
Abstract
Purpose:
To present oncologic results of laparoscopic radical prostatectomy (LRP) monotherapy for men with high-risk, localized prostate cancer, and to find factors associated with a good prognosis via surgery alone.
Patients and Methods:
Between 2002 and 2009, 241 men underwent LRP at an Asian tertiary referral center. Among them, we retrospectively identified 85 (35.3%) men who met the D'Amico's high-risk criteria: Prostate-specific antigen level >20 ng/mL, Gleason score of 8 to 10, or clinical stage ≥T2c. Perioperative parameters were analyzed against biochemical recurrence (BCR)-free survival.
Results:
At a median follow-up of 54 months, BCR developed in 28 (34.1%), with an actuarial BCR-free survival rate of 63.3% at 5 years. Pathologically, 37.6% of the men had organ-confined (OC) disease. Positive surgical margins (PSM) were identified in 49.4% of the patients. A favorable pathologic outcome, defined as OC(+)PSM(−), was observed in 24 patients and associated with a 5-year BCR-free survival rate of 87.0%, compared with 100%, 54.0%, and 46.4% in men with OC(+)PSM(+), OC(−)PSM(−) and OC(−)PSM(+) disease (log-rank, P=0.008). The overall positive lymph node rate was 14.1%. Men (65.9%) with only one D'Amico risk factor had a 5-year BCR-free survival rate of 76.9%, compared with 34.6% in men (34.1%) with ≥2 risk factors (log-rank, P<0.001).
Conclusions:
Radical prostatectomy monotherapy performed laparoscopically or robotically appears to be an option for high-risk prostate cancer, especially in men with a single D'Amico risk factor. Men with ≥2 risk factors are more prone for BCR to develop after surgery and may need second-line therapy.
Introduction
B
Some patients, however, fail to respond to monotherapy and eventually need multiple therapies. Multimodal treatment using combined ADT and radiotherapy (RT) has improved survival rates for patients with high-risk prostate cancer and is the preferred treatment at present. 7 Several recent studies have demonstrated that RP is also an acceptable treatment alternative with a 15-year prostate cancer-specific survival of more than 80%. 8 –10
Laparoscopic radical prostatectomy (LRP) has been considered an oncologic alternative to open retropubic RP for localized prostate cancer. 11 Data regarding the oncologic effectiveness of LRP for high-risk prostate cancer are still limited, however. We started to perform LRP for men with prostate cancer in 2002. 12 Among them, 85 men were stratified as having high-risk disease preoperatively according to the D'Amico classification. 13 We report the midterm oncologic outcomes of these men after LRP monotherapy and try to find factors associated with a good prognosis via surgery alone.
Patients and Methods
Between October 2002 and June 2009, 241 men underwent LRP for clinically localized prostate cancers at our institution, an Asian tertiary referral center. LRP was performed with a transperitoneal approach in the initial 23 men and an extraperitoneal method in the remaining 218.
All men received standard pelvic lymph node dissection (sPLND) with the template including the external iliac and obturator fossa groups, despite preoperative risk strata. All procedures were performed by two experienced surgeons (SCC and MKL). Among them, we retrospectively identified 85 (35.3%) men who met the D'Amico high-risk criteria: PSA level ≥20 ng/mL, Gleason score of 8 to 10, or clinical stage ≥T2c. 13 No neoadjuvant ADT was administered before LRP.
The preoperative clinical parameters including age, preoperative PSA level, biopsy Gleason score, and clinical stages were reviewed. Pathologic data including the Gleason score, pathologic stages, and positive surgical margins (PSM) were reviewed with the routine sectioning method. PSM was defined as tumor present at the inked margin of the specimen. Pathologic staging was performed using the 2002 American Joint Committee on Cancer Tumor Node Metastasis system, and Gleason scoring was assigned according to modern convention. Recurrence of disease was defined as a serum PSA value ≥0.2 ng/mL in at least two consecutive measurements or initiation of secondary therapy. Recurrence-free survival was defined as the time between surgery and the first PSA increase (≥0.2 ng/mL). Men who had a detectable postoperative PSA level immediately after surgery or received adjuvant treatment (hormone or radiation) before an increased postoperative PSA were assumed to have experienced failure at the time of surgery (ie, recurrence-free survival=0 months).
