
Abstract
Background and Purpose:
A baseline kidneys, ureters, and bladder (KUB) radiograph, at the time of computed tomography (CT) for ureteral stones, might aid interpretation of future KUBs. The CT scout radiograph might render the baseline KUB redundant, however. We sought to assess the diagnostic utility of baseline KUB for patients with ureteral stones.
Patients and Methods:
Patients with ureteral stones were retrospectively identified. All had a baseline KUB in addition to CT and were reassessed after 4 to 60 days with KUB. Each patient's imaging was randomized 1:1 into either “KUB&CT” or “CT” groups. Three urologists independently assessed the imaging: CT (with scout film) and baseline KUB in the KUB&CT group, but only the CT (not KUB) in the CT group. Definitive stone assessment on follow-up KUB was defined as all three reviewers answering either Yes or No (not Indeterminate) to the question of stone passage or migration.
Results:
Of 154 stones, the mean diameter was 4.8±2.1 mm, density was 914±300 Hounsfield units (HU), with 54.4% in the distal ureter. Stone visibility was 60.4% on KUB vs 43.5% on scout film (P<0.001). Scout film visibility favored the CT group (52.7 vs 35.0%, P=0.027). After adjusting for body mass index, skin-to-stone distance, size, density, and location, definitive assessment rates were higher in the KUB&CT group (P=0.047). When reviewers reassessed the CT group using the baseline KUB, they were able to do so definitively in an additional 16 (21.6%, P<0.001). Definitive assessments were associated with higher rates of stone visibility on scout film (86.1 vs 21.1%, P<0.001), KUB (86.1 vs 50.0%, P<0.001), and larger (6.0 vs 3.7 mm, P<0.001), denser stones (1046 vs 802 HU, P<0.001).
Conclusions:
The addition of a baseline KUB to the CT scout film improves the ability of urologists to determine stone outcome when following patients with KUB imaging and might reduce the subsequent need for additional imaging.
Introduction
N
It is standard practice at our institution for all patients with ureteral stone(s) diagnosed on CT to undergo a baseline KUB before discharge from the emergency department (ED). As part of most CTs, however, a screening (or “scout”) digital radiograph is obtained that mimics a KUB (Fig. 1). The quality of that scout image is inferior to traditional KUB radiographs, and the sensitivity of the CT scout for detecting calculi seen on CT has been reported to be 17% to 52%. 2 –6 The American Urological Association (AUA) guidelines for the imaging of ureteral calculi recommend a baseline KUB only when the stone is not visible on the scout, 1 because the two studies might be redundant. No studies have addressed whether interpretation of future KUBs is facilitated by the presence of a baseline KUB, in addition to the scout film, however.
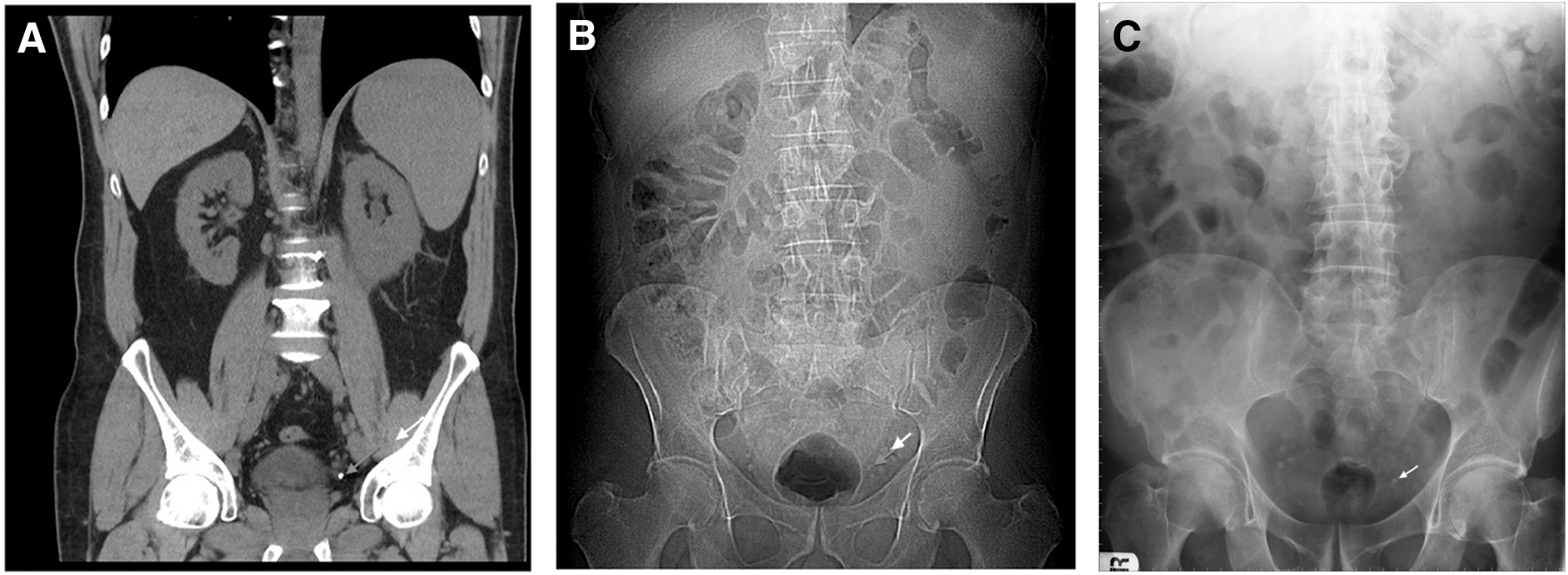
Examples of imaging studies in the same patient, with left distal ureteral calculus shown by arrows.
