
Abstract
Purpose:
To report the use and complication rates of percutaneous nephrolithotomy (PCNL) performed in the United States between 1998 and 2009.
Patients and Methods:
The Nationwide Inpatient Sample database was analyzed from 1998 to 2009 to identify all PCNL cases performed in adults ≥18 years old. Descriptive statistics were used for potential covariates: Demographics, comorbidities, academic/community hospital, rural/urban location, and U.S. geographic region. Common complications encoded by International Classification of Diseases-9 codes after PCNL were reported over time, and those found to be statistically significant were evaluated in the multivariate regression. Linear regression was used to analyze surgical trends. Multivariate regression was performed to identify covariates that predicted any surgical complication.
Results:
The use of PCNL among inpatients increased significantly from 15 to 27 surgeries/100,000 discharges between 1998 and 2009 (P<0.001), and this increase was seen in all geographic regions of the United States. The increase in adoption of PCNL was accompanied by an increase in complications (14% to 19%, P<0.001). Higher comorbidity (Charlson ≥3) was the strongest predictor of complications in multivariate analysis (odds ratio=2.22, P<0.001).
Conclusions:
This is the first study to demonstrate an increase in PCNL use in the United States over the last decade. While there was an increase in surgical complications during this same period, the complication rate found reported is commensurate with other international reports. PCNL is safe and use of percutaneous surgery in the United States will most likely continue to increase.
Introduction
To determine if the use of PCNL was increasing over time nationally, we analyzed the Nationwide Inpatient Sample (NIS). We hypothesized that the likelihood of undergoing PCNL varied as a function of demographics, regionalization, and comorbidity. We also hypothesized that certain metrics, particularly complications, would decrease over time, contributing to the adoption of PCNL.
Patients and Methods
The NIS database is part of the Healthcare Cost and Utilization Project, sponsored by the Agency for Healthcare Research and Quality. The NIS is the largest all-payer inpatient care database in the United States, containing data on more than seven million hospital stays annually from approximately 1000 hospitals, constituting a 20% stratified sample of all U.S. hospitals. All data were weighted using discharge level values, based on the relative proportion of the total U.S. hospital patient population accounted for by that record, to produce 100% national estimates. The NIS includes charge information for all patients, regardless of payer, including patients covered by Medicare, Medicaid, private insurance, and the uninsured. Inpatient stay records include clinical, hospital, and resource use information typically available from discharge abstracts. Discharges from 1998 through 2009 were included in the analysis.
We identified adult patients (≥18 years old) with International Classification of Diseases (ICD)-9 procedural codes for PCNL (55.04 or 55.03/55.21) from 1998 through 2009. Patients undergoing a PCNL during their hospital stay, including those patients needing a second-look PCNL, were all captured using these ICD-9 codes and included in the analysis; patients who needed a subsequent SWL or URS during their inpatient hospital stay were excluded. Patient age, race, sex, treatment year, geographic region of treatment (Northeast, South, Midwest, and West), Charlson Comorbidity Index (CCI) score, comorbidities (hypertension [HTN], diabetes mellitus [DM], obesity), urban/rural location, teaching/community, and length of stay were abstracted.
A list of common complications was compiled. The composite of all complications—called “any complication”—was created. Multivariate analysis using binary logistic regression was performed to predict “any complication”; variables that were P<0.2 in univariate testing, or were determined to be clinically relevant were included in model development, with the final model including only those variables that retained significance (at P<0.05 level). Collinearity precluded use of certain variables (HTN, DM, obesity with CCI score). Chi-square, analysis of variance, and Student t tests (using Bonferroni correction for intergroup comparisons) were performed depending on whether the variable was continuous or categorical. Prevalence over time was examined using simple linear regression to produce β coefficients (average change over time). We determined which covariates increased over time using the chi-square test. All testing was two-tailed, with probability of type I error alpha=0.05, a priori. SPSS version 17.0 software (SPSS, Inc., Chicago, IL) was used for all statistical analyses.
Results
Approximately 83,676 hospital discharges (weighted value) were analyzed from 1998 through 2009. The use of PCNL increased significantly, from 15 to 27 surgeries/100,000 discharges, P<0.001 (Fig. 1). Although use of PCNL significantly increased in all regions of the country, the adoption increased most in the Midwest (β=136 surgeries/year) and least in the Northeast (β=45/year) (Fig. 2). More than 86% of patients undergoing PCNL had renal calculi, while 14% had ureteral calculi. Approximately 62.1% of all PCNL cases were performed at academic teaching hospitals (Table 1).
