
Abstract
Purpose:
We examined the construct validity (ability to discriminate between experienced and inexperienced subjects) of the chicken crop model in the simulation of laparoscopic pyeloplasty.
Materials and Methods:
Dead chickens were used. The chicken crop and esophagus were used to simulate the human renal pelvis and ureter, respectively. The chicken was positioned in a left lateral position within a pelvic trainer to simulate a right ureteropelvic junction. Fifteen subjects were divided into three groups according to their levels of previous laparoscopic experience. Each subject performed a laparoscopic pyeloplasty with the model using the dismembered Anderson-Hynes technique. Operative time and quality scores were recorded. One-way analysis of variance (ANOVA) was used to detect differences among the groups. A Tukey multiple-comparisons test was used to detect differences between individual groups.
Results:
Those in the most experienced group completed the “laparoscopic pyeloplasty” in an average of 33.80 minutes and got an average quality score of 9.0. Those in the less experienced group averaged 55.20 minutes and 7.0, respectively, and those in the group with no experience averaged 92.60 minutes and 4.0, respectively. There were significant differences in operative time and quality scores between the groups as shown by the one-way ANOVA (P<0.001), and also between the individual groups as shown by the Tukey multiple-comparisons test. There was, however, no significant difference in quality scores between the most experienced group and the less experienced group.
Conclusion:
The chicken crop model exhibits good construct validity and, as such, can be used to reproduce the technical complexity of laparoscopic pyeloplasty.
Introduction
Advances in laparoscopic surgery have brought a change in training methodology. Skill laboratory has become an essential and indispensable component of laparoscopic training programs. Training surgeons outside the operating room translates into better performance and fewer complications. Use of specific training models can be an effective way for surgeons to enhance their laparoscopic skills before operating on patients.
Several training models for LP have been developed in recent years. 4 –11 Among them is a training model using chicken crop reported by Ramachandran and colleagues. 11 We have used this model in our workshop and assessed its construct validity—the ability to discriminate between inexperienced and experienced subjects.
Materials and Methods
Model
A dead, plucked chicken was purchased from a local market. A middle longitudinal incision was made through the neck and thorax to expose the chicken crop and esophagus. The lower segment of the esophagus was ligated, and the crop was thoroughly cleaned and filled with water to simulate the dilated human renal pelvis. The upper segment of esophagus was used to simulate the human ureter. The chicken was then placed in a left lateral position within a pelvic trainer to simulate a right-sided ureteropelvic junction (UPJ) (Fig. 1).

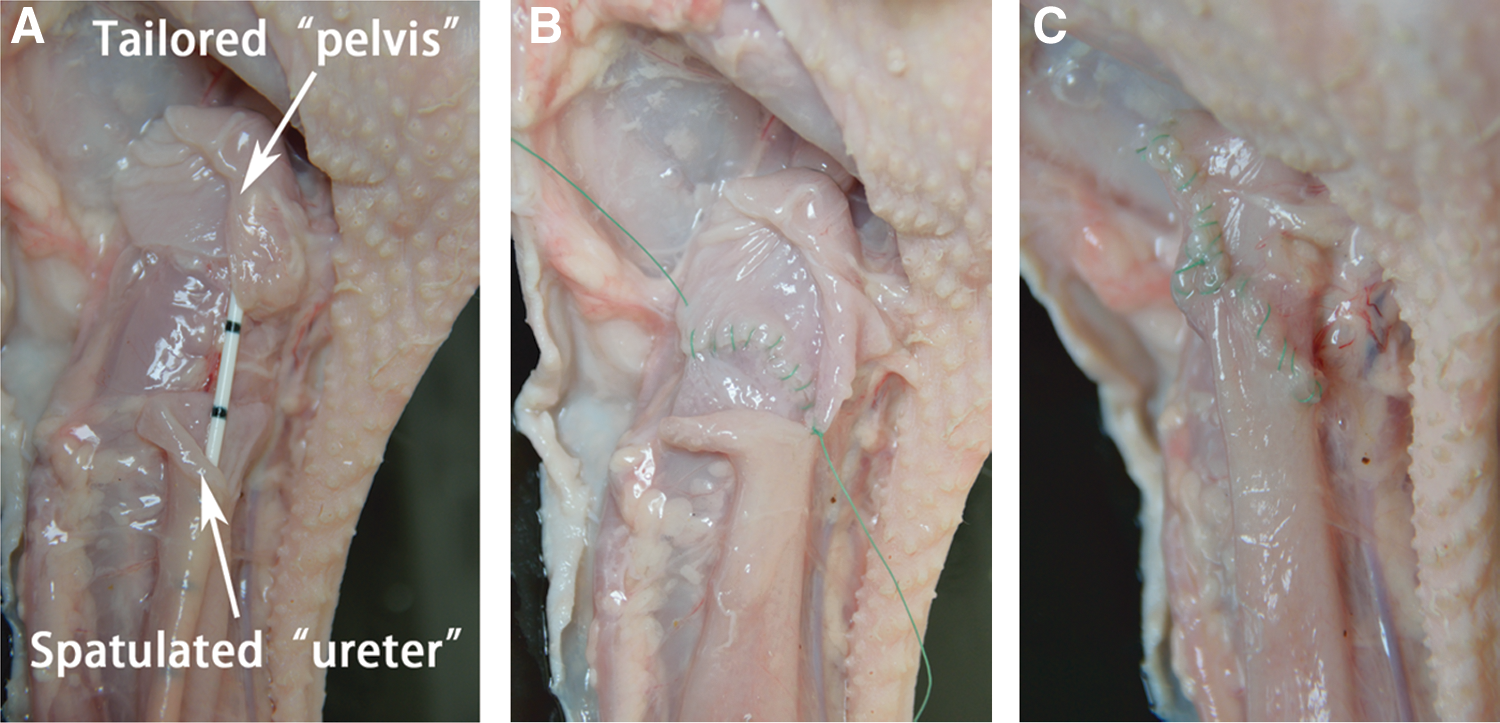
The chicken crop was used to simulate the dilated human renal pelvis, and the upper segment of esophagus was used to simulate the human ureter.