After LRP, all men except three received regular PSA monitoring and digital rectal examination at our clinics every 3 months for the first 2 years and then every 6 months thereafter. A total of three (3.5%) patients with no follow-up data were included for evaluation of preoperative and pathologic characteristics but not in the oncologic analysis.
The biochemical recurrence (BCR)-free survival was analyzed using the Kaplan-Meier method, and the log-rank test was used to compare survival curves of subgroups. Cox proportional hazards models were used to determine which clinical and pathologic factors were significant predictors of BCR after LRP monotherapy.
The Institutional Review Board of National Taiwan University Hospital approved collection and analysis of retrospective data (201203103RIC). A P-value less than 0.05 was considered statistically significant. All analyses were performed with Statistical Package for the Social Science software (SPSS, 13th ed., Chicago, IL).
Results
The preoperative patient characteristics are listed in Table 1. The surgical procedure was a transperitoneal LRP in nine (10.6%) patients and an extraperitoneal LRP in 76 (89.4%) patients. According to the D'Amico risk classification, 56 (65.9%) men had only one risk factor and 29 (34.1%) had ≥2 risk factors. None of these patients received neoadjuvant therapy before surgery.
PSA=prostate-specific antigen; GS=Gleason score.
The postoperative pathologic parameters are listed in Table 2. A PSM was identified in 42 (49.4%) patients, including 7 of 32 with pT2 (21.9%), 11 of 13 with pT3a (84.6%), 21 of 35 with pT3b (60.0%), and 3 of 5 with pT4 (60.0%) disease. Extracapsular extension (ECE) and seminal vesicle invasion (SVI) occurred in 40 (47.1%) and 36 (42.4%) men with high-risk prostate cancer, respectively. Positive pelvic lymph node metastases were reported in 12 (14.1%) patients.
Favorable pathologic outcome was defined as organ-confined disease with negative margins.
82 men were included in the oncologic analysis.
At a median follow-up of 54 months (range 18–98 mos), 28 (34.1%) of the 82 evaluable patients had BCR, three developed clinical recurrences developed in 3 (two local recurrences, one metastatic disease), and one died of prostate cancer. The median time to progression was 6.5 months. Eleven patients with positive nodal disease or a detectable postoperative PSA level after surgery received immediate salvage or adjuvant therapy (RT alone in 1, ADT alone in 6, and a combination of RT and ADT in 4).
The probability of BCR-free survival in men with high-risk prostate cancer after LRP monotherapy is shown in Figure 1. The actuarial BCR-free survival rates at 3 and 5 years were 69.1% and 63.3%, respectively. When stratified by the number of D'Amico high-risk factors, the 5-year BCR-free survival rate was 76.9% in men with only one factor vs 34.6% in men with ≥2 factors (log-rank P<0.001, Fig. 2). A favorable pathologic outcome, defined as organ-confined (OC) disease with negative margins (OC(+)PSM(−)), was observed in 24 (28.2%) patients and associated with a 5-year BCR-free survival rate of 87.0%, compared with rates of 100%, 54.0%, and 46.4% in men with OC(+)PSM(+), OC(−)PSM(−), and OC(−)PSM(+) disease, respectively (log-rank P=0.008, Fig. 3).

Overall biochemical recurrence-free survival after laparoscopic radical prostatectomy (LRP) monotherapy for men with high-risk prostate cancer.