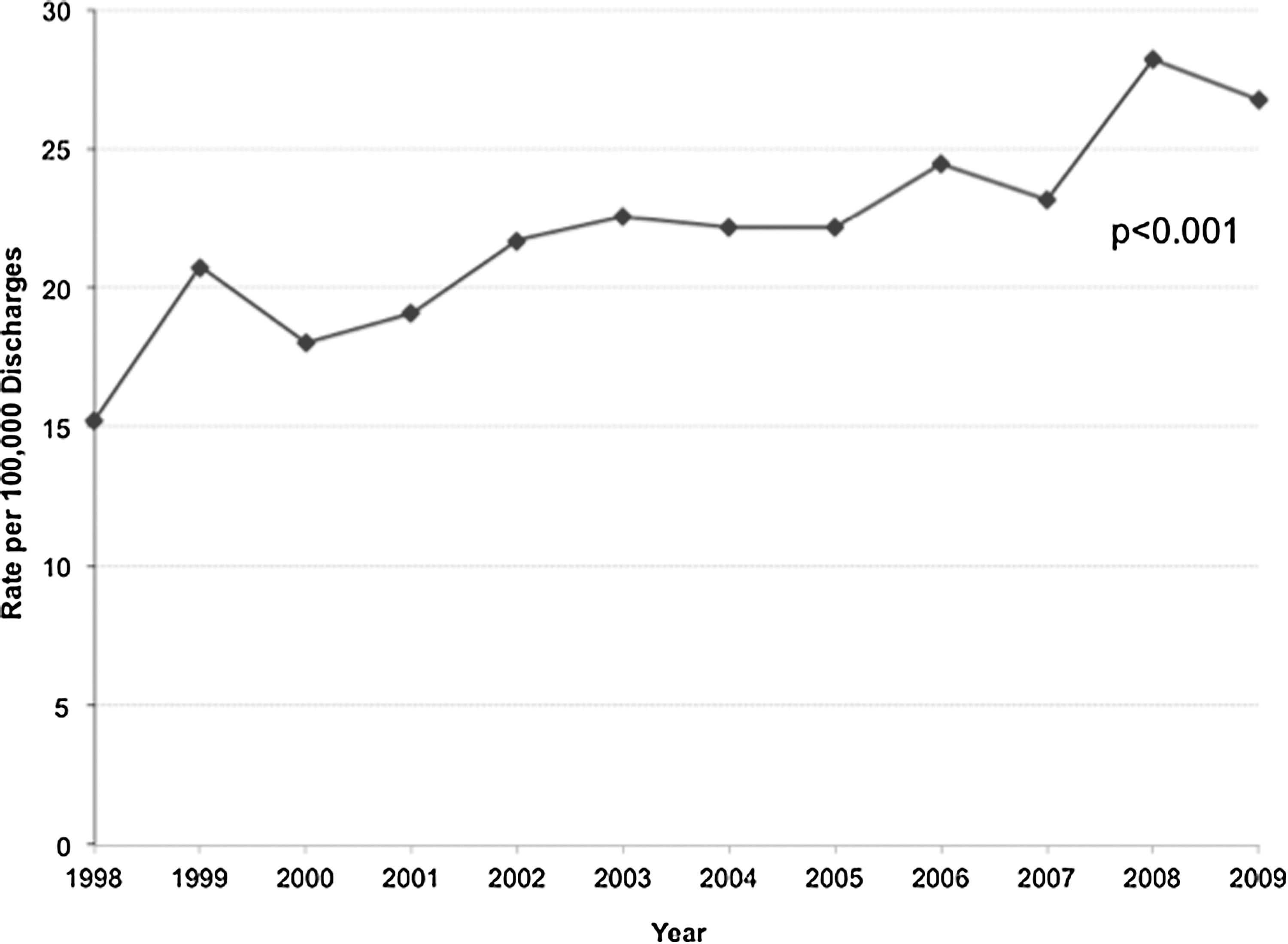
Inpatient percutaneous nephrolithotomies (per 100,000 discharges) over time.
