
Abstract
Purpose:
We compared the safety and efficacy of diode laser enucleation of the prostate (DiLEP) with plasmakinetic enucleation and resection of the prostate (PKERP).
Patients and Methods:
A total of 80 patients with bladder outflow obstruction from benign prostatic hyperplasia (BPH) were randomly assigned to either DiLEP or PKERP prospectively. All patients were assessed preoperatively and followed up at 3, 6, and 12 months postoperatively. Baseline characteristics of the patients, perioperative data, and postoperative outcomes were compared. The operative data and perioperative and postoperative complications were also recorded.
Results:
The preoperative data were comparable between the two groups. The DiLEP group had significantly shorter operative time, postoperative irrigation, time and catheterization time than the PKERP group (P=0.000, P=0.000 and P=0.000). The drop in hemoglobin level was statistically significantly less in the DiLEP group (P=0.002). There were no statistical differences in complications between the two groups except irritative symptoms (P=0.018). At the 3, 6, and 12-month follow-up, no statistically significant differences were observed between the two groups in International Prostate Symptom Score, maximum flow rate, quality of life, postvoid residual, prostate volume, and prostate-specific antigen level (P>0.05).
Conclusions:
The efficacy of DiLEP and PKERP were similar for relieving obstruction and low urinary tract symptoms. DiLEP provides less risk of hemorrhage, reduced bladder irrigation, and catheter times. The downward morcellation technique is more efficient than the resection technique. Future well designed randomized trials with extended follow-up and larger sample sizes may be needed to better verify the advantage of DiLEP in treating patients with symptomatic BPH.
Introduction
Laser enucleation of the prostate for treating patients with BPH was first described in 1998. 3 Then, a variety of lasers, including holmium laser, potassium titanylphosphate (KTP) laser, thulium laser, and diode laser were used for treating patients with BPH. 4 –10 The diode laser is absorbed by both water and hemoglobin, and ex vivo and in vivo investigations showed its high vaporization capacities and excellent coagulation properties. 10 The high-power diode laser provided significant improvements in the International Prostate Symptom Score (IPSS) and maximal flow rate (Qmax) with low morbidity. 9 Eraser laser, a 1318-nm diode laser, provided excellent safety and efficacy for treating patients with BPH. 11,12
Transurethral enucleation of the prostate (TUEP) is a novel alternative technique that can remove prostatic adenoma anatomically and also may offer comparable results to open surgery by minimally invasive endoscopic surgery. TUEP using a plasmakinetic (PK) device, so-called plasmakinetic enucleation of the prostate (PKEP), was first described in 2006. 13 A recent study showed PKEP represented a promising endoscopic approach in patients with large BPH, characterized by good surgical efficiency and similar BPH tissue removal capabilities compared with standard transvesical prostatectomy. 14
We have used the PKEP technique to relieve benign prostatic obstruction (BPO) for more than 10 years. The difference in the PKEP procedure in this study from others is that the adenoma was removed by loop electrode resection but not the morcellator. We defined this procedure as transurethral enucleation and resection of prostate (PKERP). A retrospective report of 1100 patients who were treated by PKERP in our center with mean 4.3-year follow-up has demonstrated its safety and effectiveness. 15
Based on the advantage of TUEP and the high vaporization capacities and excellent coagulation properties of the diode laser, we combined the diode laser with TUEP and morcellation in comparison with bipolar transurethral enucleation and resection of the prostate (TUERP) in the treatment of patients with BPH to evaluate the efficacy and safety of DiLEP.
Patients and Methods
Patients
From July 2011 to November 2011 in our department, patients with lower urinary tract symptoms from BPH who had the indication for endosurgical treatment were invited to participate in the study. A total of 80 patients were randomly assigned to either DiLEP or PKERP. Inclusion criteria were age ≥50 years, IPSS ≥7, and Qmax ≤15 mL/s. Exclusion criteria included any patient with neurogenic bladder, history of prostatic or urethral surgery and prostate cancer. This study was approved by our hospital ethics committee. Informed consent of all patients was obtained.