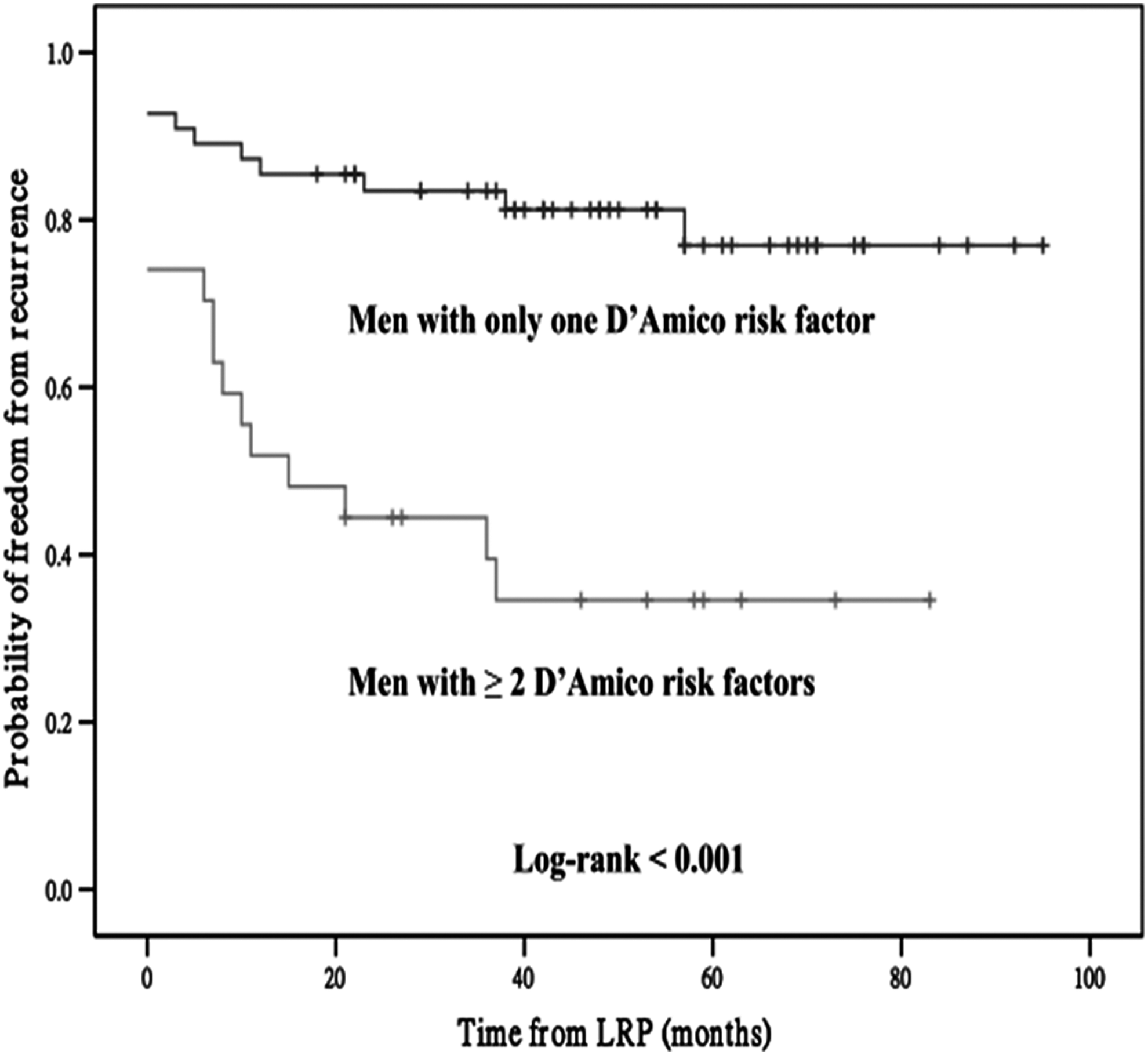
Biochemical recurrence-free survival after laparoscopic radical prostatectomy (LRP) monotherapy for men with high-risk prostate cancer according to the number of D'Amico risk factors.