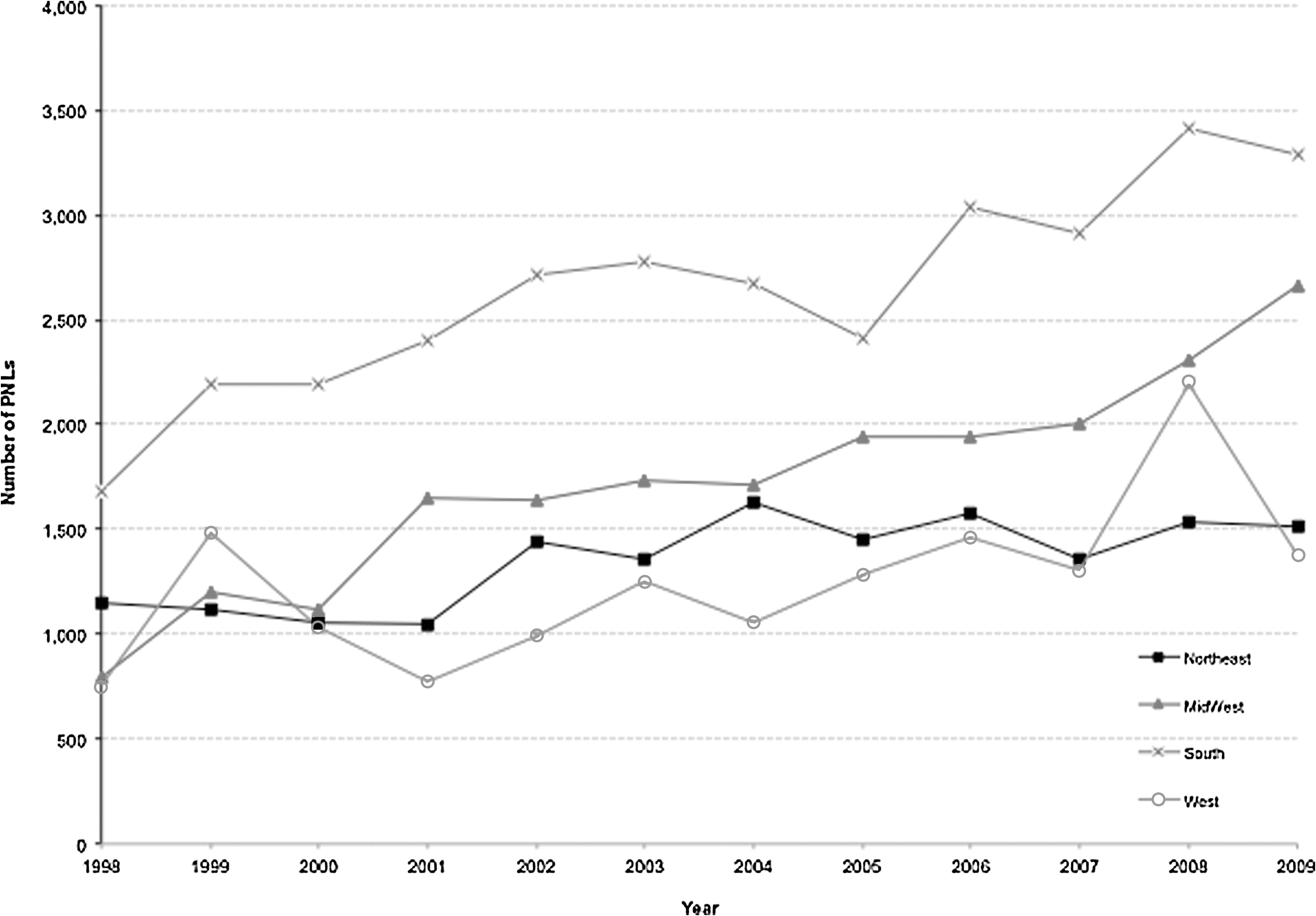
Regional use of percutaneous nephrolithotomy (PNL) over time. squares: Northeast; triangles: Midwest; Xs: South; circles: West.
PCNL=percutaneous nephrolithotomy; SE=standard error; IQR=interquartile range.
The mean age of patients undergoing PCNL was 53 years, and 51.2% of patients were female (Table 1). HTN, DM, and obesity were observed in 38%, 18%, and 9% of the entire cohort, and the proportion of patients with DM, HTN, and obesity undergoing PCNL increased significantly over time, P<0.001. The obesity rates varied by sex with women nearly twice as likely to be obese than men (11.1% female vs 6.9% males, P<0.001). Approximately 4.1% of patients who underwent PCNL had a CCI score of ≥3. Similarly, the proportion of patients with CCI ≥3 undergoing PCNL also increased significantly over time, P=0.048. The median hospital length of stay was 3 days, and length of stay significantly decreased over time from 3 to 2 days, P<0.001.