Assessment parameters
All patients received a digital rectal examination, urine analysis, and test for prostate-specific antigen (PSA) levels. The size of the prostate was measured with transrectal ultrasonography (TRUS). The functional assessments parameters included postvoid residual (PVR) urine volume, Qmax, IPSS, and quality of life (QoL) score. If prostate cancer was suspected, TRUS-guided biopsy was performed. Perioperative outcome measures included operative time, changes in serum sodium and hemoglobin levels, the need for blood transfusion, TURS, postoperative irrigation, catheterization time, and hospital stay. All patients were followed up at 3, 6, and 12 months postoperatively. IPSS, Qmax, QoL, and PVR were obtained at each follow-up. Perioperative data and postoperative outcome were compared. All complications were recorded. A test for PSA level and TRUS were performed at 6 months postoperatively.
Instruments and surgical procedures
All surgical procedures were performed by surgeons who were fully trained in DiLEP and PKERP. Major equipment for surgery: Gyrus plasma kinetic generator, 250 W Urobeam 980 nm diode semiconductor laser, Storz (Tuttlingen, Germany) 30-degree resectoscope, Storz laser operator, Storz wide-angle percutaneous nephroscope, morcellator system (including no.23030011, no.8564.121, no.22080010, no8970.001, Richard Wolf, Knittlingen, Germany). For surgery, all patients were in the lithotomy position and received epidural anesthesia.
The procedure of TUERP
The PK system uses 160 W for cutting and 80 W for coagulation. Physiologic saline served as irrigation fluid. The 27F resectoscope was placed in the bladder under video-assisted endosurgical system guidance. The incision was begun close to the verumontanum from the 5 to the 7 o'clock positions, and the urethral mucosa was incised deep to the level of the surgical capsule. The distal midlobe and mucosa were dissected in retrograde fashion toward the bladder neck by the resectoscope tip combined with a loop. The loop was used to cut off the adhesive fibers between the lobe and the surgical capsule and coagulate denuded supply vessels and hemorrhage spots on the capsule surface. This procedure progressed toward the bladder neck until the circular fiber of the bladder neck was identified. The bilateral lobes were enucleated similar to the midlobe.
After most of the blood supply to the lobes was blocked, the adenoma was resected rapidly and thoroughly by the loop electrode from the 12 to the 6 o'clock positions without serious hemorrhage. When resection was completed, all adenoma fragments in bladder were rinsed out by Ellic washer. After enucleation and extraction of all adenoma fragments, a standard 22F three-way catheter was inserted and connected to straight drainage. 15