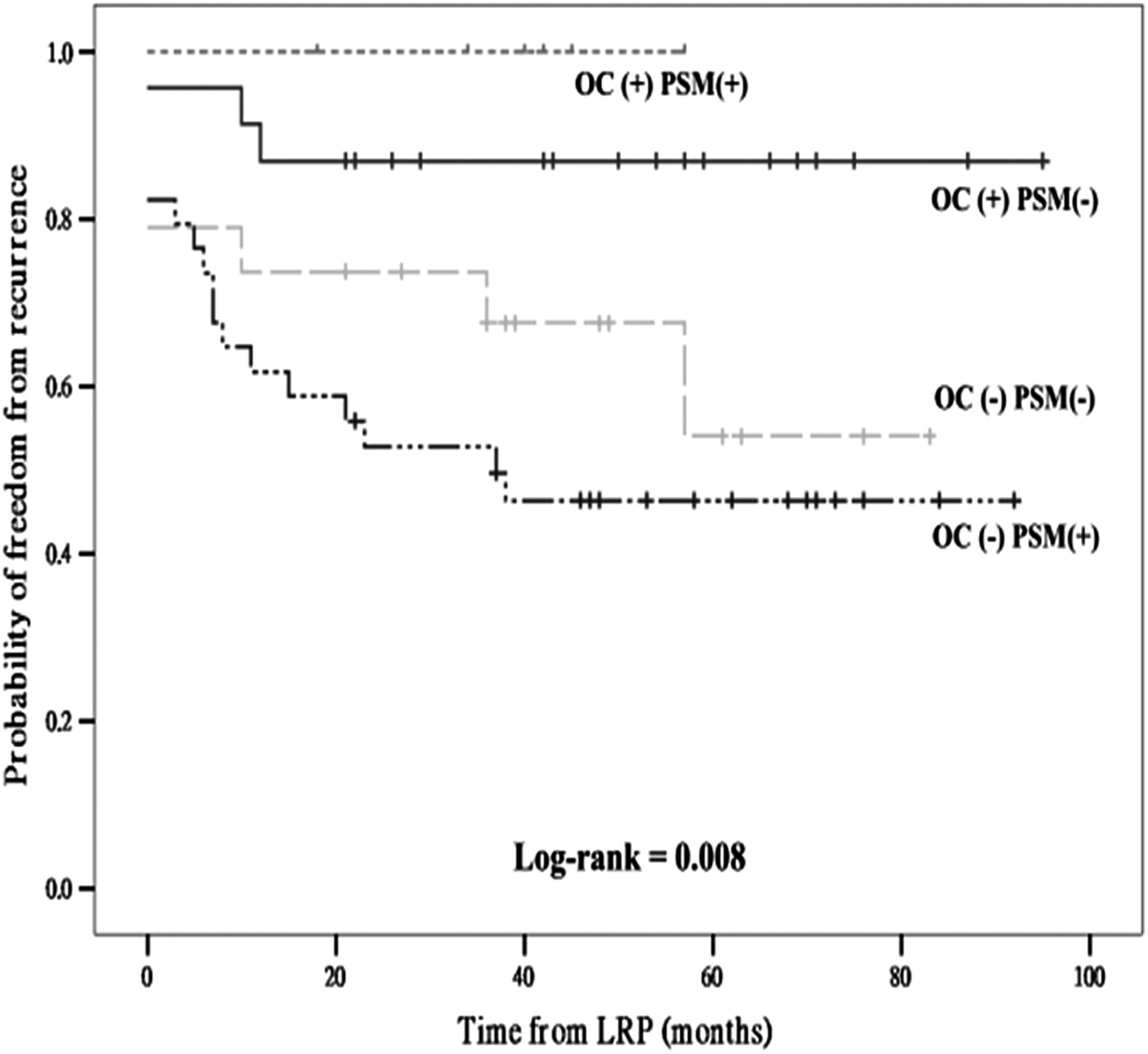
Biochemical recurrence-free survival after laparoscopic radical prostatectomy (LRP) monotherapy for men with high-risk prostate cancer according to organ-confined disease and margin status. OC=organ-confined disease; PSM=positive surgical margin.
