
Abstract
Background and Purpose:
Renal mass protocol CT (RMP-CT) using multiphase abdomen and pelvis CT imaging is the mainstay for diagnosis, characterization, and follow-up for renal masses; however, it is associated with ionizing radiation to the patient. We sought to quantify the effective dose associated with RMP-CT and to determine how patient factors affect radiation exposure.
Material and Methods:
We retrospectively reviewed the records of 247 patients undergoing management of a small renal mass (cT1a) between 2005 and 2011 at our institution. Body mass index (BMI) was categorized as normal weight, overweight, obese, and morbidly obese (≤25, 25.1–30, 30.1–35 and >35, respectively). Effective dose of RMP-CT was calculated through the dose-length-product multiplied by a factor coefficient (0.015). Effective doses in milliSieverts (mSv) were correlated to patient characteristics.
Results:
Patients' median age was 61 years, and median BMI was 28.7 kg/m2; 72% were Caucasian and 56% were male. Median effective dose was 26.1 mSv (interquartile range 20.6–35.3). When stratified by BMI, the median effective doses were 18.9, 25.2, 27.7, and 36.2mSv for normal weight, overweight, obese, and morbidly obese patients, respectively. On multivariable analyses, BMI and male sex were significantly associated with increased radiation dose.
Conclusions:
In this series, the median effective dose for RMP-CT was 26.1 mSv. Obesity was independently associated with markedly increased radiation exposure, with morbidly obese patients being exposed to almost twice the amount of radiation compared with normal weight persons. These findings should be considered when devising management strategies in patients with a renal mass and strategies should be developed to reduce medical ionizing radiation exposure.
Introduction
Currently, medical imaging represents the dominant source of ionizing radiation exposure in the Western population, accounting for 3.0 milliSieverts (mSv)/year per capita, of a total effective dose of 5.6 mSv/year. 3 Compared with 3.3 million studies in 1980 to 1982, in 2006 there were 67 million CT studies performed, representing a per capita dose of 1.47 mSv/year from CT studies alone. 3 Importantly, abdomen-pelvis CT accounts for 31% of all CT scans performed and is responsible for 48% of the cumulative radiation exposure from CT scans. 3 Because renal mass management relies heavily on imaging modalities and specifically CT, an assessment of the associated radiation exposure is warranted. A previous study found a median effective dose of 31 mSv for abdomen-pelvis multiphase CT and reported a wide variation in the effective dose. 4 The factors responsible for this ample range are unknown.
The increasing prevalence of obesity in the United States warrants continuous assessment of radiation exposure in the changing landscape of patient population. Although effective doses are expected to increase in larger patients, the impact of body habitus on radiation exposure in patients with renal masses has not been investigated.
In this study, we assess the effective radiation doses incurred by patients from RMP-CT and evaluate the impact of patient characteristics on radiation exposure in this contemporary cohort.
Materials and Methods
Patients
After approval from the Institutional Review Board, the records of patients undergoing nephron-sparing surgery for a small renal mass (≤4 cm) at our institution between 2005 and 2011 were retrospectively reviewed. Demographic and clinical characteristics—body habitus (height, weight, body mass index [BMI]), sex, race, mode of presentation (incidental or symptomatic), and renal mass size—were collected. BMI was categorized as normal weight (≤25), overweight (25.1–30), obese (30.1–35), and morbidly obese (>35). The imaging studies were reviewed to identify RMP-CT performed for diagnosis and/or characterization of the renal lesion, and calculated the associated effective doses of radiation exposure. Records missing dose length product (DLP) values and those lacking demographic information were excluded from the present analysis.
RMP-CT
All RMP-CT imaging studies were performed on 16 (LightSpeed 16, General Electric Healthcare, Milwaukee WI) or 64-slice (LightSpeed Discovery 750 HD and LightSpeed VCT, General Electric Healthcare) multidetector scanners using helical acquisition. RMP-CT studies were performed at a default voltage of 120 kV. Automatic exposure control software (AutomA, General Electric Healthcare) was used to determine tube current for each patient to minimize dose while optimizing image quality. The algorithm analyzes a scout image obtained immediately before the scan and calculates the optimal current based on a preselected noise index setting. The default scanner pitch was 3.0.
