
Abstract
Introduction:
Our objective was to determine the impact of race and tumor grade on perioperative leukocytosis on patients undergoing robot-assisted radical prostatectomy (RARP).
Methods:
A retrospective review of our urologic oncology database for patients undergoing RARP from August 2002 to July 2011 was conducted. A total of 768 patients were identified with complete data. Demographic data, preoperative prostate specific antigen (PSA), biopsy Gleason score, pathology Gleason score, pathology stage, margin status, and node status were collected. White blood cell (WBC) counts were captured preoperatively, 1 hour postoperatively, and on postoperative day 1. We assessed the differences in leukocyte responses according to the race and Gleason score using ANOVA testing.
Results:
Preoperative WBC was lowest in black men and comparable between white and Hispanic men. At 1 hour, postoperative WBC remained lowest in Black men (p<0.001). Post-RARP leukocytosis varied significantly depending on the race (p<0.001). At 1 hour, patients with Gleason 8–10 tumors had decreased WBC compared to Gleason 6 patients (p<0.05) despite similar preoperative WBC and Charlson comorbidity index values.
Conclusions:
We report novel clinical observations that suggest differences in the immune response associated with the race and Gleason grade following RARP. The clinical utility of these findings are yet to be determined.
Introduction
P
Racial and ethnic differences in peripheral white blood cell (WBC) counts have long been established at rest and following stressful stimuli such as strenuous aerobic exercises. 7 –11 Surgery, open or laparoscopic radical prostatectomy, is associated with postoperative leukocytosis host responses. A cytokine-induced inflammatory response is thought to mediate this postoperative leukocytosis. 12,13 Some investigators have noticed diminished cytokine responses following robot-assisted radical prostatectomy (RARP) or cystoprostatectomy compared to the open operation. 14 We sought to characterize perioperative leukocytosis following RARP and determine the association of race and ethnicity on host immune responses.
Materials and Methods
The Institutional Review Board approved the Columbia University Urologic Oncology Database, for patients with localized prostate cancer treated with RARP from August 2002 to July 2011, which was reviewed. In total, 1452 patients were identified who underwent RARP by five surgeons with varying levels of experience and training. We retrospectively identified 768 patients with WBC results obtained at three time points: 1–2 weeks preoperatively (preop), within 1 hour of the completion of surgery (postop#1) and on postoperative day 1 (postop#2). Racial identity was self-reported as black, white, or Hispanic-white. Patients whose racial identify is described as other included Far East and South Asians and those who did not describe themselves as a member of a particular racial group.
Clinical and pathological data, including the age, prostate specific antigen (PSA) level at diagnosis, biopsy Gleason score, clinical stage, pathological Gleason score, pathological stage, and surgical margin status, were all recorded. Prostate specimens were staged using the 2010 American Joint Committee on the Cancer TNM staging system. After prostatectomy, patients were evaluated with serial PSA tests, DREs, and imaging studies as deemed necessary.
Differences in the WBC response after RALP were analyzed according to the race and Gleason score using the Mann–Whitney and ANOVA statistical analysis. Spearman correlation coefficient was used to correlate the race with clinical factors (age, preoperative PSA, preoperative WBC, postoperative WBC#1, postoperative WBC#2, Charlson comorbidity index score, year of surgery, and surgeon) and pathologic variables (pathologic Gleason score, pathologic stage, surgical margin, and lymph node invasion status). A Cox proportional hazard model was used to identify the clinical and pathological variables that were independently predictive of the surgical margin status. All analyses were conducted using α=0.05 to determine the statistical significance.
Results
Between August 2002 and July 2011, a total of 1452 patients underwent RARP for clinically localized prostate cancer at our institution by five different surgeons. We were able to identify 768 patients who had complete WBC data for analysis. Four hundred three (52.5%) patients identified themselves as white, 155 (20.2%) were black, 91 (11.8%) were Hispanic, and 119 (15.5%) identified themselves as other. Baseline clinical and pathologic characteristics of cohorts are listed in Table 1. Whites were found to have significantly lower preoperative PSA values; however, the preoperative clinical stage was similar between all groups. With respect to pathologic Gleason score and stage, there was no significant difference between the groups. Blacks and Hispanics did have a significantly higher positive margin rate when compared to whites, and others. Charlson comorbidity index was similar throughout all groups.