A laparoscopic dismembered Anderson-Hynes pyeloplasty was performed using 4-0 polyglactin sutures (Fig. 2 A–C). At the end of the procedure, 20 mL of water was infused via the upper segment of the esophagus to detect leakage from the anastomosis. The quality of the anastomosis was assessed by an independent observer, who was blinded to the subjects. The criteria used to analyze the quality included exact tissue sutured, equal bite on each side, equal stitch intervals, no tissue tear, and a water-tight anastomosis. The total quality score ranged from 0 to 10 (0 to 2 for each item); the higher the score, the higher the quality.
Study population
Fifteen subjects with different previous laparoscopic experience were divided into three groups. The most experienced group included five urologic experts who had completed at least 10 LPs and at least 100 other laparoscopic procedures. The less experienced group included five urologic specialists who had completed at least 20 laparoscopic procedures but had little or no experience with LP. The group with no experience included five junior residents who had completed basic laparoscopic training courses but had no experience with laparoscopic procedures. Each subject performed an “LP” procedure using this model; time to complete the procedure and the quality scores were recorded.
Statistical method
One-way analysis of variance (ANOVA) was used to detect differences in time to complete the procedure and differences in quality score. A Tukey multiple-comparisons test was used to detect differences between individual groups. P values less than 0.05 were considered significant. All calculations were performed with SPSS for Windows 13.0 software (SPSS, Inc., Chicago, IL).
Results
Those in the most experienced group completed the procedure in a mean time of 33.80 minutes. Those in the less experienced group averaged 55.20 minutes, and those in the group with no experience averaged 92.60 minutes. There was a significant difference between the groups using one-way ANOVA (P<0.001). The Tukey multiple-comparisons test showed a significant difference between the most experienced group and the less experienced group (P<0.01), between the less experienced group and the group with no experience (P<0.001), and between the most experienced group and the group with no experience (P<0.001).
With regard to quality score, one-way ANOVA also showed a significant difference between the groups (P<0.001). The Tukey multiple-comparisons test showed a significant difference between the less experienced group and the group with no experience (7.2 vs 4.0, P<0.01), and also between the most experienced group and the group with no experience (9.0 vs 4.0, P<0.001). There was, however, no significant difference between the most experienced group and the less experienced group (9.0 vs 7.2, P>0.05) (Fig. 3).

Operative time and quality scores for groups after completion of the procedure. Values are expressed as mean±standard error of the mean.
Discussion
Although it is believed that LP is rapidly moving toward replacing open surgery as the gold standard in the management of UPJO, 3,12 the great technical complexity and steep learning curve impede its extensive application. Operators have to complete several complex steps in a limited working space, including the delicate tailoring of the ureter and renal pelvis, intracorporeal suturing and knotting, prevention of kinking of the ureter, and antegrade stent placement.
Urologic residents need proper training to perfect their technique to the level of a more experienced laparoscopic surgeon before they practice LP in the operating room. Although pelvic trainers can provide the necessary basic-skills training for laparoscopic surgeons, specific training models are needed to help them grasp those difficult techniques in a shorter time. A valid simulation should provide an environment as close as possible to reality, must mimic the visual–spatial and real-time characteristics of the procedure, and must provide realistic haptic feedback. 13 Convenience and cost should also be taken into consideration. Several training models for LP had been developed, including animal models and in vitro training models.