Images were acquired at slice thickness of 0.625 or 1.25 mm, depending on the specific scanner, and reconstructed to a slice thickness of 5 mm for review at the workstation. Before contrast administration, noncontrast images were obtained from the superior margin of the kidneys to the pubic symphysis. Iopamidol (Isovue 300, 150 mL) was administered intravenously at a rate of 3 mL/sec. Subsequently, two sets of contrast-enhanced images were acquired with the first set from diaphragm to the inferior margin of the kidneys, and the second set of images acquired from the top of the kidneys to the pubic symphysis. For patients presenting for first-time evaluation of a renal mass, contrast-enhanced imaging was performed in the nephrographic phase followed by excretory phase, whereas for patients with known renal RCC, contrast-enhanced imaging included the arterial phase followed by portal venous phase to optimize detection of potential RCC metastases. Therefore, for each RMP-CT scan, three sets of images were obtained for each patient.
Effective doses in mSv for CT imaging studies were calculated by obtaining the product of the DLP (CT dose index multiplied by the scan length), routinely stored in our picture archiving and communication system for CT studies, and the reference standard conversion coefficient (0.015 for abdomen and pelvis studies 5 –8 ).
Statistical analyses
Data are presented as median (interquartile range [IQR] or number [percent]) unless otherwise specified. Associations between effective doses and patient characteristics were evaluated using univariable correlations and regression models. Multivariable models including age, sex, body habitus, as well as renal mass size were constructed to determine factors associated with effective doses of RMP-CT.
Statistical analyses were performed using the R software v2.13 (the R Foundation for Statistical Computing, Vienna, Austria). All tests were two-sided and P values <0.05 were considered statistically significant.
Results
Overall, 247 patients were included in this study. Median patient age was 61 (51–68) years, median BMI was 28.7 (26.1–33.7), 139 (56%) were men, and 178 (72%) were Caucasian. Detailed patient characteristics are presented in Table 1. Median effective dose from RMP-CT was 26.1 mSv.
IQR=interquartile range; BMI=body mass index; DLP=dose length product.