The objective of this study was to determine whether the ability of urologists to determine a stone's status on a follow-up outpatient KUB is improved by the presence of a baseline KUB (in addition to the CT), or whether the CT scout radiograph is sufficient. Theoretically, if the baseline KUB improves diagnostic accuracy, further imaging (eg, ultrasonography or repeated CT) could be avoided. A secondary objective was to determine the relative imaging characteristics of ureteral stones on CT and scout and KUB radiographs.
Patients and Methods
After Institutional Review Board approval was obtained, this study was performed including patients referred to the Stone Clinic from the ED at a single center (St. Michael's Hospital). Patients presenting with ureteral stone(s) on CT between September 2007 and June 2011 were retrospectively identified. All patients had a baseline KUB performed within 24 hours of the CT, and then underwent a follow-up KUB 4 to 60 days after the CT for reassessment of the stone's persistence and location. Patients without a timely follow-up KUB at St. Michael's Hospital, without ureteral stones on CT, and those <18 years of age were excluded. CTs were performed with a General Electric 64-slice scanner. Scout radiographs, using the renal colic protocol, were performed at 120 kVp (peak kilovoltage), 80 milliampere-seconds (mAs) for an anterior-posterior view. KUB radiographs were typically performed at 75 to 80kVp and 20 to 25 mAs.
Baseline data were collected, including patient information (age, sex, dates of imaging studies, height, and weight) and stone information from CT (location, maximal and perpendicular dimensions on axial images, vertical dimension on coronal images, skin-to-stone distance [SSD, measured vertically from skin to posterior edge of stone] and mean stone density). Stone locations were defined as upper (including ureteropelvic junction), mid, or lower (including ureterovesical junction [UVJ]) ureter.
The primary research question was whether interpretation of a KUB, performed in the outpatient setting to reassess a known ureteral stone, is improved by having a baseline KUB along with the CT, or whether the CT with its scout radiograph is sufficient. To answer the question, each patient's imaging was randomized 1:1, using a randomization table, to either the “KUB&CT” or “CT” group (Fig. 2).

Flow diagram depicting study design. KUB=kidneys, ureters, and bladder; ER=emergency room; CT=computed tomography; F/U=follow-up.
Three independent urologists retrospectively reviewed the imaging for each stone to answer the question “on this follow-up KUB, has the stone passed or migrated since the CT?” All three urologists were blinded to patient outcomes and treatment. The three urologists independently reviewed the follow-up KUB (4–60 days post-CT) and the baseline CT (including axial, coronal, and scout images) for all patients. In the KUB&CT group, the baseline KUB (performed within 24 hours of the CT) was also used to answer the question of stone passage, but in the CT group, the baseline KUB was not viewed. Window and level setting were individually optimized for each stone. If all three urologists independently answered either “yes” or “no” to the question of stone outcome on the follow-up KUB (rather than “indeterminate/maybe”), the assessment was considered “definitive.” Clinically, definitive assessments of follow-up KUBs would not need further imaging, such as ultrasonography or repeated CT, to determine the stone's status. The rates of definitive assessment were compared between the KUB&CT and CT groups.
After all assessments were completed, the imaging for each stone in the CT group was reassessed, now also with the baseline KUB. Each urologist also rated the stone's visibility (visible, slightly visible, or not visible) and size (in two dimensions) on the baseline KUB and scout film. A stone was defined as visible if all reviewers rated it either visible or slightly visible, and the stone measurements were reported as the mean of the reviewers' measurements.
Parametric data were compared with one-way analysis of variance and paired t test and nonparametric data with the chi-square or Fisher exact test, where appropriate. Multivariate binary logistic regression modeling was used to adjust for SSD, density, maximal dimension, and location to determine if definitive assessment rates differed between the KUB&CT and CT groups. Data analysis was performed using StatPlusmac:2009 and SPSS 21, with P values <0.05 considered significant.
