
Abstract
Background and Purpose:
The energy source used for stone fragmentation is important in miniperc. In this study, we compared the stone fragmentation characteristics and outcomes of laser lithotripsy and pneumatic lithotripsy in miniperc for renal calculi.
Patients and Methods:
After Institutional Review Board approval, 60 patients undergoing miniperc for renal calculi of 15 to 30 mm were equally randomized to laser and pneumatic lithotripsy groups. Miniperc was performed using 16.5F Karl Storz miniperc sheath and a 12F nephroscope. Laser lithotripsy was performed using a 550-μm laser fiber and 30 W laser with variable settings according to the need. Pneumatic lithotripsy was performed using the EMS Swiss lithoclast. Patient demographics, stone characteristics, intraoperative parameters, and postoperative outcomes were analyzed.
Results:
The baseline patient demographics and stone characteristics were similar in both groups. The total operative time (P=0.433) and fragmentation time (P=0.101) were similar between the groups. The surgeon assessed that the Likert score (1 to 5) for fragmentation was similar in both groups (2.1±0.8 vs 1.9±0.9, P=0.313). Stone migration was lower with the laser (1.3±0.5 vs 1.7±0.8, P=0.043), and fragment removal was easier with the laser (1.1±0.3 vs 1.7±1.1, P=0.011). The need for fragment retrieval using a basket was significantly more in the pneumatic lithotripsy group (10% vs 37%, P=0.002). The hemoglobin drop, complication rates, auxiliary procedures, postoperative pain, and stone clearance rates were similar between the groups (P>0.2).
Conclusion:
Both laser lithotripsy and pneumatic lithotripsy are equally safe and efficient stone fragmentation modalities in miniperc. Laser lithotripsy is associated with lower stone migration and easier retrieval of the smaller fragments it produces.
Introduction
P
The beneficial role of miniperc has been established in large series. 6 The technique of miniperc relies mainly on stone fragmentation and its removal by saline irrigation. Thus, the energy source used for stone fragmentation is an important aspect in miniperc. The optimal energy source to be used in miniperc, however, has not been prospectively evaluated so far. In this study, we compared laser with pneumatic lithotripsy to assess the relative merits and disadvantages.
Patients and Methods
This study was conducted in a tertiary care urology hospital in Western India. After Institutional Review Board and ethics committee approval, patients undergoing miniperc for renal calculi between 1.5 cm and 2.5 cm in our institution from December 2011 to January 2013 were equally randomized into laser and pneumatic lithotripsy groups (Fig. 1). Informed consent was obtained from each patient included in the study. Randomization was performed using computer generated numbers in blocks of five. Randomization was performed centrally and conveyed to the operating surgeon before the start of the procedure. Patients having active urinary tract infection, coagulopathy, pregnancy, anomalous kidney, or renal calculi that required more than one puncture were excluded from the study.

Consort flow diagram.
All procedures were performed under general anesthesia. With the patient in the lithotomy position, ureteral catheterization was performed using a 5F ureteral catheter under cystoscopic guidance. With the patient in the prone position, ultrasonography guided caliceal puncture was made, and a glidewire (Terumo, Tokyo, Japan) was passed into the pelvicaliceal system after confirmation of proper access under fluoroscopy. Tract dilation was performed over the glidewire using a 14F screw dilator, followed by insertion of the obturator and sheath of the 16.5F miniperc system (Karl Storz, Tuttlingen, Germany) (Fig. 2).
