
Abstract
Background and Purpose:
Surgery continues to be the main form of treatment for patients with renal tumors. We create a more practical and intuitive score for renal tumor classification.
Patients and Methods:
Eighty patients underwent surgery for renal tumors and were prospectively enrolled. The tumors were classified using the following variables: (1) tumor size, (2) endophytic or exophytic tumor, (3) longitudinal location of the tumor, (4) the extent of the impairment of the renal parenchyma, (5) relationship with the renal sinus, and (6) anterior or posterior.
Results:
The mean operative time, tumor size,and bleeding increased proportionally to the increased complexity of the tumor measured by scores (P<0.0001, P<0.0001, and P=0.036, respectively). The mean total score was 8.7 points for patients undergoing partial nephrectomy (PN) and 14.4 points for those undergoing radical nephrectomy (RN) (P<0.0001). Patients with larger tumors, completely endophytic, which exceeded the renal medulla, and were centrally located, underwent RN more often (86.7% − P<0.0001, 64% − P=0.01, 77% − P<0.0001, and 78.9% − P<0.0001, respectively). In univariate analysis, RN was associated with tumors larger than 7 cm (P=0.001), tumors that exceeded the renal medullary (<0.001), centrally located tumors (odds ration [OR]=150, P<0.001), and tumors of high complexity (P<0.001). Analysis showed no association between complications and variables in the score. The findings were similar when the tumors were evaluated with the R.E.N.A.L. score system.
Conclusion:
Surgical Approach Renal Ranking is a simple, practical and intuitive classification for renal tumors that can be used in the decision-making process and to predict outcomes in the surgical treatment of patients with renal tumors.
Introduction
S
When surgery becomes an option, both the technical ability of the surgeon and the anatomic findings of the renal tumor are important factors. The analysis of each parameter is essential in considering the procedure to opt for and what will be the results of the adopted treatment. Recently, Kutikov and Uzzo 8 have suggested the R.E.N.A.L. (radius; exophytic/endophytic properties; nearness of tumor portion to the collecting system; anterior/posterior; location relative to the polar line) nephrometry score as a scoring system to quantify relevant anatomic findings that are fundamental to clinical decision taking and in making effective comparisons. This has created a new paradigm in the handling of patients with renal tumors.
Around the same period, Italian researchers suggested another anatomic classification—the PADUA (preoperative aspects and dimensions used for an anatomical) score—for renal tumors, based on presurgery aspects and dimensions in patients eligible to nephron-sparing surgery. 9 Since then, several research studies have been published in the medical literature evaluating the utility of such scores in predicting the need for surgery and complications in the management of renal tumor. 10 –12 Nonetheless, despite this great benefit added to the diagnosis and therapeutic armamentarium of renal tumor, these scores present anatomical variables that are difficult to evaluate in the day-to-day practice of clinical urology, besides the fact that there is no similar score technique validated in Brazil.
The objective of this research is to create a new scoring system of renal tumor that might be more practical, intuitive, and quantifiable, as well as to evaluate its capacity in predicting results and complications in the surgical management of kidney tumors in a university hospital. This new score was also compared with the R.E.N.A.L. score system.
Patients and Methods
Between January 2011 and January 2012, 80 patients within the age range of 23 and 87 years underwent renal tumor surgery at the Federal University of Sao Paulo. A prospective study was conducted. All patients initially underwent a preoperative CT scan and/or magnetic resonance imaging (MRI) evaluation.