In 13,020 (15.6%) patients, “any complication” was seen, and the three most common reported complications were urosepsis/urinary tract infection (8.4%), blood transfusions (4.4%), and sepsis (2.4%) (Table 2). The overall complication rate significantly increased from 14.1% to 18.5% between 1998 and 2009 (Fig. 3); specifically, rates of pneumothorax (P=0.031), transfusion (P<0.001) and sepsis (P<0.001) increased over time. Because complications increased rather than decreased as we originally hypothesized, we performed a subanalysis to better understand which demographic and disease factors may account for rising complications. Multivariate analysis demonstrated that patients with CCI ≥3 were 2.22 times more likely to have “any complication” (Table 3). Females were at increased risk of having “any complication.” PCNLs performed in the South or West and urban centers were associated with an increased chance of complication. The complication rates in rural (720/4853, 14.8%) and urban (12,227/78,568, 15.6%) hospitals as well as teaching (7,895/51,803, 15.2%) and nonteaching (5,052/31,617, 16%) hospitals were compared and no differences were observed, P=0.54 and P=0.33, respectively.
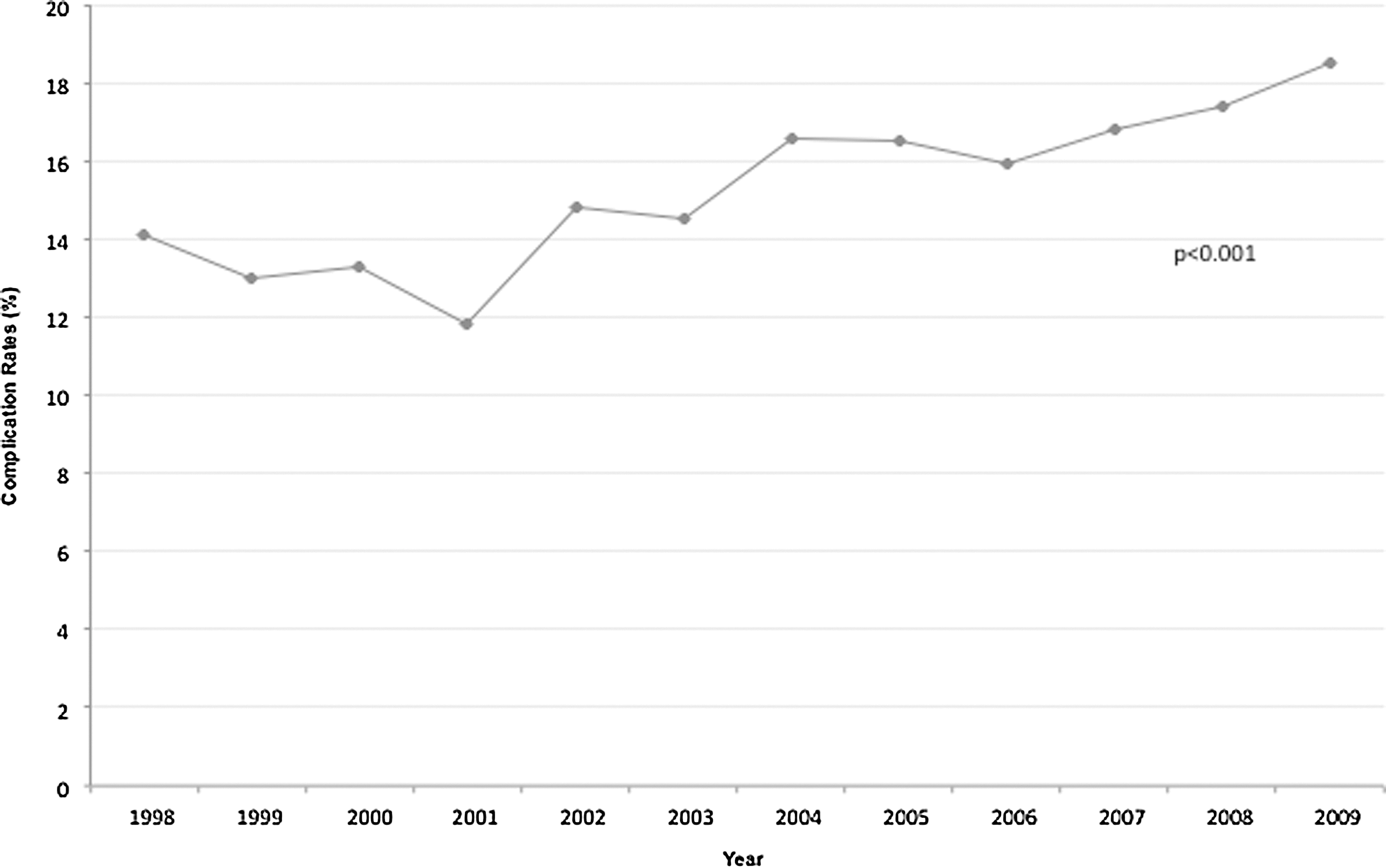
Complication rates over time.