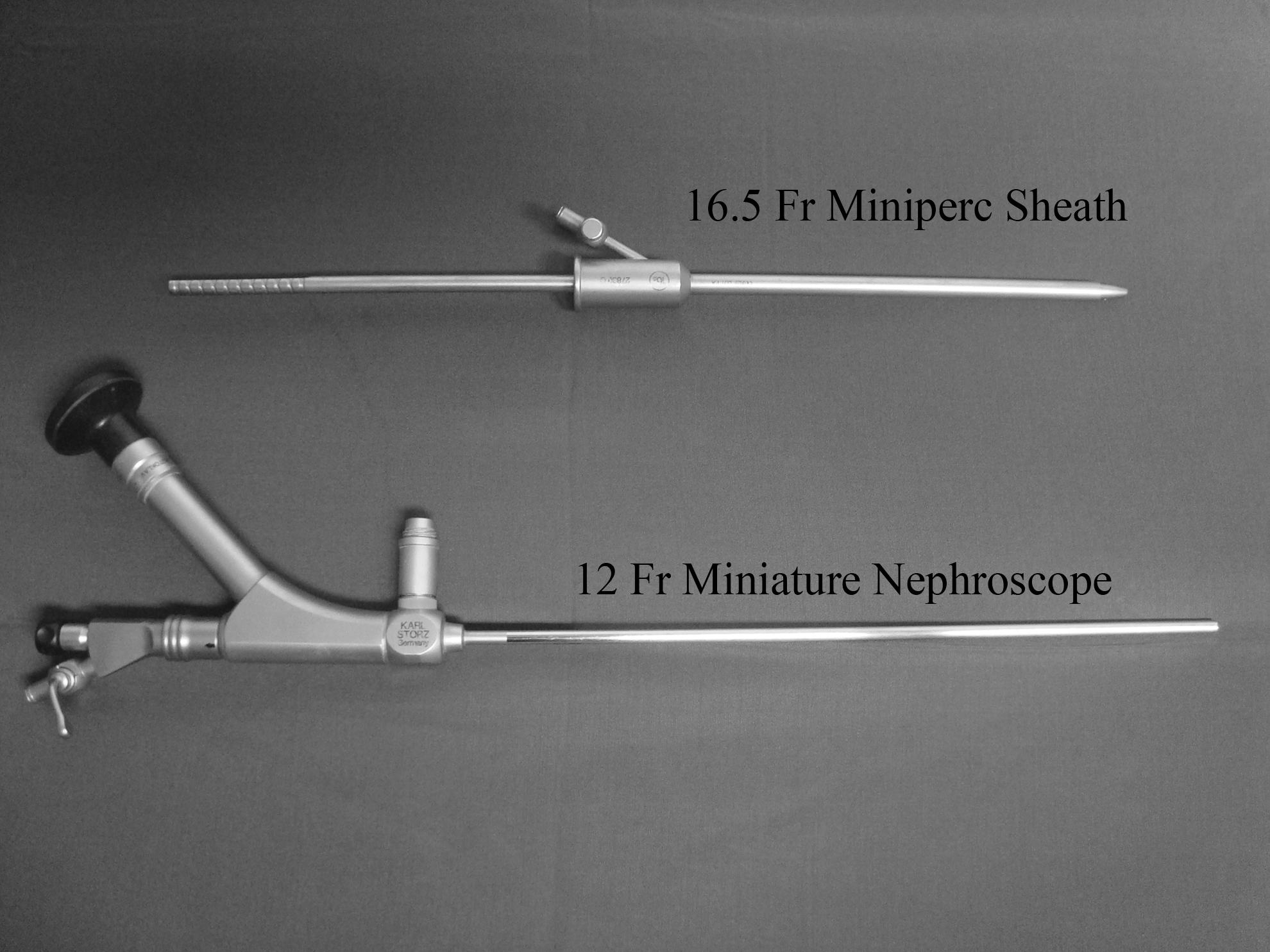
Instruments used for miniperc.