PSA=prostate specific antigen.
In Figure 1, preoperative WBC was found to be lowest in black men, while whites and Hispanics had comparable levels. Black men also had the lowest 1 hour postoperative WBC (p<0.001). When stratified by the pathologic Gleason score, we found at 1 hour that patients with Gleason 8–10 tumors had decreased WBC compared to Gleason 6 and 7 patients despite having similar preoperative WBC and Charlson comorbidity index values. (Fig. 2) With respect to age, we found no association with WBC at any time point pre- or postoperatively (Fig. 3).
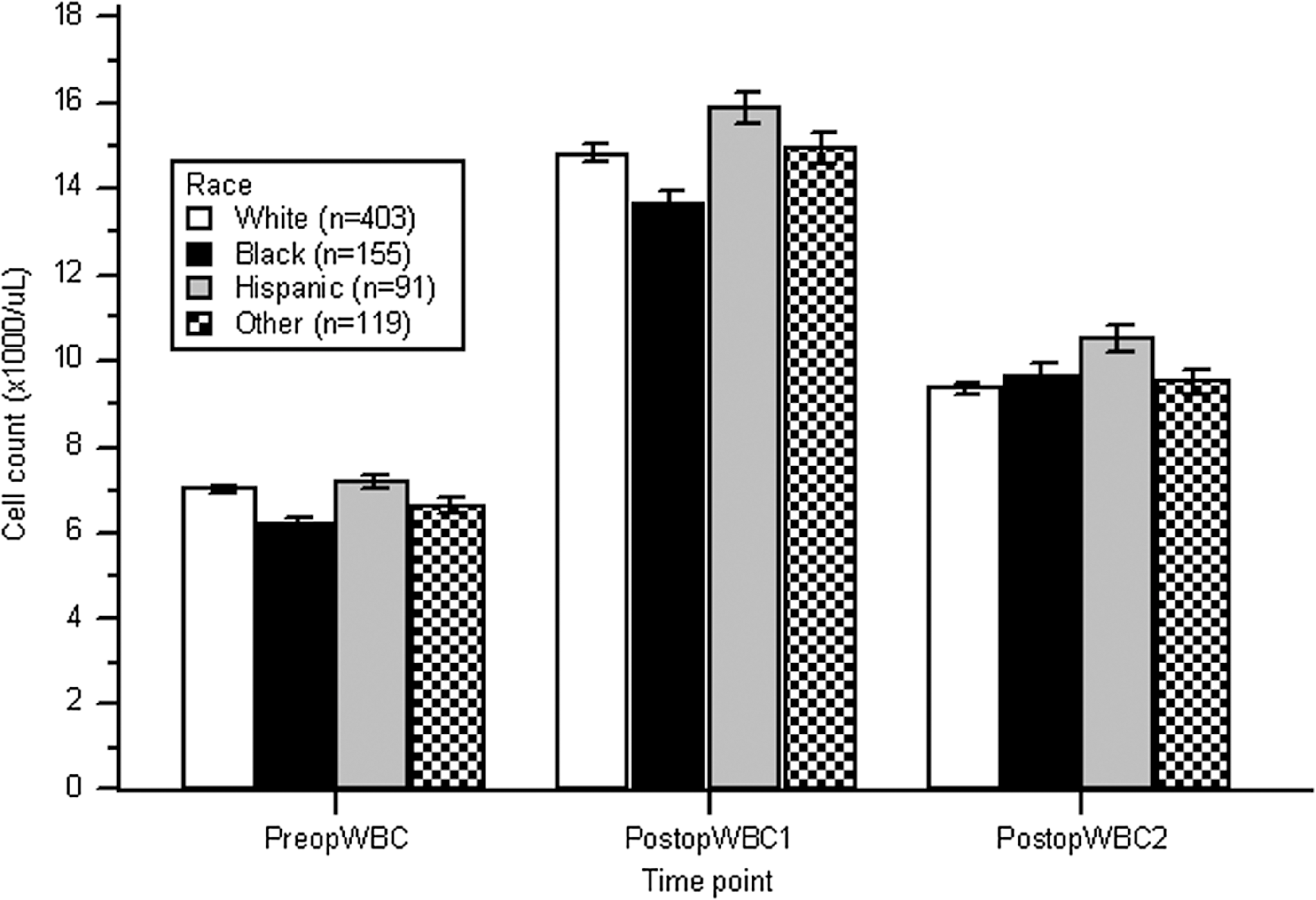
Racial differences in postrobotic prostatectomy peripheral leukocyte count white blood cell (WBC).