Results
After randomization, there were 154 stones: 74 in the KUB&CT and 80 in the CT group. Patient and CT stone characteristics did not differ significantly between the groups (Table 1). KUB had greater sensitivity for stone detection than CT (60.4% visible on KUB vs 43.5% visible on scout, P<0.001) (Table 2). The rates of definitive assessment of the follow-up KUB did not differ statistically between the CT and KUB&CT groups (48.6 vs 42.5%, P=0.444). Agreement between the KUB and CT scout radiographs in identifying ureteral stones was 76.6%. Five (3.2%) stones were visible only on the CT scout film, while 31 (20.1%) were visible only on the KUB scout film. In addition, when the three reviewers were asked to look back at the KUB radiograph in the CT only group, they were able to definitively assess stone outcome in an additional 16 (21.6%) of patients at baseline, compared with CT scout alone.
CT=computed tomography; KUB=kidneys, ureters, and bladder; BMI=body mass index; HU=Hounsfield unit.
CT=computed tomography; KUB=kidneys, ureters, and bladder.
On univariate analysis (Table 3), definitive assessments in the CT group were associated with higher rates of stone visibility on scout radiographs (86.1 vs 21.1%, P<0.001) and KUB (86.1 vs 50.0%%, P<0.001). The reviewers were able to make more definitive stone assessments for larger (6.0 vs 3.7 mm, P<0.001), more dense stones (1046.3 vs 801.9 HU, P<0.001) and more upper ureteral stones (P=0.027). Neither SSD nor body mass index (BMI) differed between the indefinite and definitive assessments.
KUB=kidneys, ureters, and bladder; BMI=body mass index; HU=Hounsfield units.
On univariate analysis, definitive assessment of stone outcome did not differ between the two groups (Table 3). Despite randomization, however, there were differences between the two groups in terms of stone visualization at baseline: The CT group contained more stones that were visible on the scout film (52.7 vs 35.0%, P=0.027) with a trend toward higher visibility on KUB (67.6 vs 53.8%, P=0.080).
The relative stone visibilities and maximal dimensions for each stone on CT, KUB, and scout radiographs are illustrated in Table 4.
CT=computed tomography; KUB=kidneys, ureters, and bladder.
Multivariate analysis with binary logistic regression modeling, however, allowed adjustment for the covariates of BMI, SSD, stone density, maximal stone dimension, and stone location. Logistic regression revealed that definitive stone assessment rates were higher in the baseline KUB&CT group (P=0.046, Table 5). In addition, when the reviewers were asked to reassess stone outcome in the CT group, now using the baseline KUB, the reviewers were able to do so definitively in an additional 16 (21.6%) of cases (P<0.001). Stones located in the distal ureter, including the UVJ, were more difficult to visualize and determine outcome definitively (P=0.006). There was, however, an interaction between stone size and stone location: distal ureteral and UVJ stones were significantly smaller than mid- and upper-ureteral stones (P<0.001). Although lower BMI was a significant factor in assessing stone outcome (26.1 vs 29.3, P=0.030), SSD was not.
KUB=kidneys, ureters, and bladder; CT=computed tomography; BMI=body mass index; SSD=skin-to-stone distance; HU=Hounsfield unit; UVJ=ureterovesical junction; UPJ=ureteropelvic junction.
Discussion
While noncontrast CT of the abdomen and pelvis has become the main diagnostic test for patients with acute renal colic, it is not the ideal imaging modality for serial follow-up of patients with identified ureteral stones, because of financial, resource limitation, and radiation exposure concerns. Abdominal radiography, particularly KUB, is the mainstay for following radiopaque stones in the outpatient setting to reassess stone persistence and location. It is common practice to monitor patients with known ureteral stones, which have not been documented to pass, at 1 to 2 week intervals using abdominal radiography. 2 A baseline abdominal radiograph has been presumed to be helpful in interpreting subsequent radiographs, because it demonstrates the stone's degree of radiopacity, establishes the bony anatomy, and demonstrates the pattern of phleboliths and other calcified structures that can mimic stones. The scout radiograph generated as part of an axial CT scan, however, might make a baseline KUB redundant. Although numerous studies have compared the imaging characteristics of KUBs and scout radiographs, no study to date has tested how relying solely on a CT scout, without a baseline KUB, might impact the clinician's ability to interpret future radiographs of the stone.
