
Abstract
Background and Purpose:
The effectiveness of locoregional hyperthermia combined with intravesical instillation of mitomycin C to reduce the risk of recurrence and progression of intermediate- and high-risk nonmuscle-invasive bladder cancer is currently investigated in clinical trials. Clinically effective locoregional hyperthermia delivery necessitates adequate thermal dosimetry; thus, optimal thermometry methods are needed to monitor accurately the temperature distribution throughout the bladder wall. The aim of the study was to evaluate the technical feasibility of a novel intravesical device (multi-sensor probe) developed to monitor the local bladder wall temperatures during loco-regional C-HT.
Materials and Methods:
A multisensor thermocouple probe was designed for deployment in the human bladder, using special sensors to cover the bladder wall in different directions. The deployment of the thermocouples against the bladder wall was evaluated with visual, endoscopic, and CT imaging in bladder phantoms, porcine models, and human bladders obtained from obduction for bladder volumes and different deployment sizes of the probe. Finally, porcine bladders were embedded in a phantom and subjected to locoregional heating to compare probe temperatures with additional thermometry inside and outside the bladder wall.
Results:
The 7.5 cm thermocouple probe yielded optimal bladder wall contact, adapting to different bladder volumes. Temperature monitoring was shown to be accurate and representative for the actual bladder wall temperature.
Conclusions:
Use of this novel multisensor probe could yield a more accurate monitoring of the bladder wall temperature during locoregional chemohyperthermia.
Introduction
T
Transurethral resection of bladder tumors remains the gold standard for the initial treatment of patients with NMIBC, but the high rates of recurrence and significant risk of progression to higher grade tumors mandate additional adjuvant therapies. 2,3 A wide variety of drugs has been administered intravesically over the years with prophylactic intent. To date, bacillus Calmette-Guérin immunotherapy and mitomycin C (MMC) chemotherapy are considered standard intravesical treatments. Undesirable toxicities and suboptimal efficacy, however, resulted in the search for novel therapeutic strategies such as device-assisted drug administration. 4,5
Device-assisted strategies for intermediate- and high-risk groups include: Photodynamic therapy, electromotive drug administration, and the combination of intravesical hyperthermia (HT) and chemotherapy (C). 6 The latter, referred to as chemohyperthermia (C-HT) (MMC/hyperthermia), has proven to be more effective than MMC alone for patients with T a-1 G1–3 NMIBC in comparative studies with ablative 7 as well as prophylactic intent, 8 and promising results are continuously emerging. 9
To date, the most common form of C-HT uses intracavitary heating (Synergo®), in which HT is administered via local microwave irradiation of the urothelium by means of a 915-MHz intravesical microwave applicator. 6 Locoregional HT has been proposed as an alternative to intracavitary HT techniques, because locoregional HT is expected to yield a more uniform bladder wall temperature distribution, which may be monitored for further optimization of HT delivery. To this end, a novel multisensor probe was developed for more accurate monitoring of the bladder temperature during locoregional C-HT. We describe and evaluate the technical feasibility test of this intravesical device during development required before clinical use during locoregional C-HT treatment.
Materials and Methods
Study design
A research project funded by the Dutch Cancer Society (UVA 2012 5539: Optimization of bladder hyperthermia treatment for NMIBC by using locoregional heating, improved thermometry and 3D hyperthermia planning) was designed in collaboration with the urology and radiation oncology departments at our institute. In summary, locoregional HT (heating of the bladder and surrounding tissue) is performed to achieve intravesical temperatures of about 41°C–44°C, while three-dimensional (3D) steering of the temperature rise is used, guided by high resolution hyperthermia treatment planning (HTP) and improved by 3D temperature data, obtained by developing a new probe to monitor the bladder wall temperature distribution.
The first stage of our study and the purpose of this article is the development of a multisensor thermometry probe capable of: (1) Instilling the bladder with MMC; (2) inflating a balloon for fixation; and (3) unfolding multiple thermocouples for accurate measurement of the bladder wall temperature at different locations. The first two functions each needed one separate lumen. The third function needed a system capable of unfolding multiple thermocouples to measure the temperature at the bladder wall.