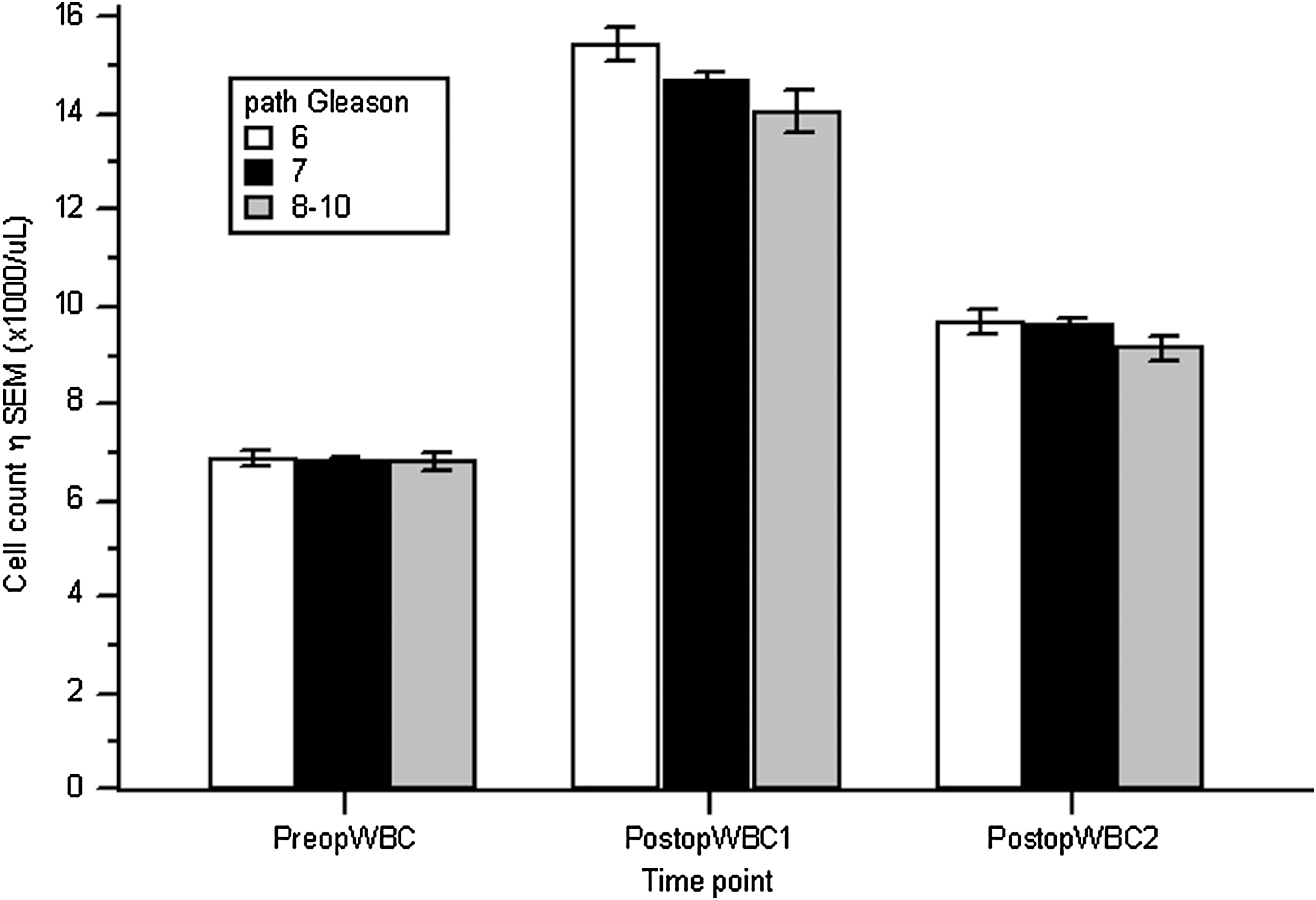
Comparison of postrobotic prostatectomy peripheral leukocyte count (WBC) by pathologic Gleason score.