Table 3 shows the Cox proportional hazards model of the preoperative and pathologic predictors of time to BCR in men with high-risk prostate cancer after LRP monotherapy. None of the D'Amico high-risk factors, including PSA level ≥20 ng/mL, biopsy Gleason score ≥8, and clinical stage ≥T2c, was associated with BCR independently in this multivariate analysis. Compared with men with only one risk factor, however, men stratified with ≥2 risk factors had a significantly higher risk of BCR developing after surgery (hazard ratio [HR] 4.2, 95% confidence interval [CI] 1.9–9.1, P<0.001). Among pathologic variables, only pathologic stage ≥pT3 (HR 5.4, 95% CI 1.6–17.9, P=0.006), but not the pathologic Gleason score or presence of a PSM, was the independent predictor of BCR.
HR=hazard ratio; CI=confidence interval; PSA=prostate-specific antigen; PSM=positive surgical margin.
Discussion
The treatment of men with high-risk localized prostate cancer remains a clinical challenge. The current literature suggests multimodal treatment using combined definitive RT and ADT for men with high-risk prostate cancer. In a phase III randomized trial conducted by the Radiation Therapy Oncology Group (protocol 92-02), long-term ADT (2 years) plus RT for patients with Gleason 8 to 10 locally advanced prostate cancer was associated with a 5-year overall survival rate of 81.0%, disease-free survival rate of 41.9%, cause-specific survival rate of 93.4%, and biochemical failure rate of 33.4%. 7 This means approximately one-third of patients with high-risk disease undergoing RT and long-term ADT succumb to biochemical progression within 5 years and need second-line therapy. There are few proven effective local therapy options, however, and based on a consideration that salvage RP after failed RT is extremely challenging and might be associated with a high incidence of morbidities, 14 many men are treated with long-term ADT, thus submitting them to untoward adverse effects of ADT 15 even though the majority of them might have only residual localized disease. On the other hand, it would be much easier to apply adjuvant or salvage therapy if the patient is treated primarily with RP.
Several retrospective studies have addressed the long-term oncologic effectiveness of open RP for high-risk or locally advanced prostate cancer, with different risk definitions and variable reported outcomes. In general, 5-year BCR-free survival rates of 24% to 68% have been reported; specifically, when using D'Amico criteria to define high-risk disease, the 5-year BCR-free rates ranged from 36% to 68%. 16 –19 The majority of patients in these studies, however, received additional treatments, and thus the results reflected a composite response generated by combination therapy rather than RP alone. Loeb and colleagues 8 reported on 175 men with D'Amico high-risk prostate cancer who predominantly underwent RP monotherapy between 1992 and 2008. At RP, 36% had organ-confined disease. The 5- and 10-year BCR-free survival rates were about 75% (estimated) and 68%, respectively. 8
The only comparative analysis performed by Boorijian and associates 20 retrospectively examined the long-term outcomes of men with high-risk prostate cancer after RP and after RT with or without ADT therapy. The authors defined high-risk prostate cancer according to NCCN guidelines and found that compared with RT plus ADT, surgery alone provided similar long-term cancer control in terms of 10-year systemic progression-free survival and cancer-specific survival, and even a superior 10-year overall survival rate.
Recently, there has been a shift in technique from open RP to less invasive approaches, such as LRP and robot-assisted laparoscopic prostatectomy (RALP). For men with clinically localized prostate cancer, the endoscopic approach is an oncologically and functionally effective alternative to its open counterpart. 11 Studies reporting the outcomes of these minimally invasive methods for high-risk disease are limited, however (Table 4). Touijer and coworkers 21 reviewed 1231 consecutive patients, of whom 146 (12%) were stratified as having high-risk prostate cancer according to the Kattan nomogram. The probability of a 5-year BCR-free survival rate for those men was 53%. Ploussard and colleagues 22 also demonstrated the outcomes of extraperitoneal LRP with sPLND in 110 men with high-risk prostate cancer based on the D'Amico classification. They noted about 35% of high-risk cancer was OC. The ECE, SVI, and PSM rates were 65%, 25%, and 39%, respectively. The BCR-free survival rate at 3 years was approximately 70%. 22
Transperitoneal laparoscopic radical prostatectomy (TPLRP).