The procedure of DiLEP
The power of the diode laser system was set at 120 W. The procedure of DiLEP was similar to PKERP. The differences were that the denuded supply vessels and hemorrhage spots were coagulated by the 980 nm diode laser. The whole adenoma was enucleated and pushed into the bladder. The adenoma was removed by the morcellator system. Morcellation using an inverse (downward) technique introduced by Hwang and associates 16 was used to improve the safety of the morcellation procedure. The blade is hung upside down such that it is directed toward the base of the bladder. By positioning a morcellator on top of prostatic tissues, the tissues can be held and evacuated from above by suction. The surgical procedure is shown in Figure 1.
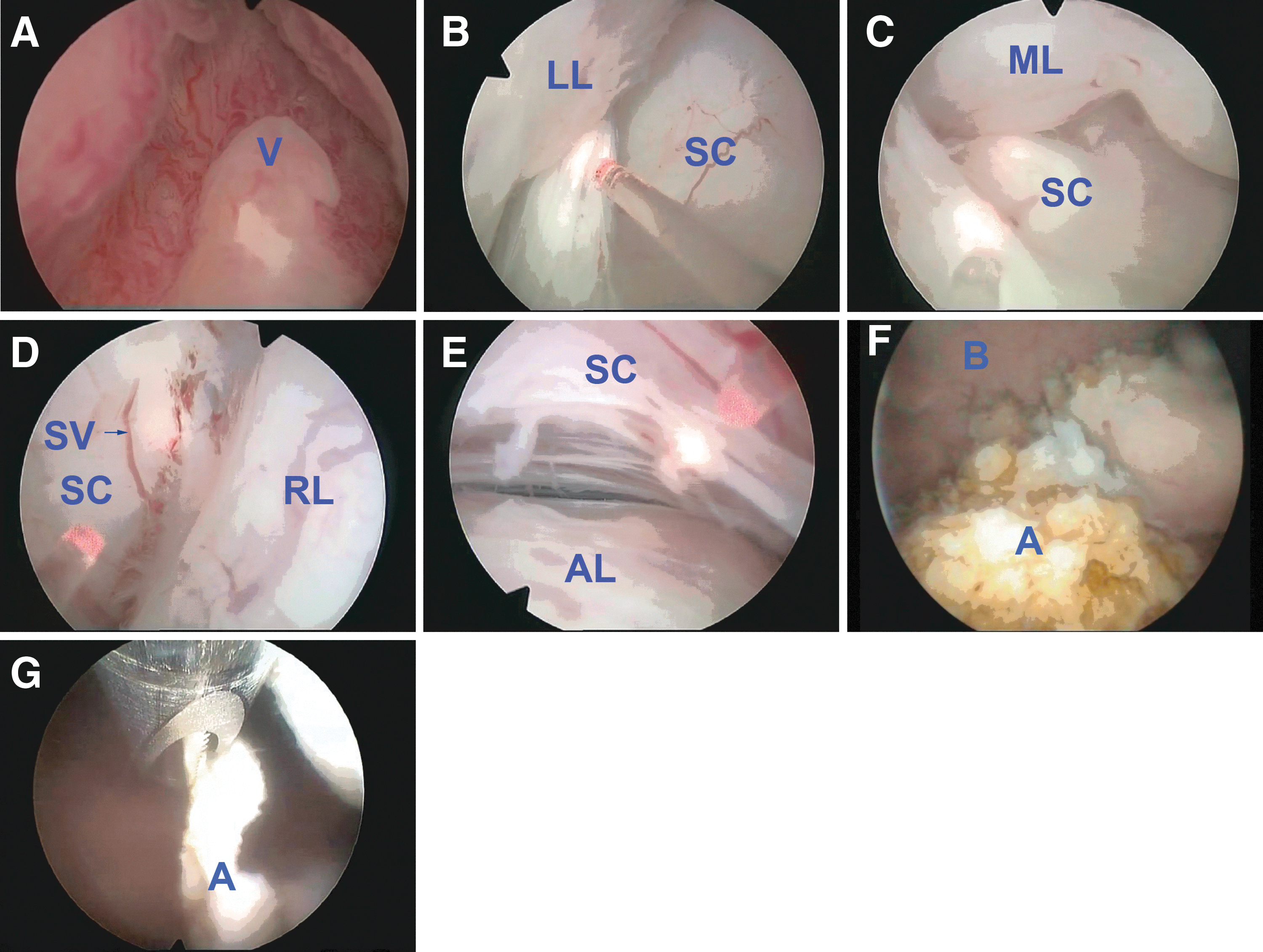
Diode laser enucleation of the prostate (DiLEP) operative steps:
Statistical analysis
The sample size was calculated to be at least 33 patients in each group with α=0.05, β=0.20 and a desired statistical power level of 80%. Considering our research expenses and study period, 40 patients were set in each arm. All measurement data were presented as mean±standard deviation. Statistical analysis was conducted using SPSS 18.0 Statistical Software (IBM, Armonk, NY) performing one-way analysis of variance and chi-square test with the significance level at P<0.05.
Results
The baseline characteristics of the DiLEP vs PKERP groups were not significantly different in any aspect (P>0.05). Hyponatremia was not observed in both groups, and there was no statistically significant difference in serum sodium decrease between the two groups (P=0.000). The hemoglobin drop in the DiLEP group was significantly lower than in the PKERP group (P=0.002). The enucleating duration was similar between the two groups (P=0.117). The morcellation duration in the DiLEP group, however, was significantly shorter than the resection duration in the PKERP group (P=0.000), and the total surgical duration in the DiLEP group was significantly shorter than in the PKERP group (P=0.000). There was no significant difference in resected tissue weight and percentage of resected tissue between the groups (P=0.493 and P=0.127). There was no statistically significant difference in hospitalization time between the two groups (P=0.103). The postoperative irrigation time and catheterization time in the DiLEP group was significantly shorter than inthe PKERP group (P=0.000). Data are shown in Table 1.
Different methods for removal of the adenoma were used in the two groups. A morcellator was used in the DiLEP group, but a loop electrode was used in the PKERP group.
Percentage of resected tissue: Resected weight/preoperative prostate volume.