Effective doses were then correlated to demographic and clinical characteristics with univariable analyses (Table 2). Both height and weight were associated with effective doses on univariable analyses; consequently every unit increase in BMI increased the effective dose by 0.53 mSv. Patient age was inversely associated with the effective dose, whereby every year of age resulted in a 0.2 mSv decrease in radiation exposure (P=0.002). The median effective doses were 18.9 mSv in normal weight, 25.2 mSv in overweight, 27.7 mSv in obese, and 36.2 mSv in morbidly obese patients (P<0.001), Figure 1. Of note, men received higher effective doses compared with women (26.8 vs 24.5 mSv, P=0.023), Figure 2.
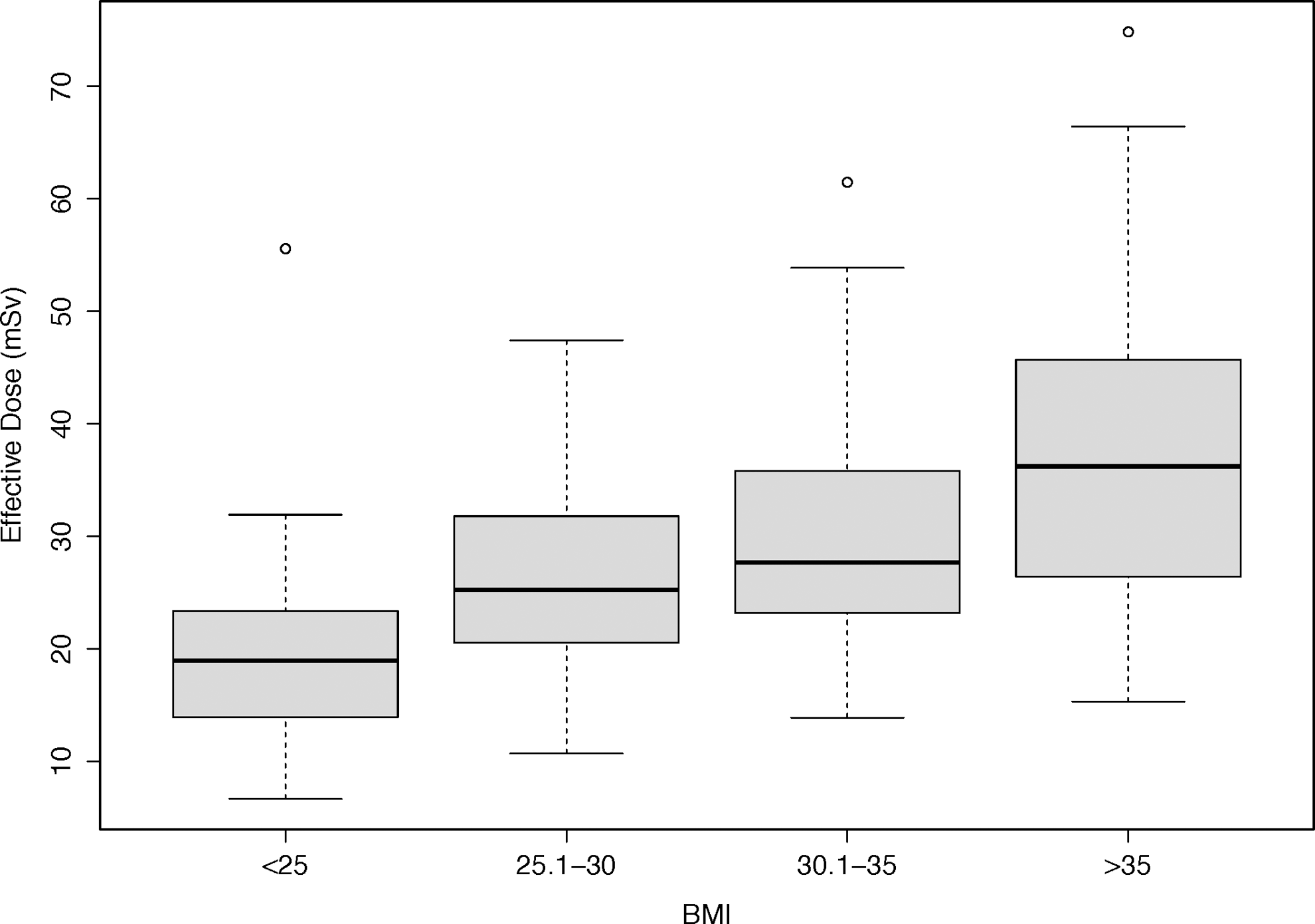
Distribution of effective doses from renal mass protocol CT by body mass index (BMI).

Distribution of effective doses from renal mass protocol CT by body mass index (BMI) in males and females.
CI=confidence interval; BMI=body mass index; IQR=interquartile range
On multivariable analyses BMI, age, and sex maintained independent associations with the effective dose (Table 3). Compared with women, men had a 4.5 mSv increase in the effective dose when adjusted for other characteristics. Compared with normal weight (BMI ≤25) patients, higher BMIs were independently associated with higher effective doses, with a 6.0, 9.1, and 18.5 mSv increase in the effective doses for overweight, obese, and morbidly obese patients, respectively (all P ≤0.001).
CI=confidence interval; BMI=body mass index.
Discussion
Currently, RMP-CT is the mainstay imaging modality for diagnosis, characterization, and surveillance of renal masses and represents a common urologic imaging study. We found a median effective dose of 26.1 mSv for one RMP-CT. Furthermore, the effective dose was strongly associated with body habitus. Morbidly obese patients incurred roughly double the effective dose compared with normal weight patients.
In the present study, the median effective dose was 26.1 (IQR, 20.6–35.3) mSv. A previously published study reported an effective dose of 31 (21–43) mSv. 4 A recent analysis of CT radiation doses in Saskatchewan, Canada, reported a mean dose of 29.5 (±13.8) mSv for multiphase abdomen-pelvis studies. 9 While the median dose in our study is lower, the variations of effective doses are similarly wide. These findings highlight the substantial effective doses associated with this type of imaging. Moreover, while median doses are high, the individual effective doses may be much higher; in fact, in this study, the effective dose was >35 mSv in 25% of the patients. Another study reported doses as high as 90 mSv for a single study. 4 Importantly, in the setting of the small renal mass, imaging procedures would not typically be limited to one study; rather, the patient often undergoes serial imaging for surveillance or follow-up after treatment.