Perioperative leukocyte counts (WBC) according to age.
Discussion
In the United States, black men have not only the highest risk developing prostate cancer with an annual incidence of 178/100,000, they also suffer from a high risk of prostate cancer mortality. 1,3 –5 These disparities in outcomes have been attributed to multiple theories, including socioeconomic status, access to healthcare, treatment choice, and tumor biology. 4,5 Identifying potential contributing factors that explain such disparities with prostate cancer can help discover other avenues for treatment and ultimately prevention. We report novel clinical observations that suggest differences in immune responses associated with race and Gleason grade following RALP. Black men undergoing RALP had lower preoperative and immediate postoperative WBC counts as compared to other racial groups. In addition, we saw a significant trend toward lower WBC in patients with higher grade tumors (Gleason 8–10). Our results suggest there is a potential immunologic role that may contribute to the racial differences associated with prostate cancer outcomes.
The inverse relationship between neutrophil activity and the presence of cancer is well documented. 15 Defects in the neutrophil cytotoxic oxidative metabolism have been found with increased incidence in patients with lung cancer 16 and other solid organ diseases. 15 Similarly, the associations between defective leukocyte chemotaxis and motility and melanoma, 17 breast cancer, 18 and colon cancer 19 have been demonstrated. Furthermore, there has long been evidence that cancer tumors produce factors that inhibit neutrophil function. Serum from patients with cancer has been shown to inhibit neutrophil chemotaxis 20 and phagocytosis. 21 Which of these processes has a larger contribution to the development of malignancies is unknown. Whether it is an inherent defect in neutrophil cytotoxicity allowing malignancies to develop or rather the cancers' ability to impair neutrophils that is primarily responsible for carcinogenesis has yet to be determined. It is clear that neutrophils play a role in the destruction of cancer cells.
The neutrophil activity has been shown to be a prognostic indicator for prostate cancer. Neutropenia (neutrophil count of >1500/mL) in African American men carries an elevated risk of having poorly differentiated prostate cancer. 22 Neutrophil infiltration on prostate biopsy correlates inversely with the presence of malignancy 20 and an elevated serum neutrophil count is associated with decreased likelihood of positive prostate biopsy. 23 Our results, along with the abovementioned evidence, suggest that there may be an immunologic component as to why black men are at greater risk from prostate cancer than other racial groups.
Investigation of immunologic treatments for urologic malignancies has confirmed the association of activation of the innate immune system and cancer abatement. Intravesical Bacille Calmette–Guerin (BCG) has been a validated treatment for superficial bladder cancer since 1976. 24 Studies have correlated successful BCG treatment with neutrophil activation, migration, and presence in urine. 25,26 More recently in 2010, the FDA approved Sipuleucel-T as a therapeutic cancer vaccine for patients with hormone refractory metastatic prostate cancer. Sipuleucel-T involves exposing a patient's own antigen presenting cells to a fusion protein, including prostatic acid phosphatase and granulocyte-macrophage colony stimulating factor ex vivo, and then infusing these cells back into the patient. In the phase III study, Sipuleucel-T was able to extend survival by a median of 4.1 months. 27 These results further corroborate the role of our innate immune system with that of potential cancer control.
There are several limitations of this study that must be considered, including its retrospective study design. We lack long-term disease-specific recurrence and mortality data, which could help elucidate whether WBC levels correlate worse disease-specific outcomes in different racial groups. We also acknowledge the possibility of racial misclassification since this was self-reported by patients without validation.
Conclusions
The WBC level is a routine test that is easily performed and interpreted. Our findings suggest a relationship between the race and tumor grade with leukocystosis in men undergoing RARP. Further investigations are necessary, particularly determination of an associative versus causative relationship. As such, the clinical utility of these findings remains to be determined.
Footnotes
Author Disclosure Statement
No competing financial interests exist.