Outcome=any complication (1998–2009).
OR=odds ratio; CI=confidence interval.
Discussion
Recent work by the Clinical Research Office of the Endourological Society (CROES) has confirmed that PCNL use is now widespread through the industrialized world. This project by CROES revealed that more than 5800 percutaneous procedures have been performed between November 2007 and December 2009. 5 In fact, these numbers are arguably very conservative, because the database only abstracts a few academic centers in the United States and academic and community centers associated with the Endourological Society. Including data from all academic and community hospitals in these countries would produce a much higher prevalence of percutaneous surgery. By using the NIS, we were able to estimate national numbers for all inpatient percutaneous procedures performed at both academic and community hospitals. Our analysis confirmed that the global trend of increased use of PCNL also occurred in the United States between 1998 and 2009.
Moreover, our data illustrate the use of PCNL has almost doubled during this period. This analysis contradicts previous reports using Medicare datasets from a slightly earlier period (1992–1998), which demonstrated stable use of PCNL. 6 Medicare datasets represent a selection bias because they are unfortunately limited to older patients and those selected persons eligible for Medicare coverage. The increased adoption of PCNL is also demonstrated across all regions of the United States, confirming a uniform, nationwide trend. Why the adoption is more pronounced in the Midwest and South compared with the West and Northeast is unclear. Increased prevalence of nephrolithiasis in these areas could potentially explain the regional trends. Larger stone burden as well as surgeon and patient preferences are potential explanations, but this evidence is beyond the scope of NIS. Financial incentives also may play a role as has been surmised for other stone procedures in a recent report on outpatient surgery in Florida 7 and regionalization of complex procedures to tertiary centers may also contribute to preferential choice of certain procedures. 8
We had hypothesized that the adoption of this new technology might be because of improved outcomes such as declining complications. The data instead showed that complications significantly increased from 14.1% to 18.5% during this period. Although our prevalence of complications is consistent with a recent systematic review reporting a 23.3% complication rate for PCNL, 9 we surmise several plausible explanations for this increase in complications.
We know that according to several studies, complications in low-volume centers are greater than high-volume centers. 10 –12 Therefore, the diffusion of PCNL during our 10-year period was possibly accompanied by a large proportion of complications at low-volume centers attempting to adopt the technology. The CROES data also illustrated that severity of complications was initially higher until 100 to 150 cases were achieved. 10 In fact, severity of complication had a bimodal distribution with severity increasing after 150 cases. The data also demonstrated that probability of complication was proportional to stone burden. Taken together, it is conceivable that as centers became more comfortable with PCNL, stone burden and case volume increased—having an overall increase in complication effect. Indeed it can be inferred that stone burden most likely increased given the significant rise in complications typical of larger stones, such as transfusions, sepsis, and pneumothorax. 13
Comorbidity is an intuitive covariate of PCNL complications. Tefekli and associates 14 demonstrated that complications were 2.7 times more common in patients with DM and HTN. Patients with metabolic syndrome also needed more ancillary treatments after PCNL. Similarly, our study demonstrated that comorbidity (CCI ≥3) increased the risk of complications by 2.2. Increased prevalence of DM and HTN in patients undergoing percutaneous surgery over time in our cohort may thus account for the increased rate of complications reported from 1998 to 2009. The rising prevalence of metabolic syndrome (DM, HTN, obesity, hyperlipidemia) in the United States over the last decade 15 and the association between metabolic syndrome and nephrolithiasis 16 –18 supports our supposition that these cocovariates may have contributed to the rise in PCNL complications.
Limitations of the NIS are inherent to this dataset: It relies on accurate physician coding, and it does not provide clinical data (eg, stone size) that would possibly provide insight into procedure choice. Another limitation of the NIS is that complications are not classified according to the Clavien-Dindo system, 19 and thus direct comparisons of severity of complications with other large PCNL case series are not possible. There is a trend toward percutaneous surgery in an outpatient setting, and we admittedly are missing this data; however, this surgery is still predominantly an inpatient procedure. Notwithstanding the above limitations, this study is important in that it quantitatively confirms that percutaneous stone surgery has increased over the last decade in the United States.
Conclusions
In the largest U.S. NIS, PCNL use has increased by nearly twofold. Although there was a concomitant increase in complications, this perhaps is a natural phenomenon observed during diffusion of an established surgical technique to patients with more comorbidities at hospitals less experienced in performing this procedure. The proportion of complications is consistent with worldwide reports and supports the continued use of percutaneous surgery. Increased use will likely witness a plateau in complications, further justifying the advantages of percutaneous surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.