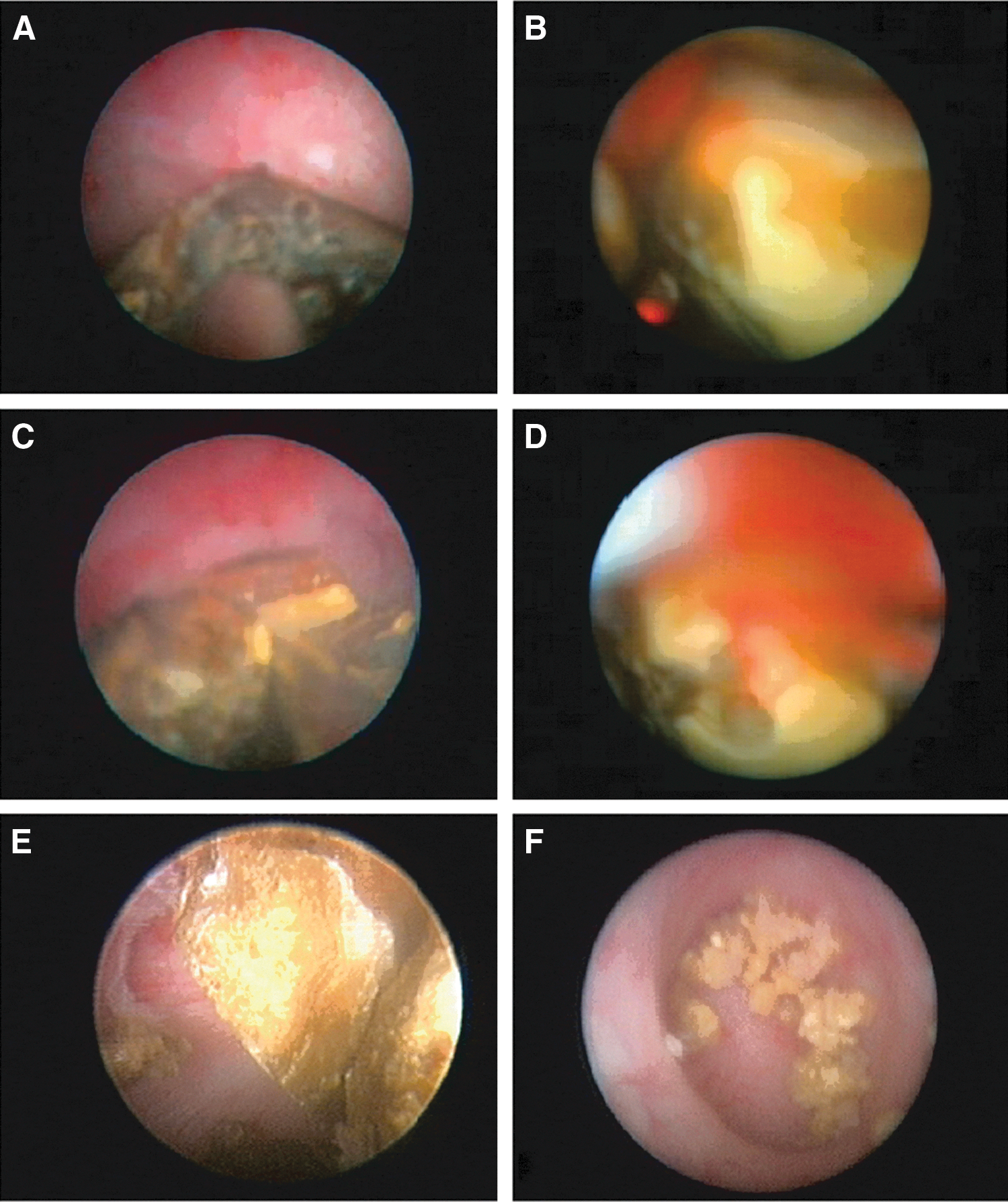
Using a 12F miniature Storz nephroscope that has a 6F channel, stone fragmentation was performed with either holmium:yttrium-aluminum-garnet (Ho:YAG) laser 30 W (LISA Sphinx, LISA laser USA, Pleasonton, CA) or pneumatic lithotripter (Swiss lithoclast,® EMS Medical Systems, Nyon, Switzerland) as per randomization (Figs. 3A–F). The laser fiber used was 550 μm, with energy of 0.5 to 1.5 J and frequency of 6 to 20 Hz. Laser fragmentation was started using low energy with high frequency and changed to high energy with low frequency for final fragmentation. Pneumatic lithotripsy was performed using a 1.0 mm lithoclast probe in single pulse mode. Stone fragments were flushed out of the kidney through the miniperc sheath with saline irrigation from the nephroscope or, if required, from the ureteral catheter. Those fragments that could not be flushed were retrieved using a nitinol basket. Intraoperative stone clearance was confirmed using nephroscopy and fluoroscopy.
