and less analgesic requirement. ORC, however, had a significantly shorter operative time. Otherwise, no other difference was found between the two procedures regarding length of hospital stay, complications, or pathologic outcomes. These findings were echoed by observational studies that reported similar results. 41,42 Both studies, however, also reported a shorter length of hospital stay in the RRC group. 41,42
In a cost comparison between the two procedures, Lee and colleagues 43 found that although RRC was materially more costly, it was more cost efficient than ORC when the impact of complications was considered. Unlike the study by Gregori and coworkers, 17 study, Lee and coworkers 43 reported that the extended length of stay of the ORC group alone was insufficient to overcome the higher costs of the robotic system. What varied to shift the balance to RRC was the cost impact of complications, whereby ORC's cost of complications was significantly more than RRC if ileal conduit diversion was performed. 43 They reported that RRC remained more costly when the neobladder groups were compared. 43 Nonetheless, RRC reports are emerging with promising results from numerous centers. 2,44 –46 As with LRC, however, longer oncologic outcomes are lacking.
Current literature suggests the view that perioperative outcomes of LRC are considered superior or as good to those of the open procedures, except for length of operative time. Furthermore, similar short-medium–term oncologic outcomes have been reported showing LRC's equivalence to ORC's results (Table 1). 12,13,18,20,47 Whether RRC will supersede LRC and take its place to rival ORC, however, only further comparative studies and time will tell with an interesting look at cost comparison as well.
Another important issue to consider is the role for an enhanced recovery protocol (ERP). Arumainayagam and associates 48 found significantly shorter length of hospital stay in patients who underwent ORC in whom the ERP was implemented as opposed to patients who did not have ERP. This can potentially be emulated in both LRC and RRC groups with similar positive results.
Strengths and limitations of review
The main limitation of this review is the inclusion of observational studies with small patient cohorts. Only five of the studies had more than 20 patients, and all the studies had fewer than a 50 patient cohort. Furthermore, no randomized study was found in the literature comparing ORC and LRC. This leads to a risk of bias of the results. The results of the meta-analysis, however, are emulated by the included studies with similar findings and outcomes, in addition to portraying similar results to LRC series published; hence, this would strengthen the notion that the pooled analysis results can be relied on.
The strength of this review was that it was conducted in an impartial, systematic, and methodical manner in keeping with Cochrane standards. This truly represents the current evidence available in the literature comparing LRC and ORC.
A large, multicenter trial comparing the two procedures is needed. An inclusion of cost analysis between the procedures, including postdischarge convalescence and return to work analysis, an analysis of an ERP effect, in addition to patient and surgeon perspectives regarding pain and overall satisfaction with the procedure must be included. Furthermore, classification of the complications into a standardized system such as the Clavien classification is recommended. 49 More importantly, long-term oncologic outcome studies comparing the two procedures will be the most important factor in deciding which procedure is superior. With increasing experience, RRC may surpass both procedures.
Conclusion
A meta-analysis of the literature reveals that in experienced hands, LRC is a feasible and safe alternative to ORC with significantly less blood loss, transfusion and analgesic requirement, shorter lengths of hospital stay, and less complications. LRC was also found to be more cost effective than ORC. Nevertheless, further studies are needed to evaluate the long-term oncologic comparisons between the two procedures.
Footnotes
Acknowledgment
OMA would like to acknowledge Dr. Isra Ashi for her support and advice.
Disclosure Statement
No competing financial interests exist.