DiLEP=diode laser enucleation of the prostate; PKERP=plasmakinetic enucleation and resection of the prostate.
All 80 patients in the two groups completed the follow-up at 3, 6, and 12 months after operation. There was no statistically significant difference in IPSS, QoL, Qmax, PVR, prostate volume, and PSA level between the two groups (P>0.05). The follow-up data are shown in Table 2.
IPSS=International Prostate Symptom Score; SD=standard deviation; DiLEP=diode laser enucleation of the prostate; PKERP=plasmakinetic enucleation and resection of the prostate; QoL=quality of life; Qmax=maximum flow rate; PVR=postvoid residual; PV=prostate volume; PSA=prostate-specific antigen.
Two (5%) cases of intraoperative capsule perforation occurred in the DiLEP group and in one (2.5%) patient in the PKERP group. The difference was not statistically significant (P=0.556). No blood transfusion was needed in either group. Death, TURS bladder injury and rectal injury did not occurred in either group. Three (7.5%) patients and four (10%) patients had transient incontinence in the DiLEP group and PKERP group, respectively. The difference was not statistically significant (P=0.692). Urinary control in seven patients with transient incontinence was recovered at 3-month follow-up. Five (12.5%) patients and 14 (35%) patients had postoperative bladder irritation in the DiLEP group and PKERP group, respectively. The incidence of bladder irritation in DiLEP group was statistically significantly less than in the PKERP group (P=0.018). None of the patients in the two groups had urinary retention, long-term urinary incontinence, urethral stricture, and secondary hemorrhage. The complications in the two groups are shown in Table 3.
DiLEP=diode laser enucleation of the prostate; PKERP=plasmakinetic enucleation and resection of the prostate; TURS=transurethral resection syndrome.
Discussion
BPH is a common medical condition in middle-aged and elderly men. TURP remains the gold standard surgical treatment for patients with symptomatic BPH. Although the complications of contemporary TURP continuously declined compared with previous classic studies, traditional TURP is still associated with significant morbidity, especially bleeding. 17 Urologists therefore make efforts to look for new endoscopic treatments for patients with symptomatic BPH.
Combined with the PK system, TUEP is an endoscopic alternative for the treatment of symptomatic BPH for men even for the cases with prostate volume larger than 80 ml. 14 As the high vaporization capacities and excellent coagulation properties of lasers were verified, several lasers including holmium laser, KTP laser, thulium, and diode laser were adapted in TUEP. Krambeck and colleagues 4 reported on more than 1000 patients who underwent holmium laser enucleation of the prostate (HoLEP) during 10 years and in whom excellent long-term results were achieved. 4 TUEP using a thulium laser or KTP laser is a safe and efficacious procedure for the treatment of patients with symptomatic BPH. 5 –8
Urobeam 980 nm diode lasers, selectively absorbed by water and hemoglobin in tissues, was confirmed effective in hemostasis by animal experiments, even more effective than KTP laser, holmium laser, and standard monopolar resectoscope. 18,19 The 980 nm and 1318-nm diode laser provided excellent safety and efficacy for treating patients with BPH. 9 –12 The advances of DiLEP over PKERP, however, the standard method for treating patients with BPO in our center, still needed to be confirmed by prospective randomized controlled trials. The present study compared the efficacy and safety of DiLEP and PKERP for BPO.
This study showed that no patients needed blood transfusions in both groups. The drop in hemoglobin in the DiLEP group, however, was significantly less than in the PKERP group. Diode lasers were selectively absorbed by both water and hemoglobin, resulting in excellent hemostasis. 20 This study using diode laser to treat patients with BPH showed similar results with other studies on hemostatis. 9 –12
TURS was another severe complication of traditional TURP, but no TURS was observed in both groups. Because physiologic saline was applied as the irrigation fluid, DiLEP and PKERP almost have no risk of TURS. 21,22 Another reason was that the relatively short operative time because of the relatively small prostates in this study reduced the absorption of irrigation fluid into the circulation.