A number of options were considered. One option was to use the Colombo and van der Heijden designs for intracavitary HT, in which balloons were used to press three or five separate single point thermometry probes to the bladder wall. 10,11 Another option was to create a loop or umbrella capable of unfolding into the bladder cavity. Advantages of this design were the distribution of measurement points over the entire bladder wall, not disturbed by temperature gradients within the bladder because of the alignment with the bladder wall. Development of this multisensor unfolding thermometry probe was performed in collaboration with Ella-CS™ (Czech Republic), and the main challenge was to design a system that would always unfold properly and reproducibly against the bladder wall. In addition, the thermometry points should always be in good contact with the bladder wall for the effective clinical range of bladder volumes, which is limited because the bladder is filled with a distinct quantity of fluid during HT plus MMC.
After evaluation of the advantages and disadvantages of loop vs umbrella probes, an umbrella-like multisensor probe was further developed, consisting of seven thermocouples integrated in an 18F open-end catheter. Five of seven thermocouples that extend against the bladder wall when deployed were mounted on the arms of the umbrella; the remaining two thermocouples provide intralumenal measurements at two different locations along the central axis of the bladder.
Three different sizes were tested with a deployment radius of the thermocouples of 5 cm, 7.5 cm, and 10 cm (Fig. 1). These prototypes were tested in three stages: (1) The first stage involved phantom tests using cavities of different shapes and sizes to visually verify that all measurement points stayed in contact with the inner cavity wall under all circumstances; (2) the second stage involved animal testing using porcine models, in which the probe's deployment into the pig's bladder was assessed in situ. For this purpose, probes integrated into an 18F open-end catheter were introduced into the bladder of female pigs in a transvaginal fashion, by perforating the vesicovaginal septum, thus reproducing transurethral use in humans. Simultaneously, a laparoscopic endoscope was inserted through the bladder dome to monitor on video how the thermocouples deployed into the cavity against the bladder wall. The same procedure was reproduced using human bladders obtained from obduction, in accordance to the local ethics committee.

Umbrella-like (deployed) multisensor probe integrated in an 18F open-end catheter. Multisensor probes were of different sizes (5, 7.5 and 10 cm) according to the deployment radius of thermocouples.
(3) CT and thermal verification of the position of the thermocouples with respect to the bladder wall were performed by using porcine bladder models embedded in a saline-filled pelvis-sized phantom heated with the AMC locoregional HT device. 12 The 0.3% saline in the phantom has the properties of a realistic muscle-fat mixture at the 70 MHz frequency of the HT device. The bladder was filled with 60, 120, and 180 mL 0.9% saline resulting in higher power absorption than in the surrounding phantom material. The phantom was placed in the AMC HT device and exposed to 400 W for 15 minutes.
The temperature rise inside the bladder was recorded with the deployed umbrella probe. The temperatures recorded by the five thermocouples mounted on the arms of the umbrella were compared with independent thermometry at the exterior of the bladder wall. The temperature rise at the center of the bladder was recorded with two thermocouples providing intralumenal measurements along the central bladder axis.
Results
Tests using cavities of different shapes and sizes demonstrated that all measurement points stayed in contact with the inner cavity wall under all circumstances (Fig. 2). In the second stage, all probe sizes were successively evaluated in terms of deployment features and interaction with the bladder wall (mucosa) at different bladder volumes in pig bladders in situ. The 7.5 cm radius thermocouple probe yielded optimal bladder wall contact, adapting to different realistic filling volumes of 60, 120 and 180 mL during actual intravesical treatment (Fig. 3). CT verification in the pelvis-sized phantom confirmed the position of the thermocouples with respect to the bladder wall (Figs. 4 and 5).

Deployment of 5 cm radius thermocouples in a bladder phantom.

Endoscopic vision shows deployment of thermocouples into the human bladder cavity.