Live animal models could provide sufficiently realistic simulation of laparoscopic conditions such as pneumoperitoneum, blood circulation, bleeding, and anatomic environment. 14 McDougall and collaborators 4 developed a porcine model in 1997. In this model, unilateral UPJO was created by ligating the UPJ over a 5F catheter for 6 weeks. The time-consuming preparation made this model both inconvenient and costly. Fu and colleagues 5 used a short segment of porcine small intestine to simulate the enlarged renal pelvis. The intestinal wall is much thicker than the renal pelvis wall, however, and intestinal mucosa is much different from urothelium. Moreover, live animal models need a complete set of equipment and instrumentation, anesthesia, and care. Ethical consideration and costs also limit the use of live animals in many countries and regions.
In vitro training models present obvious advantages with regard to availability, versatility, low cost, and absence of the need for extreme care and anesthesia. The LapED 4-in-1 model developed by Abraham and colleagues 6 provided content and face validity for both LP and vesicourethral anastomosis. The model is inexpensive and reusable, but not available in most countries and regions currently. Raza and coworkers 7 also introduced an LP model using a surgical glove. Nevertheless, synthetic models do not handle like live tissue at present.
Models composed of ex vivo animal organs share similar qualities and appearance with humans. In 2006, Ooi and associates 8 developed a simple model using chicken skin that had the advantage of low cost and ready availability. The tough chicken skin makes needle insertion very difficult, however, and tissue tear never happens even with brutal manipulation. Trainees could not comprehend the fragility of the renal pelvis and ureter, and therefore learn to manipulate tissue meticulously with this model.
Yang and coworkers 9 used a carp swim bladder and porcine ureter to construct a training model that demonstrated satisfactory fidelity and practicality; however, the LP procedure cannot be simulated completely because the ureter is separate from the “renal pelvis” at the beginning, and the swim bladder is too thin so that it is easily torn during suturing. Moreover, obtaining the fresh swim bladder and porcine ureter is not easy. A porcine bladder and urethra were used for the UPJ simulation in the training model developed by Teber and colleagues. 10 Trainees could practice the whole LP procedure with this model. The porcine bladder wall, however, is much thicker than the human renal pelvis wall, and the caliber of porcine urethra is much larger than that of the human ureter. All of these make this model less of fidelity.
In the model developed by Ramachandran and colleagues, 11 the chicken crop and esophagus share similar size, appearance, flexibility, thickness, and texture with human dilated renal pelvis and ureter. This model can be used to simulate both left and right UPJ. It allows trainees to practice the complete LP procedure, and provides sufficient surrounding tissue for preliminary dissection and mobilization, adding to the realistic nature of the simulation. 11 Practicing with this model, trainees had to manipulate tissue gently and exactly to get satisfying tailoring, perform sutures from many different angles, and handle the sutures without getting them tangled. After practicing, trainees could get acquainted with the steps of LP, enhance their manual dexterity and coordination, and improve their skill of intracorporeal suturing and knotting. It may help the trainees shorten the learning curve and improve their operative performance.
Operative time is the most common objective measure to evaluate proficiency and to differentiate between experienced and inexperienced subjects. 15,16 Some studies used volume of leakage as a single objective measure to evaluate anastomotic quality. 15 The quality of the UPJ anastomosis, however, is closely related to factors such as the distance between sutures, placement of the first stay suture without tension, and the positioning of a Double-J stent. 5 As a single factor, leakage volume is not enough to determine the anastomotic quality, so a multiple-criteria assessment was used to evaluate the anastomotic quality. 7,11
An ideal training model should have subjective validities such as face validity and content validity, and objective validities such as concurrent validity, predictive validity, and constructive validity. Construct validity is a mandatory, and one of the most valuable, assessments of a simulator before its acceptance as a competency-evaluating device. In this regard, the simulator must be able to distinguish the experienced from the inexperienced surgeon. 17
We tested this model for construct validity by examining whether operative time and quality scores were consistent with the degree of experience of the surgeons. In this study, there is a strong negative correlation between time to complete the procedure and subjects' experience. The differences in time to complete the procedure were statistically significant between the three groups.
A positive correlation between quality scores and subjects' experience was also found. A statistical difference in quality score was shown between the most experienced group and the group with no experience and between the less experienced group and the group with no experience. Although the most experienced group had a higher average quality score than that of the less experienced group (9.0 vs 7.2), we did not find a significant difference. This may be because of the small sample size of this study. The difference in operative time and quality score proved that this model was able to distinguish between subjects with different levels of experience and consequently has good construct validity.
This model is inexpensive and convenient, because a dead chicken provides all materials we need. This model, however, may be unavailable in some countries or regions, because of the restriction of chicken viscera.
The predictive validity (the degree of concordance between the outcomes on the training model and real-life performance) of this model should be assessed in future studies.
Conclusion
The chicken crop model exhibits good construct validity. It is relatively cost-effective and readily available, and can be used to reproduce the technical complexity of LP.
Footnotes
Acknowledgments
The model used in this study was described initially by Dr. Anil Ramachandran from India.
We thank Dr. Antoinette Bediako-Bowan of Korle Bu teaching hospital, Accra, Ghana, for her careful polishing of the English writing of the article.
Disclosure Statement
No competing financial interests exist.