Insertion of a Double-J stent or nephrostomy tube was left to the discretion of the surgeon as per the merit of the individual case. A perurethral catheter along with a ureteral catheter (if present) was removed on the first postoperative day. Patients were discharged on the first postoperative day if there was no complication.
The primary outcome was total operative time. Secondary outcomes studied were stone fragmentation time, surgeon assessed Likert scores for ease of stone fragmentation, stone migration and retrieval, need for basket to retrieve stone fragments, intraoperative and postoperative complications (according to the Clavien-Dindo classification), 7 hemoglobin drop, auxiliary procedures, postoperative pain score, analgesic requirement, hospital stay, and stone clearance on fthe irst postoperative day and 1 month follow-up. The operating surgeon noted Likert scores for stone fragmentation, migration, and retrieval at the end of the procedure. At postoperative day 1 and at 1-month follow-up, stone clearance was assessed by radiography of the kidneys, ureters, and bladder (KUB) and ultrasonographic KUB.
The sample size of 60 patients was calculated using a sample size calculator to detect a mean difference in total operative time of 15 minutes between the two groups, with a power of 0.8 and alpha value of 0.05. All data were prospectively entered in Excel sheets. Discrete categorical data were expressed as number and percentage. Continuous data were expressed as mean±standard deviation. Categorical variables were analyzed using the Pearson chi-square test or the Fisher exact test. Continuous variables were compared between the two groups using independent samples Student t test or Mann-Whitney U test. A P value<0.05 was considered as significant.
Results
The baseline patient demographics and stone characteristics were similar in both the groups (Table 1). The total operative time (P=0.433) and fragmentation time (P=0.101) were similar between the groups. In the pneumatic lithotripsy group, significantly more patients needed the use of a basket or forceps to retrieve stone fragments (37% vs 10%, P=0.002). Among the surgeon Likert scores, ease of fragmentation was similar with both modalities (P=0.313), while there was higher stone migration (P=0.043) and more difficulty in fragment retrieval (0.011) in the pneumatic lithotripsy group (Table 2). Complication rate, postoperative pain scores, analgesic requirement, need for auxiliary procedures, and stone clearance rates were similar in both groups (P>0.2) (Table 3).
Values are expressed as mean±standard deviation.
In case of multiple calculi, the site of the largest calculus has been provided.
SD=standard deviation.
VAS=visual analog scale.
Discussion
In standard PCNL, blood loss increases with an increase in the size of the tract. 8 In the recent Clinical Research Office of the Endourological Society Percutaneous Nephrolithotomy Global Study, sheath size was associated with increased transfusion rates (P<0.0001), with transfusion rates of 1.1% for the smallest sheath (<18F) and 12.0% for the largest sheath (≥32F). 9 In view of these advantages and with the availability of smaller custom-made instruments, miniperc has been widely used to manage renal calculi in all age groups. For the management of small renal calculi, miniperc provides a safe and effective alternative to RIRS. 10 Multitract miniperc has been used to manage even staghorn calculi. 11
The commonly used modalities to fragment calculi in miniperc are laser and pneumatic lithotripters. Choosing the appropriate lithotripter is important because operative time in miniperc has been shown to be prolonged because of smaller instruments and sheath size. 12 Moreover, because most of the stone fragments get flushed out along with saline irrigation, proper fragmentation of calculi is important for the success of the procedure. In this study, the total operative time and fragmentation time were similar in both laser and pneumatic lithotripsy groups. In pneumatic lithotripsy, initial fragmentation was rapid. Further fragmentation of the fragments, however, was difficult and time consuming. In laser lithotripsy, the fragmentation rate was nearly uniform throughout the procedure and was efficient for both the whole calculus and smaller fragments. In laser, initial dusting could be performed using the low energy and high frequency setting. As the size of stone decreased, the settings could be changed to high energy and low frequency to individually break the remaining larger fragments. This ability to alter the settings to optimize the fragmentation and reduce migration was an important advantage of laser lithotripsy.