Our data demonstrates that interpretation of KUBs in patients with known ureteral stones is improved by viewing a baseline KUB, in addition to a CT. While there was no added benefit to the baseline KUB on univariate analysis, there were confounding covariates (stone size, location, density, and patient BMI) that rendered more stones visible on the CT scout in the CT group (P=0.027), and there was a trend toward more stones being visible on KUB (P=0.080). Given that definitive assessment was associated with higher rates of stone visibility on scout and KUB radiographs, as seen in Table 3, the baseline differences (with more visible stones in the group without a baseline KUB) might have accounted for the similar rates of definitive assessment.
To account for these baseline differences between the groups, multivariate binary logistic regression modeling was performed, to control for factors that might influence the ability to visualize the stone on radiography (BMI, SSD, density, stone size, and location). While none of these factors was individually significant, when taken together, there were small differences between the two groups (ie, the CT group had slightly smaller, less dense, more distal ureteral stones that might be difficult to distinguish from phleboliths). This regression analysis confirmed that assessment with baseline KUB, in addition to the baseline CT, was more likely to be definitive than those without the baseline KUB (P=0.046). In addition, when the reviewers reassessed each stone in the CT group using the baseline KUB, an additional 16 (21.6%, P<0.001) assessments were converted to definitive.
The rate of stone visibility on scout radiography was similar to previously published rates (43.5%) and was significantly lower than the visibility rate on KUB (60.4%, P<0.001). Interestingly, the measured stone diameter was similar on the CT axial images and scout radiograph (P=0.713) but larger on KUB than the other two modalities (P<0.001, Table 4). The first report on CT scout radiography was by Chu and associates 2 in 1999, in which 49% of stones were found to be visible. and Jackman and colleagues 4 and Assi and coworkers 7 were the first to directly compare the sensitivities of scout and abdominal radiographs for ureteral calculi and found KUBs to be more sensitive than scouts, which has been confirmed by multiple studies. 3,5,6 Higher scout radiograph sensitivity has been reported with larger stones. 2,6 –8 upper ureteral stones, 8 lower kilovoltage settings, 2 and denser stones. 8 Based on the correlations of CT (with scout) findings and abdominal radiography, as well as the finding that no stone visible on the scout was missed on KUB, 5 –7 many authors have concluded that a scout radiograph could replace a baseline KUB for stones that are detectable on the scout. 3,4,6,7 Five (3.2%) stones in this study, however, were visible on the scout and not on KUB.
Though the AUA Guidelines for the imaging of ureteral calculi recommend a baseline KUB only when the stone is not visible on the scout film, 1 this is often impractical. This practice would necessitate a physician (either radiologist, emergency physician, or urologist) to assess the CT scout film before deciding whether to perform a KUB. Furthermore, at our institution, the final radiologist CT reports do not include an interpretation of the CT scout radiograph, although this practice has been recommended. 7 While the patient is in the radiology department, it is more efficient to simply perform a KUB along with the noncontrast CT, particularly because this study demonstrates the added diagnostic sensitivity of the baseline KUB and the added diagnostic value when later interpreting subsequent abdominal radiographs. In the outpatient setting, improved diagnostic certainty on follow-up KUBs might help avoid additional testing to reassess the ureteral stone's status, with the associated costs and possible radiation exposure, such as repeated CT or ultrasonography.
The results need to be interpreted in the context of the study's limitations. Outcomes, including stone visibility and persistence or migration at follow-up, were based on the aggregate of the three assessments, rather than a consensus. The aggregate, however, might resemble real practice more closely, particularly because the three reviewers were urologists. The urologist assessments of the follow-up KUBs were neither clinically confirmed, because the stone composition and whether the stone had truly passed were not retrospectively available in most cases, nor radiologically confirmed by a repeated CT. Relying on an aggregate of three qualified reviewers' independent assessments, however, should increase the accuracy of their diagnostic confidence. Also, the lack of reviewer blinding to the stone's group (ie, KUB&CT or CT) is a potential source of bias.
To our knowledge, this is the first study that tests the relative utilities of a baseline KUB and a CT scout radiograph when applied to a common clinical scenario. The simulation of a patient's outpatient follow-up directly answers the question that the previous studies have addressed in an indirect fashion. The population was large, which is beneficial because the stones were heterogeneous. We included even the stones that were not visible on scout or abdominal radiography, because clinicians do not know about a stone's visibility (or lack thereof) when the baseline KUB is performed along with the CT. Further prospective study is warranted to confirm the benefit of the baseline KUB.
Conclusions
A baseline KUB, performed once ureteral stones are diagnosed on a noncontrast CT, including its scout radiograph, improves the clinician's ability to interpret follow-up radiographs in the outpatient setting. Theoretically, the increased diagnostic certainty afforded by the baseline KUB could obviate further imaging (eg, CT or ultrasonography) along with their expense and possible increased radiation exposure. We will continue to perform a baseline KUB at our institution for all patients with ureteral stone(s) on CT.
Footnotes
Disclosure Statement
No competing financial interests exist.