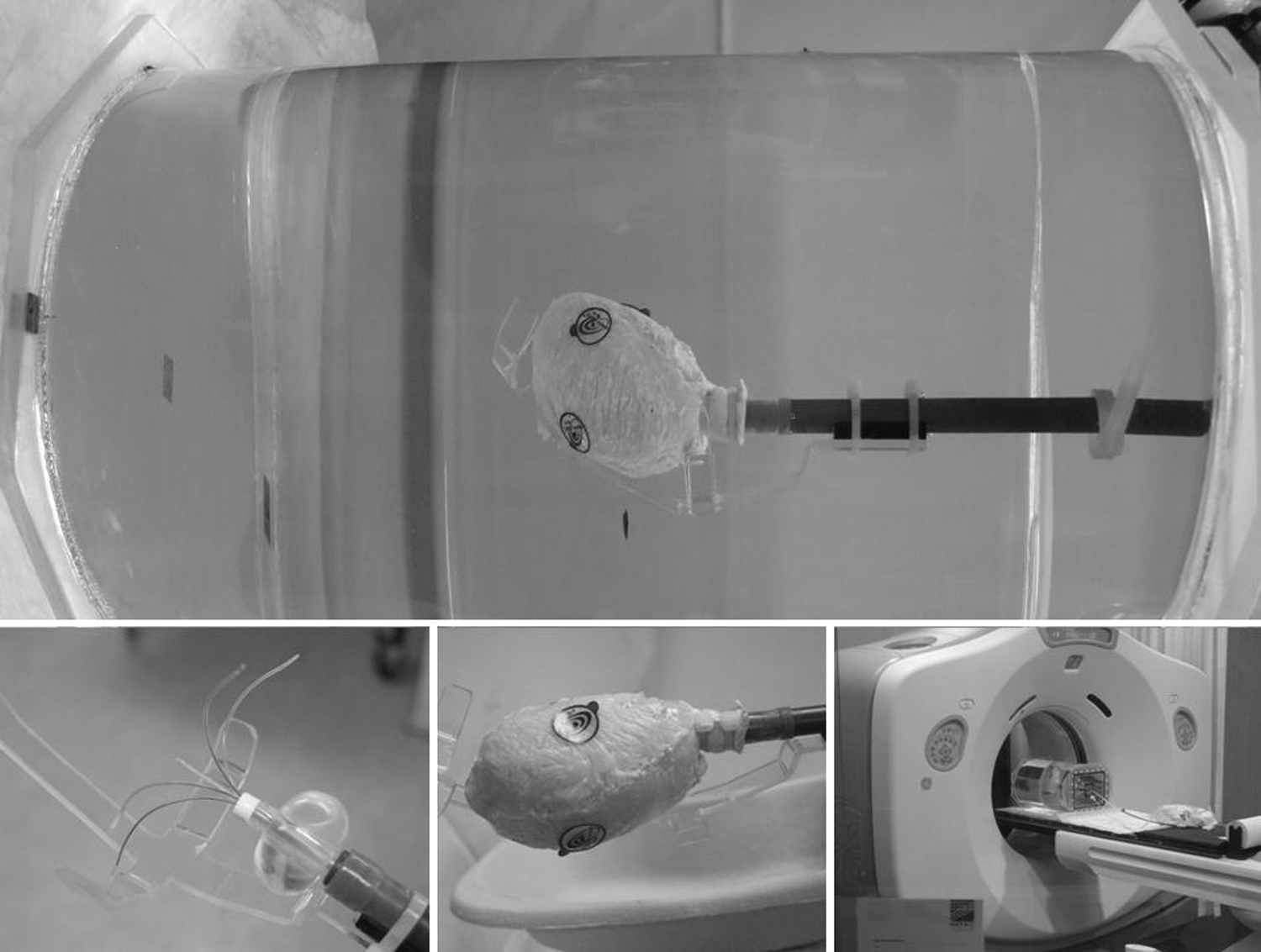
Porcine bladder embedded in a saline-filled phantom (40×35×27 cm) (top). Detail of the components and placement of the phantom on the CT scan (bottom).