Transient stress urinary incontinence is a common complication of endosurgical prostate enucleation, including laser enucleation and PKEP. The prevalence of transient stress urinary incontinence after HoLEP has been reported to be 1% to 44%. 16,23 The incontinence frequency of thulium:yttrium-aluminum-garnet vapoenucleation of the prostate (ThuVEP) and photoselective vaporization of the prostate (PVP) was reported to be 2.5% to 25% and 0% to 2% in recent studies. 6,24 –27
This study demonstrated that stress urinary incontinence frequency in DiLEP was comparable to that of PKERP. The stress urinary incontinence rate in the DiLEP group and PKERP group was 7.5% and 10%, respectively, similar to HoLEP and ThuVEP. 6,16,24,25 Stress urinary incontinence disappeared at the 3-month follow-up. The transient stress urinary incontinence in this study might be caused by blunt trauma of the external sphincter from a too large swinging amplitude of the sheath or compressive atrophy of the external sphincter, but not the thermal injury of the external sphincter. Therefore, stress urinary incontinence can be obviously relieved after a period of pelvic floor muscle training. Efforts to reduce injuries on the external sphincter during enucleation, however, are also to be made. 28
Laser enucleation has maximal association with irritative symptoms. 29 The irritative symptoms incidence of HoLEP and ThuVEP was 31.2% and 4.34% to 22.5%. 6,24,25,29 This study showed the incidence of irritative symptoms in the DiLEP group is 12.5%, significantly less than the 35% in the PKERP group. This can be explained by the fact that the prostatic adenoma was enucleated chiefly by mechanical force in both the DiLEP group and the PKERP group. In contrast to other laser enucleation of the prostate, less coagulated and necrotic tissues in the DiLEP group have to slough off postoperatively because of less heat injury in the DiLEP group on the wound surface than the PKERP group in this study. 29
Accordingly, the curative effect of DiLEP and PKERP is similar. There was no statistically significant difference between the two groups in Qmax, QoL score, IPSS, and PVR at 3-, 6-, and 12-month follow-up postoperatively. It demonstrates that the curative effect of DiLEP is at least equivalent to PKERP in the early postoperative period. The question is whether the patients who improved from baseline to early follow-up will sustain these improvements at later follow-up. Long-term follow-up data, therefore, should be collected to compare DiLEP with PKERP in the future.
Although the application of the PK system in TURP does not improve the resection efficiency, PK TURP shows superiority over monopolar TURP because of its fewer complications. 30 Comparing of studies showed higher efficiency in bipolar TURP than laser enucleation including eraser laser enucleation of the prostate and HoLEP. 11,31 The result of this study, however, was opposite in that DiLEP was more efficient than PKERP. The key point that is different from other centers is that the surgical procedure enucleating the adenoma using the sheath is similar between two groups in this study. The energy for the enucleation procedure in our center is just used for hemostasis. Because the prostate size and the enucleating procedure between the two groups are similar, the enucleating time between the two groups was similar. The longer operative time was contributed by the longer time needed for resection of the adenoma than morcellation of the adenoma. The efficiency of the inverse morcellation technique introduced by Hwang and coworkers 16 was up to 4.06 g/min16 and this study showed similar morcellation efficiency. The combination of the inverse morcellation technique and our endoscopic enucleation technique makes the DiLEP technique more efficient.
Accordingly, the percentage of resected tissue was similar between the DiLEP group and PKERP group in this study. The percentage of resected tissue in this study is similar to the recent study of HoLEP, ThuVEP, and PKEP. 6,14,24,25,31 Because the surgical procedure enucleating the adenoma using the sheath in this study was similar to open prostatectomy, the adenoma was sure to be anatomically enucleated completely. That will ensure the relief of bladder outlet obstruction from BPH.
These results have limitations because of the small sample size and short follow-up. These results, therefore, should be confirmed with larger prospective randomized trials comparing DiLEP with HoLEP, ThuVEP, PVP, or open prostatectomy with longer follow-up.
Conclusions
PKERP and DiLEP were shown to be effective and safe treatments for prostates of all sizes. DiLEP provides less risk of hemorrhage, reduced bladder irrigation, and catheter times. The inverse (downward) morcellation technique is more efficient than the resection technique. Future well-designed randomized trials with extended follow-up and larger sample sizes may be needed to better verify the advantage of DiLEP in treating patients with symptomatic BPH.
Footnotes
Acknowledgment
This work was supported by China Postdoctoral Science Foundation funded project (No. 2012M511830 for Bingkun Li).
Disclosure Statement
No competing financial interests exist.