Extraperitoneal laparoscopic radical prostatectomy (EPLRP).
TP/EP LRP.
Robot-assisted LRP.
OC=organ-confined; PSM=positive surgical margin; LNI=lymph node positive; BCR=biochemical recurrence; NCCN=National Comprehensive Control Network.
With the advent of the da Vinci® Surgical System, several RALP series focusing on high-risk prostate cancer have been reported. Preliminary experience has revealed excellent pathologic outcomes, but a longer follow-up is needed to confirm its oncologic competence. 23 –28
In the present study, we believed a median follow-up of 4.5 years was appropriate, because BCR usually develops during the first 2 years. Although BCR remained common (34.1%) in the present cohort, an even higher proportion of these patients (∼66%) were disease-free after LRP monotherapy. According to the D'Amico classification, 65.9% of our high-risk prostate cancer patients had only one risk factor, and more than three quarters (76.9%) of them enjoyed a 5-year BCR-free survival, compared with only 34.6% in men with ≥2 risk factors. Of note, the number of D'Amico high-risk factors was the only preoperative independent variable that significantly predicted disease recurrence, and the risk of development of BCR in men with ≥2 risk factors was approximately four times greater than in men with one risk factor. That means in selected groups of patients with high-risk disease, LRP alone is able to provide satisfactory oncologic results.
Even though the 5-year BCR-free survival in the present study was comparable to that of the series from Touijer and associates 21 and Wambi and coworkers, 28 there is definitely room for improvement. Three Phase III randomized trials of adjuvant RT vs a wait-and-see policy have reported the benefits of immediate postoperative irradiation for patients with advanced prostate cancer undergoing RP: The Southwest Oncology Group (SWOG) trial 8794, 29 the European Organization for Research and Treatment of Cancer trial 22911, 30 and the German ARO 96-02 trial. 31 Generally, regardless of patient selection and treatment, these trials demonstrated significant improvements in reducing local failure and a 50% to 60% reduction in the risk of BCR after RP and adjuvant RT. On top of that, SWOG 8794 reported that adjuvant RT was also associated with improved metastasis-free and overall survival and the need for salvage ADT. 29
When evaluating the role of minimally invasive surgery in high-risk prostate cancer, it is important to ask two questions. First, what type of lymph node dissecting template should be considered? Recent data have demonstrated an extended PLND (ePLND) involving removal of the obturator, external iliac, and hypogastric nodes with or without the presacral and common iliac nodes is capable of retrieving more lymph nodes, detecting more lymph node metastases, and increasing the accuracy of nodal staging to define the extent and location of disease. In addition, ePLND might play a therapeutic role in a subset of patients with a limited lymph node burden as well. 32 Accordingly, ePLND is currently recommended by EAU guidelines for patients with high-risk prostate cancer. 5
The next question is whether PLND performed laparoscopically or robotically can be done as well as open surgery? A group from Memorial Sloan-Kettering Cancer Center reviewed 648 men with clinically localized prostate cancer who underwent RP and PLND and found that sPLND through a transperitoneal laparoscopic approach was a feasible procedure, and demonstrated similar oncologic adequacy in terms of nodal yields (median 13.5 vs 12, P=0.13) and detection rate (15.1% vs 10.2%, P=0.62) compared with open PLND. 33 With a mean nodal yield of 21 (range 9 to 55) and a lymph node metastases rate of 17%, Wyler and colleagues 34 also demonstrated laparoscopic ePLND was a safe and effective equivalent to open surgery for high-risk prostate cancer.