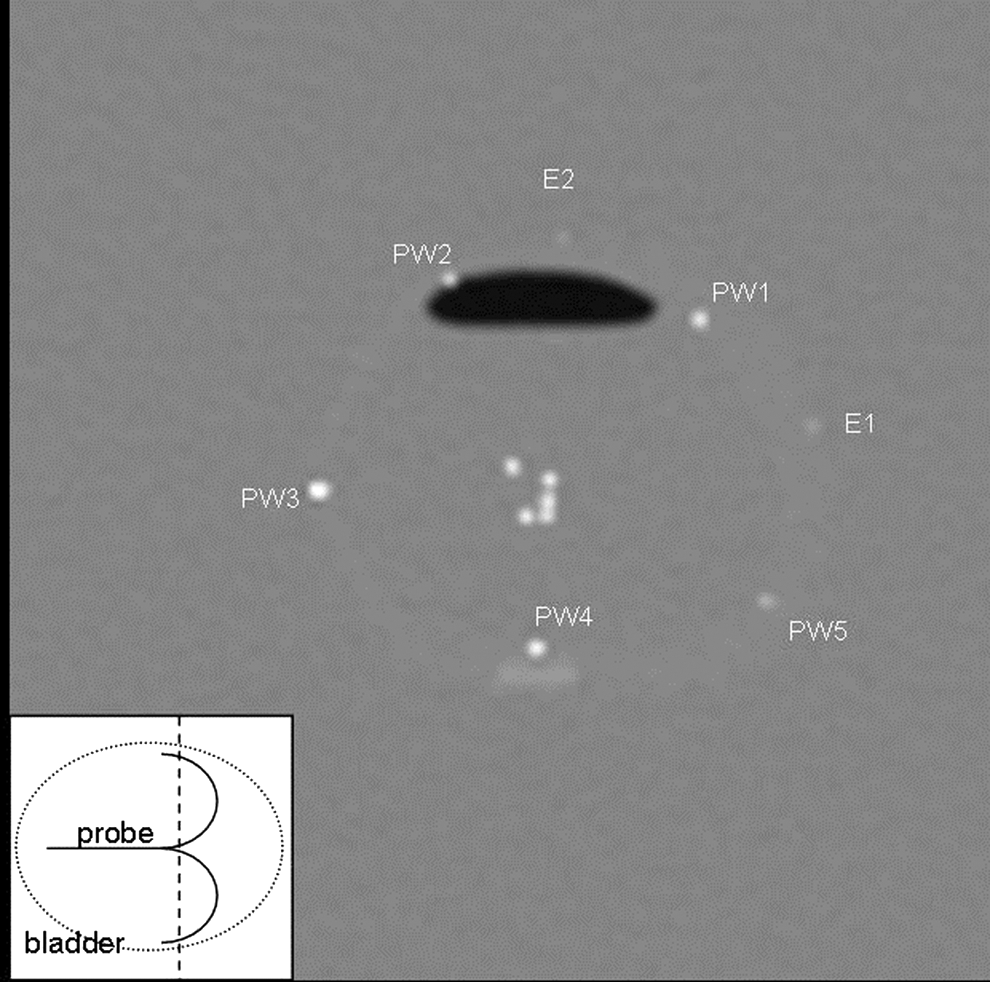
CT scan of the deployed 7.5 cm probe in the bladder filled with 180 mL in saline-filled phantom. Transversal slice along dotted line showing thermocouple sensors PW1–PW5 and E1–E2 (see also Fig. 6). Note small air pocket in the top of the bladder. PW=probe thermocouple at wall; E1=thermocouple outside bladder; E2=thermocouple outside bladder.
The heating test demonstrated that the deployed 7.5 cm umbrella thermocouples showed excellent alignment and that the temperature rise recorded inside the bladder matched the measurements with the additional thermocouples mounted on the exterior bladder wall for 60, 120, and 180 mL bladder volumes. The temperature rise recorded at the center of the bladder exceeded the temperature rise measured at the inner and outside bladder wall, and this was reliably recorded by the probe (Figs. 6 and 7).
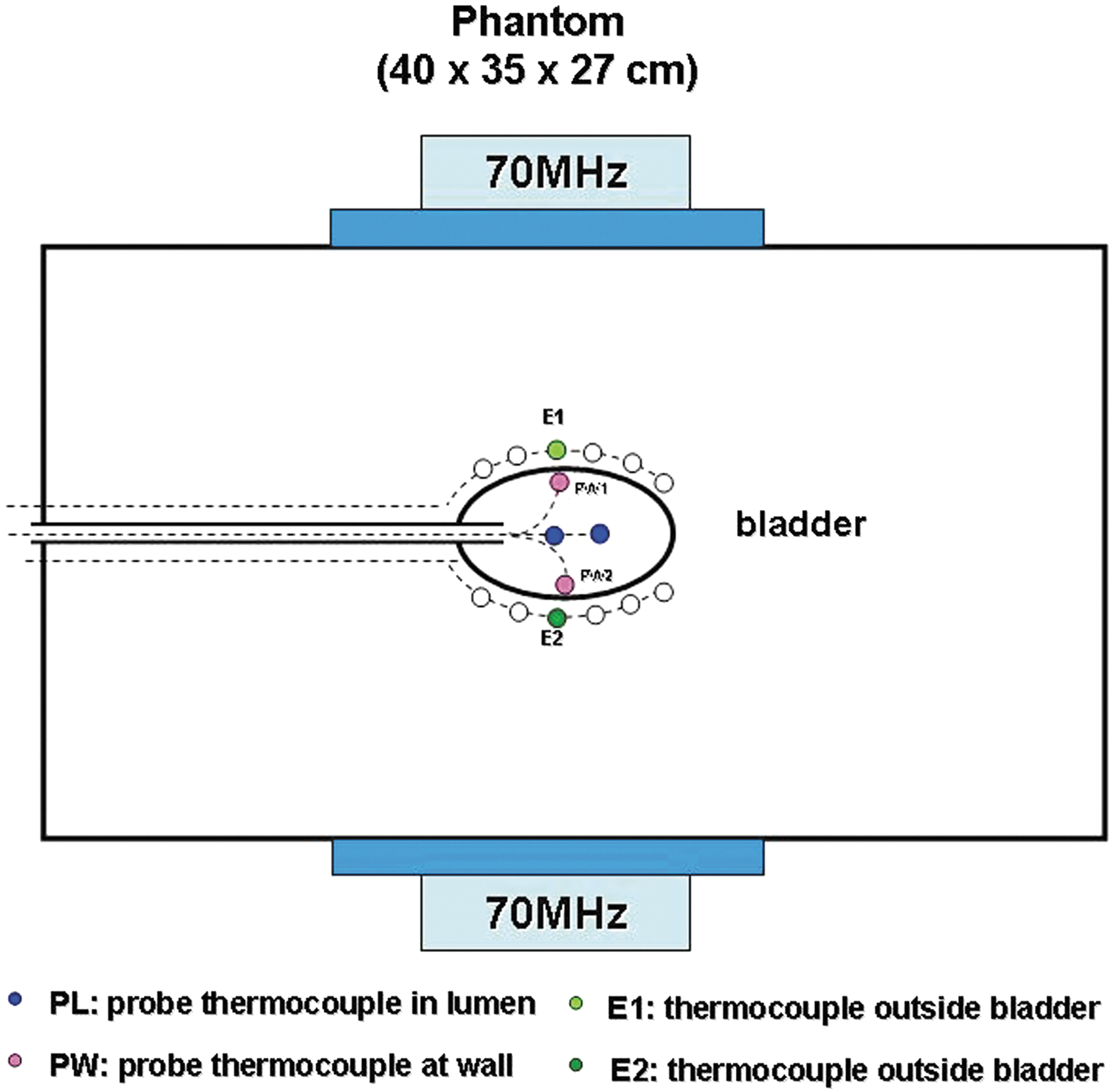
Schematic drawing of the phantom's setup and the position of thermometry probes.
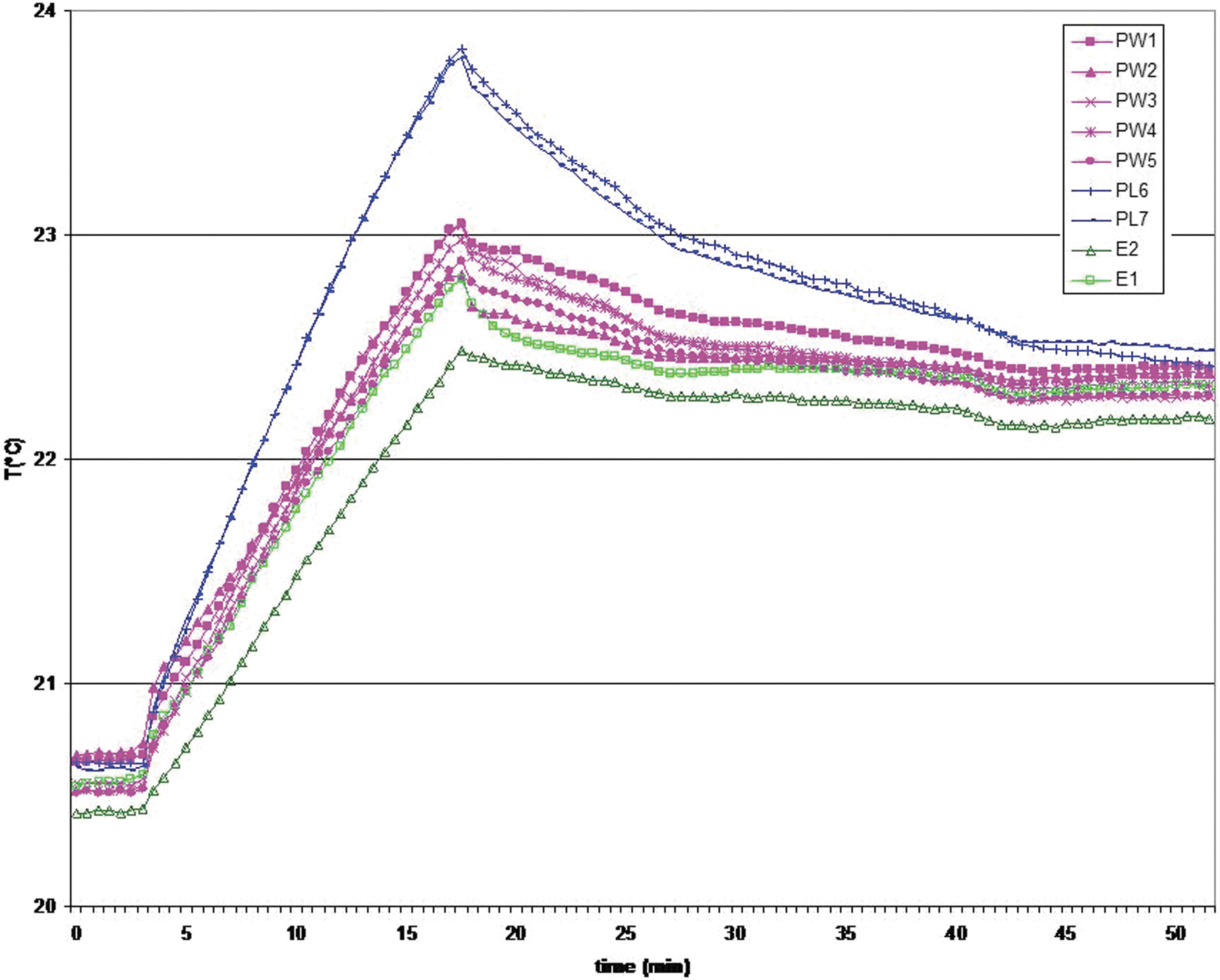
This graph shows identical measurements between the PW1 and PW2 (internal bladder wall) and E1 and E2 (external) thermocouples. Bladder filled with 180 mL saline. Heating with AMC locoregional hyperthermia device between t=3 and t=18 minutes (400 W). The probe thermocouples in the lumen (PL) show a much higher temperature rise because more power is dissipated inside the bladder than in the surrounding phantom.