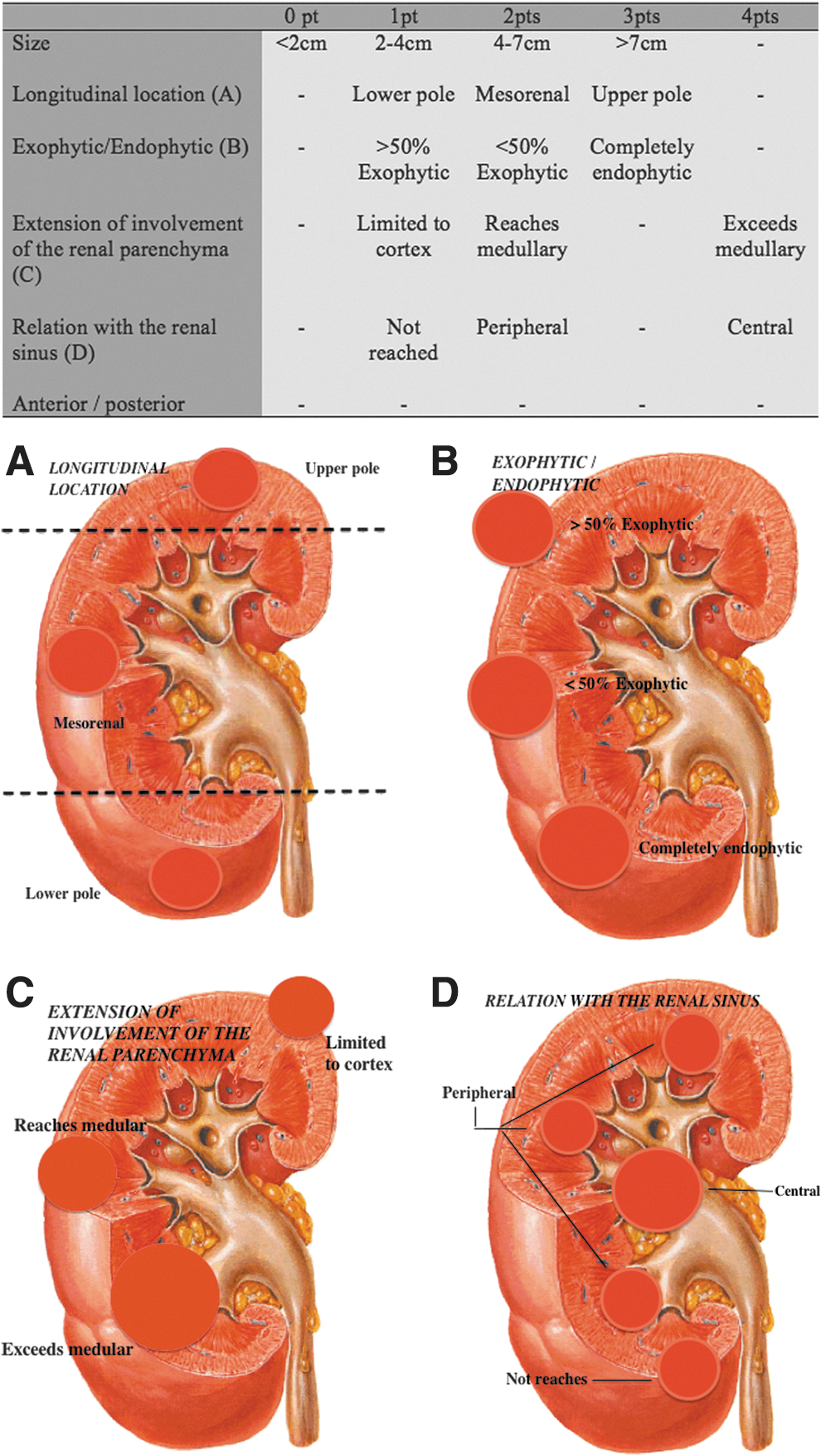
The scanned tumors were classified by a urologist and a radiologist taking into account the following variables: (1) tumor size, (2) endophytic or exophytic, (3) longitudinal location, (4) extension of involvement of the renal parenchyma, (5) relation with the renal sinus, and (6) anterior or posterior location.
A weight was assigned to each variable to form a rating scale ranging from 4 to 17 points. Tumors were classified into four categories according to their size, as follows: (0) <2 cm, (1) 2 to 4 cm, (3) 4 to 7 cm, and (4) >7 cm. The endophytic or exophytic characteristic was classified in the following manner: (1) >50% exophytic, (2) <50% exophytic; (3) completely endophytic. Longitudinal classification of the tumors was divided into three categories: (1) lower pole, (2) mesorenal, and (3) upper pole. Because of the increased surgical relevance of the variables regarding the extension of the compromised renal parenchyma and the relation with the renal sinus, greater weights were assigned to these components, and the resulting classification was as follows: (1) limited to cortex, (2) reaches medullary, (4) exceeds medullary, and (1) does not attain the renal sinus, (2) peripheral, (4) central, respectively (Fig. 1).
Surgical Approach Renal Ranking.
The tumors were classified as being of low, medium, and high complexity whenever the score added up to 4 to 8, 9 to 12, and 13 to 17, respectively. The patients were treated with partial nephrectomy (PN) or RN, through a laparoscopic, robot-assisted, or open procedure. The R.E.N.A.L. score system was also calculated for all tumors examined.