In the present study, men with high-risk disease were predominantly treated with extraperitoneal LRP and sPLND, which provided a positive lymph node rate of 14.1% and an average nodal count of 9.1 (median 8, range 2–22). These results seemed to be comparable with other series, despite the inherent limitations of the extraperitoneal approach in dissecting the hypogastric and common iliac nodes. It might potentially underestimate the true incidence of nodal metastases in prostate cancer, particularly in high-risk disease, because up to 50% of lymph node metastases are located along the hypogastric vessels. In our 12 patients with positive nodal disease, 6 who received immediate ADT and 6 who opted for observation remained disease-free for a median of 57.5 months without any secondary therapy.
Another consideration about the role of surgery for high-risk prostate cancer is the nerve-sparing technique during LRP. Among the 85 men, 55.4% underwent nerve-sparing surgeries (bilateral 24.3%, unilateral 31.1%), which was significantly lower than that in the low-to-intermediate-risk groups (77.6%, P=0.001) in our series. The PSM rate in this group of patients was 56.1%. Of note, more than two-thirds (68.3%) of patients with high-risk disease receiving nerve-sparing LRP remained disease-free at a median follow-up of 4.5 years. These results were similar to those in previous open and robotic series. A nerve-sparing procedure during minimally invasive surgery for some high-risk prostate cancer is feasible and safe in selected patients.
We recognize that our study might be flawed by several limitations. First, the nature of a retrospective chart review lends itself to some criticisms. Second, the study power was limited by the relatively small sample size because the prevalence rate of prostate cancer in Asian men is much lower than in Western countries. In addition, the study outcomes might be biased by patient selection because the cohort represented a younger and healthier population for surgery and might not be representative of all men with high-risk prostate cancer.
Another caveat in the present study is that men with OC(+)PSM(+) had a 5-year BCR-free survival rate of 100%, which was better than that in men with OC(+)PSM(−) disease (Fig. 3). A possible reason for this point is the limited case number in this group—only 6 men with OC(+)PSM(+), compared with 24 with OC(+)PSM(−), 19 with OC(−)PSM(−) and 36 with OC(−)PSM(+), and this may have reduced its power. The other possibility is that some of these PSM might be “capsular incisions” with a small PSM, so there was no detrimental effect on our BCR-free survival. Of note, all six patients with pathologic OC(+)PSM(+) disease had only one D'Amico risk factor, which is probably another explanation for their good outcomes. Furthermore, in our multivariate analysis model, the presence of PSM did not predict BCR in men with high-risk prostate cancer after LRP. The two major independent predictors were the number of D'Amico factors and pathologic stage (≥pT3).
As mentioned above, in the spectrum of treatment options for high-risk prostate cancer, a combination of ADT and RT or open RP is most commonly used. The benefit of ADT+RT treatment is low invasiveness, but it is associated with possible complications after RT and long-term ADT, and a lack of effective salvage treatment. A more aggressive primary treatment with RP may avoid those problems, provide better control of the primary tumor, and accurately define the extent of disease. In the era of minimally invasive surgery, RP performed by laparoscopic or robot-assisted techniques has resulted in decreased perioperative morbidities and comparable oncologic and functional outcomes, and should be considered as a less invasive surgical alternative for managing high-risk prostate cancer.
Conclusions
LRP monotherapy in our hands provided a 5-year BCR-free survival in 63.3% of men with high-risk localized prostate cancer, which is compatible with concurrent series. Moreover, in selected patients with only one D'Amico high-risk factor, LRP was able to demonstrate a better BCR-free survival rate of 76.9% at 5 years. Men with ≥2 risk factors were more prone to have BCR develop after surgery and may need second-line therapy or a consultation for RT+ADT. Therefore, we believe that RP performed laparoscopically or robotically appears to be an attractive and feasible option for this subgroup of patients. The role of immediate adjuvant therapy in long-term survival should be further evaluated in a prospective study.
Footnotes
Disclosure Statement
No competing financial interests exist.