Discussion
Since the studies of Rigatti and associates, 13 who first combined intravesical MMC with intracavitary 915 MHz microwave HT to reduce recurrence and progression, the combined regimen has been tested in different clinical settings for almost two decades. 6 –8,10,11,14 –18 Two different bladder-heating techniques have been applied: (1) Intracavitary microwave HT in the treatment of NMIBC; and (2) locoregional HT for muscle-invasive bladder cancer. Intracavitary heating techniques have disadvantages in comparison with locoregional HT: In particular, greater temperature differences in the bladder wall because the spatial power distribution of an intracavitary microwave antenna is not evenly distributed over the surface of the bladder wall, and a single antenna offers no option to modify the power distribution. Achieving a good thermal dose over the entire bladder wall can thus easily result in overheating of parts of the bladder wall, resulting in pain and toxicity. 8 The newly developed thermometry probe would be helpful in preventing both underdosage and overheating because it provides extensive and accurate temperature data across the bladder wall.
Locoregional HT given with an array of antennas results in a temperature rise in a large pelvic volume with the option of 3D spatial steering of the power distribution and is therefore expected to yield a better controlled and more uniform temperature distribution in the bladder wall. 12 Thermometry in locoregional HT treatments is usually limited to intravesical measurements for the bladder and intralumenal measurements in the rectum and vagina to avoid implant risks. 19,20 Thus, also for this treatment modality, the newly developed thermometry probe would be of great help. In addition, HTP software has been introduced to compute optimal antenna settings before treatment. 21,22 Clinical application of HTP and optimization has proven to be a promising technique. 23
Conclusions
This novel multisensor probe yields a more accurate monitoring of the bladder wall temperature during locoregional C-HT and will now be applied in clinical treatments.
Footnotes
Acknowledgments
This research was funded by grant UVA 2012 5539 of the Dutch Cancer Society. Takeda contributed to the development of the catheter with an unrestricted research grant.
Disclosure Statement
No competing financial interests exist.