Several patient characteristics were associated with the effective dose on univariable analyses. When stratified by BMI, proportional increase in the effective doses is demonstrated, with 19, 25, 28, 36 mSv for normal weight, overweight, obese, and morbidly obese patients, respectively (Table 2). Morbidly obese patients incur almost twice the dose compared with normal weight patients. With obesity being a risk factor for renal cell carcinoma, the obese population appears to be at highest risk of significant radiation exposure associated with the management of renal masses. At the same time, the association between obesity and medical comorbidities further enhances the potential of these patients to receive radiographic studies and thus even higher cumulative radiation exposure.
On multivariable analyses, BMI and male sex were associated with markedly increased effective doses. Compared with normal weight patients, we have shown 6, 9, and 18 mSv increases in the effective doses for overweight, obese, and morbidly obese patients. Obesity has been previously shown to increase the effective doses. A study from our institution has demonstrated similar associations between effective dose during percutaneous nephrolithotomy and BMI, 10 whereby morbidly obese patients incur more than double the dose of normal weight patients. Similar findings were reported in low-dose CT for evaluation of renal colic. 11
It is not surprising that larger patients would receive a higher radiation dose because a greater number of photons are needed to maintain image quality in the setting of greater photon beam attenuation. In taller patients, imaged body length is increased resulting in higher effective dose because of increased scan coverage. Quantification of this phenomenon in the clinical setting emphasizes the marked impact of obesity on radiation exposure.
In both univariable and multivariable analyses, male patients incurred higher radiation exposures. When adjusted for other characteristics, the multivariable model shows that the effective doses for men are on average 4.5 mSv higher compared with women. This finding may be because of differences in body composition, and specifically the distribution of muscle mass and adipose tissue, between sexes.
In a previous study, effective doses associated with the different types of CT imaging were correlated to the risk of malignancies attributable to radiation. 4 In their study, the attributable risk of radiation-induced malignancy for one multiphase abdomen pelvis CT was estimated as 0.8 to 11.1 malignancies per 1000 patients. 4 The authors have also estimated that in 60 year-old patients, every 660 to 700 scans of this type would result in a radiation-induced malignancy whereas the risk of radiation-induced malignancies in younger patients is substantially higher. 4 In the setting of a renal mass, these numbers should be interpreted cautiously, because these patients typically undergo serial imaging, thereby drastically reducing the number of patients to be scanned to induce one malignancy. For example, a patient with a diagnosis of renal mass by means of a renal mass protocol CT and undergoing surveillance with yearly CT imaging for 5 years, one could estimate a radiation-induced malignancy developing in 1 in 100 patients.
The current study is not void of limitations. First, the retrospective nature of the analysis may introduce inherent biases. Second, we did not analyze parameters other than BMI, body weight, and height for assessment of body habitus; however, BMI is the most commonly used metric in the clinical setting. In addition, minor variations in radiation exposure based on the various makes, models, detector number, and ages of scanners may have reduced our precision in the estimates; however, because these variations are common in most imaging centers, these may make our data more generalizable. Finally, the effective dose estimates were based on dose-length product, and we were not able to provide organ-specific doses to associate with body habitus. This estimation of the effective dose, however, has been shown to be reliable and reproducible. 12
In spite of the aforementioned limitations, this is the first study to quantify effective doses for RMP-CT protocols based on a patient's body habitus. The findings of our study suggest that radiation exposure in patients undergoing evaluation for a renal mass is substantial. Based on our results, we do not suggest replacing current diagnostic strategies for renal masses but rather attempt to increase awareness to radiation exposure in these patients and draw attention to strategies to reduce radiation exposure, especially in the setting of serial imaging, typically performed for follow-up and surveillance. We suggest that alternative imaging schedules and/or alternative imaging modalities (ultrasonography, contrast-enhanced ultrasonography, reduced dose CT, magnetic resonance imaging, etc.) should be explored. Our data should be considered when devising clinical guidelines for the management of the small renal mass, specifically with regard to follow-up imaging regimens as well as for active surveillance protocols.
Conclusions
In this study, the median effective dose for renal mass protocol CT was 26.1 mSv, indicating substantial radiation exposure associated with this imaging procedure. We have also demonstrated that normal weight, overweight, obese, and morbidly obese patients incur effective doses of 18.9, 25.2, 27.7, and 36.2 mSv, respectively. On average, men received 4.5 mSv higher doses compared with women. While increasing awareness to patients' radiation exposure, these data can be valuable for devising imaging protocols for surveillance and post-treatment follow-up for patients with a renal mass.
Footnotes
Disclosure Statement
No competing financial interests exist.