Stone migration is an important issue in PCNL. In this study, laser lithotripsy lead to lower stone migration than pneumatic lithotripsy. Stone migration has been shown to be lower with laser lithotripsy in ureteroscopy. 13 Because the mechanism of action of the Ho:YAG laser involves more photothermal effect than a photoacoustic effect, stone migration was lower. 14 This advantage was better appreciated as the calculi were broken into smaller fragments. With pneumatic lithotripsy, stone migration increased as the size of fragments decreased, while laser was still efficient for dusting the smaller stone fragments. If a lower caliceal access is obtained, as is commonly performed, retrieval of stone fragments migrated into upper and middle calices using a rigid nephroscope may be difficult, especially in obese patients and those with low-lying kidneys because of hindrance from the iliac crest. 15 This can lead to significant torque in the renal parenchyma with potential for infundibular tear and bleeding. Moreover, small fragments may unknowingly migrate to inaccessible calices. This may require the use of flexible instruments or even another tract for clearance of stone.
Because the caliber of miniperc sheaths is narrow, they allow flexible ureteroscopes but not flexible nephroscopes. Using a flexible ureteroscope antegradely has the disadvantages of poor vision and difficulty in maneuvering. 15 These additional procedures add to the cost and morbidity of the procedure. In addition, if these fragments are not visible on fluoroscopy, incomplete stone clearance results. In this regard, routine use of flexible nephroscopy has been shown to reduce the incidence of residual calculi. 16 Various devices such as Stone Cone™ 17 and the Accordion® stone management device 18 have been developed to prevent stone migration into the ureter. These devices are not used routinely, however, and they do not prevent migration into inaccessible calices.
In the pneumatic lithotripsy group, stone retrieval was relatively difficult and needed the use of a basket more frequently. We used single pulse mode in pneumatic lithotripsy, because it has been shown that multiple pulse mode leads to longer operative time and more residual calculi. 19 In addition to the higher stone migration in the pneumatic lithotripsy group, the size of fragments created in that group was larger when compared with those of laser lithotripsy (Fig. 4A, 4B). Ho:YAG laser lithotripsy produces significantly smaller fragments compared with those of pneumatic lithotripsy. 20 These were probably the reasons for difficulty in retrieving stone fragments in the pneumatic lithotripsy group. When compared with pneumatic lithotripsy, laser lithotripsy produced more fine sand-like debris (Fig 4C). Carr and associates 21 showed that the rate of stone formation within 1 year was significantly higher after SWL compared with PCNL. While the location of stone recurrences in the SWL group shifted to mid and lower calices, a similar trend was not seen in PCNL. 21 Thus, it was suggested that the stone debris left behind in SWL led to an increased chance of recurrent stone formation. 21 It remains to be seen whether the fine stone debris produced by laser lithotripsy leads to a higher risk of stone recurrence.

The complication rates in both the groups were similar and low. This was probably because of the relatively smaller bulk of renal calculi included in this study and the relative safety of miniperc. The postoperative pain scores and analgesic requirements in both the groups were similar. Thus, the type of energy source used did not have an influence on postoperative pain. The stone clearance rates were apparently similar in both the groups. In ureteroscopy for distal ureteral calculi, a recent meta-analysis showed that laser lithotripsy had a better stone clearance rate. 13 This was probably the result of lower stone migration associated with laser lithotripsy.
One limitation of our study was that it was not adequately powered to detect a small change in stone clearance rates between the two modalities. This was not the primary objective of the present study, however, and our data did not suggest any trend toward a clinically significant difference between the two groups regarding stone clearance. Another potential limitation was the lack of use of a CT scan for assessing residual calculi. This was not performed because ofeconomic and radiation hazard considerations.
Conclusions
Both laser and pneumatic lithotripsy are equally safe and efficient stone fragmentation modalities in miniperc. Laser lithotripsy is associated with lower stone migration and easier retrieval of the smaller fragments it produces.
Footnotes
Disclosure Statement
No competing financial interests exist.