The differences between numerical variables were established through the analysis of variance test. Comparisons between proportions were performed through the chi-square test. Logistical regression analysis was used to evaluate the capacity of the scoring system in predicting perioperative complications and decisions concerning the type of surgery. The results were considered statistically significant when the P value was below 5% (P<0.05). The analysis was performed using the PAWS Statistics 17 program.
Results
In this study, 80 patients were involved, 56 of whom were males (70%) and 24 (30%) females. Age varied between 23 and 87 years with an average age of 55.6 years. The average surgery time was 144.4 minutes, and average tumor size was 4.8 cm. Laparoscopic partial nephrectomy (LPN) was the type of surgery most performed (51.3%), renal-cell carcinoma (RCC) was the histologic type most commonly found (68.8%), and pT1a was the most frequent stage found (50.8%) (Table 1).
Patients were divided into three groups according to the complexity of the tumor as per score classification: Group 1 patients with low complexity tumors (4–8), group 2 with moderate complexity (9–12), and group 3 with high complexity (13–17). The average surgery time, tumor size, and estimated bleeding increased according to the complexity of the tumor, as classified by the Surgical Approach Renal Ranking (SARR) scoring system, with a statistical significance P<0.0001, P<0.0001, and P=0.036, respectively (Table 2).
Analysis of variance (ANOVA) test.
The patients were stratified and evaluated with respect to the type of surgery: PN×RN. The average of the total sum of the score was 8.7 points for those patients who underwent PN and 14.4 points for those who underwent RN with statistical significance (P<0.0001). When variables were evaluated separately, it was observed that patients with bigger tumors, completely endophytic that extended beyond the renal medulla, and were centrally located were more frequently those who underwent RN (86.7% − P<0.0001; 64% − P=0.01; 77% − P<0.0001, and 78.9% − P<0.0001, respectively). The data show that the longitudinal location (lower pole tumor, mesorenal, or upper pole) did not interfere in the decision for surgery type when evaluated in isolation (P=0.19). The findings were similar when the tumors were evaluated with the R.E.N.A.L. score system (Table 3).
Chi-square test.
R.E.N.A.L.=radius; exophytic/endophytic; nearness; anterior/posterior; location; SARR=Surgical Approach Renal Ranking.
In the univariate analysis, RN was significantly associated with tumors larger than 7 cm (odds ratio [OR]=16.6 − P=0.001), tumors that extended beyond the renal medulla (OR=33.75 − P<0.001), tumors of central location (OR=150 − P<0.001), and high-complexity tumors (OR=39.53 − P<0.001). No RN association was found with totally endophytic tumors (OR=1.71 − P=0.307), of upper pole (OR=2.34 − P=0.07), and posterior location (OR=2.02 − P=0.25). When the univariate analysis was performed with the R.E.N.A.L. score system, results were similar (Table 4).
Radical nephrectomy reference=1; partial nephrectomy reference=0.
R.E.N.A.L.=radius; exophytic/endophytic; nearness; anterior/posterior; location; SARR=Surgical Approach Renal Ranking; OR=odds ratio; CI=confidence interval.
The univariate logistical regression did not show any association between complications and the variables that make up both scores (Table 5).
R.E.N.A.L.=radius; exophytic/endophytic; nearness; anterior/posterior; location; SARR=Surgical Approach Renal Ranking; OR=odds ratio; CI=confidence interval.
When only PNs were assessed in relation to the sum total score, margin status, and complications, the scores are equal in predicting positive margin status or complications (no significant difference between groups). The SARR score, however, can predict the type of procedure (open or laparoscopic), depending on the complexity of the tumor. Patients with more complex tumors (highest score) more often undergo PN open than LPN (P=0.047). Also, there was also a difference for the R.E.N.A.L. score system but not statistically significant (P=0.07) (Table 6).
R.E.N.A.L.=radius; exophytic/endophytic; nearness; anterior/posterior; location; SARR=Surgical Approach Renal Ranking.
Discussion
Imaging breakthroughs allowed for an incidental increase in the number of diagnoses of renal masses. 13 In parallel, the surgical management of such tumors has been changing from RN to the so-called nephron-sparing surgeries. The development of minimally invasive techniques has given rise to LPN and cryoablation as as examples of acceptable alternatives in appropriate situations. 14
The anatomic complexity of the tumor remains as the main characteristic that urologists use to determine the surgery type and treatment strategy for renal tumor. Recently, three different systems of valuation have been reported as a means of standardizing and quantifying the complexity of tumors. 8,9,15 These were developed to be a common language when discussing the geometry of the anatomy and the complexity of renal masses. Furthermore, these results have the power of influencing the choice of type of treatment and of foreseeing complication risks.
PADUA and the R.E.N.A.L. score involve similar components allowing for a more comprehensive description of the tumor size, exophytic/endophytic characteristics, polarity, anterior/posterior location, and proximity to the collecting system. Each component is attributed a score giving a uniform classification. The central index, however, is a completely different system that uses a relatively complex mathematical measuring concept and defines the centrality of the tumor based on the distance ratio between the center of the tumor and the kidney, and the tumor radius. 15
This study proposes a presurgery classification system for the management of renal tumor integrating the most important anatomic variables described in the literature. It was developed with the purpose of making the urologist's surgery decision taking more practical, intuitive, and efficient when evaluating a renal tumor, apart from allowing for the prognosis of complication risks.
The size of the tumor is the main prognosis factor for RCC. Such observation is the result of several published reports on this matter 16 and has led to frequent propositions for changing the staging of the illness. 17 It is well-known that renal tumors incidentally diagnosed are smaller and bear less malignancy risk. 18 The reduction in the size of renal tumors has played an important role in today's treatments involving nephron-sparing surgery. In this context, PNs have a fundamental role, with a bigger emphasis being given to LPN, which, when performed by experienced hands, has given better results with respect to NPA in more recent studies. 19 We have classified the tumors in four categories: (0) <2 cm; (1) 2 to 4 cm; (3) 4 to 7 cm; (4) >7 cm, given the observation that patients with smaller tumors more frequently underwent PN.
The variable that describes the exophytic and endophytic characteristics of the renal tumor was used to describe the relation of the tumor with the surface of the kidney. This characteristic has been related to the complexity of the tumor and the risk of complications. 20 In the present study, 64% of patients with totally endophytic tumors underwent RN.
The longitudinal location has classified the renal masses in upper pole, mesorenal, and lower pole tumors. Upper pole tumors have been shown to be more complex and have been more frequently managed with RN vis-à-vis mesorenal and lower pole tumors.
The depth of tumor penetration has been well identified and described as an important variable that affects the facility of nephron-sparing surgery and the postsurgery complication rate. Some groups have noticed that the depth of the tumor affects the surgery decision taking process. 21,22 The extension of the compromised renal parenchyma has a high relation with the complexity of the tumor. This study has given weight to this variable because of its great importance regarding the decision to perform surgery and the potential complications. The logistical regression analysis revealed that the chance of a patient undergoing RN was 34 times greater in a patient with a tumor that extended beyond the renal medulla. This fact emphasizes the importance of such a variable in the surgery decision making process.
The relation of the tumor with the renal sinus has proven to be another variable in this research. Similarly, the extension of the compromised renal parenchyma variable has also been given weight because of its importance in the surgery decision taking process. Thus, 1 point has been attributed to tumors that do not attain the renal sinus, 2 points to tumors that reach the sinus peripherally, and 4 points to central tumors. This study has shown that the chance of a central tumor being managed with RN was 150 times greater in relation to other tumors.
The last variable of the score describes whether the tumor is anterior or posterior relative to its axial plan. Although there is no problem with open surgery, the anterior or posterior positioning of the tumor can affect laparoscopic or percutaneous procedures. 22,23 For posterior tumors, partial robotic or laparoscopy nephrectomy demands an extensive mobility, rotation of the kidney, or retroperitoneoscopy. 23 In a similar way, anterior tumors managed with radiofrequency or cryoablation may be difficult to reach because of the proximity of adjacent organs or with the need to pass by areas of the kidney that have not been affected. 22,24
By observing the results of this study, it is clear that both scores system (R.E.N.A.L. and SARR) were similar in predicting complications, margins status, or the surgery decision making process. The SARR score, however, is a simpler classification scheme, more intuitive, and more practical. No need to take millimeter measurements or make complicated calculations, making its use easier. The urologist can classify tumors only looking at a CT or MRI scan. These observations make the SARR a useful tool that can be used in clinical practice and not just in a research protocol.
Conclusion
The SARR score is a simple, practical, and intuitive renal tumor-classifying tool that can be used when planning a decision for surgery. It can also predict results and complications in the surgical treatment of patients with renal tumors.
Footnotes
Disclosure Statement
No competing financial interests exist.