
Abstract
Purpose:
To assess application of cystatin C and neutrophil gelatinase-associated lipocalin (NGAL) as biomarkers for renal ischemic injury. We also evaluated the use of allopurinol as a renoprotective agent. A second goal was to assess cystatin C as a biomarker in patients undergoing partial nephrectomy.
Methods:
Using 58 Sprague-Dawley rats, we evaluated urinary cystatin C (n=26) and NGAL (n=32) as a biomarker for renal ischemia injury. Half of the rats were pretreated with allopurinol; the other cohort served as a control. The right renal hilum was ligated in all rats, thereby creating a solitary kidney model. After a 30-minute stabilization period, the left hilum was clamped for time periods of 15, 30, and 60 minutes. Urinary levels of cystatin C and NGAL were then measured at the following time points: Preclamp (after the 30-minute stabilization period) and postclamp (30, 45, and 60 minute periods after unclamping). For our clinical subjects, serum cystatin C levels (n=17) were obtained preoperatively, at the induction of anesthesia before robot-assisted partial nephrectomy, immediately postoperatively, and on postoperative days 1 and 2. Three of these patients had their tumors excised off clamp and served as controls. We then estimated glomerular filtration rate by using the Creatinine-Cystatin C Equation.
Results:
Urinary levels of cystatin C and NGAL increased after renal clamping. The 30-minute period of ischemia demonstrated the greatest increase of these biomarkers. Allopurinol did appear to serve a renoprotective function in those animals undergoing 30-minute clamp times. In our clinical patients, the serum cystatin C levels did increase at each postoperative time point, but remained nonelevated in the control group.
Conclusions:
Cystatin C and NGAL both appear to be useful biomarkers of renal injury. Studies with larger numbers are needed, however. Also, allopurinol does exhibit renoprotective effects against ischemic injury.
Introduction
A
Urinary cystatin C and neutrophil gelatinase-associated lipocalin (NGAL) represent potential early biomarkers of acute kidney injury. Our hypothesis was to first determine if urinary cystatin C and NGAL levels can quantitate renal damage secondary to warm ischemia through experiments in a solitary kidney animal model. A second goal was to investigate use of allopurinol for renoprotective abilities in this same animal model, using cystatin C and NGAL findings to quantify the protective effects.
Finally, we evaluated the clinical utility of cystatin C in a clinical series of patients who underwent robot-assisted partial nephrectomy. Our hypothesis was that cystatin C could be used as a clinical biomarker after surgery to assess acute kidney injury postoperatively. Unfortunately, our hospital laboratory does not have the ability to quantitate NGAL levels, and thus only cystatin C was studied in our surgical population.
Methods
All of the experimental procedures described in this study were approved by and performed in accordance with the guidelines established by the Institutional Animal Care and Use Committee. These experiments were conducted in male Sprague-Dawley (SD) rats weighing 350 to 450 g that were purchased from Charles River Laboratories (Wilmington, MA), housed at least 3 days for acclimatization in a temperature- and light-controlled room, and allowed free access to a standard diet (Ralston-Purina, St. Louis, MO) and tap water. Fifty-eight study animals underwent experimentation, divided into cystatin C (n=26) and NGAL (n=32) groups. Half of the rats were pretreated with allopurinol, and the other cohort of animals was used as controls.
Rats were anesthetized with thiobutabarbital sodium (Inactin; Sigma-Aldrich) at a dose of 100 mg/kg. Supplemental doses of anesthesia were administered throughout the experimental period as needed. The rats were placed on a servo-controlled surgical table that maintained body temperature at 37°C. Tracheostomy was performed, and the animals were continuously provided with a mixture of 95% O2 and 5% CO2 through the endotracheal tube. The right jugular vein was catheterized for intravenous administration of 6% albumin solution.
A PE100 catheter was inserted into the bladder of rats to collect the urine effluent, and urinary cystatin C and NGAL levels were then analyzed (Fig. 1). The right renal hilum and ureter were first exposed and ligated, thereby creating a solitary kidney model. After a 30-minute stabilization period, the experimental protocol was initiated. The left renal hilum was isolated and clamped (Figs. 2 and 3). Urine was collected during the following periods: Preclamp (after 30 minutes of initial equalization) and postclamp (30, 45, 60 minutes after unclamping). Rat urines were analyzed for cystatin C and NGAL levels at each period.

Catheterization of rat bladder.

Clamping of renal hilum.
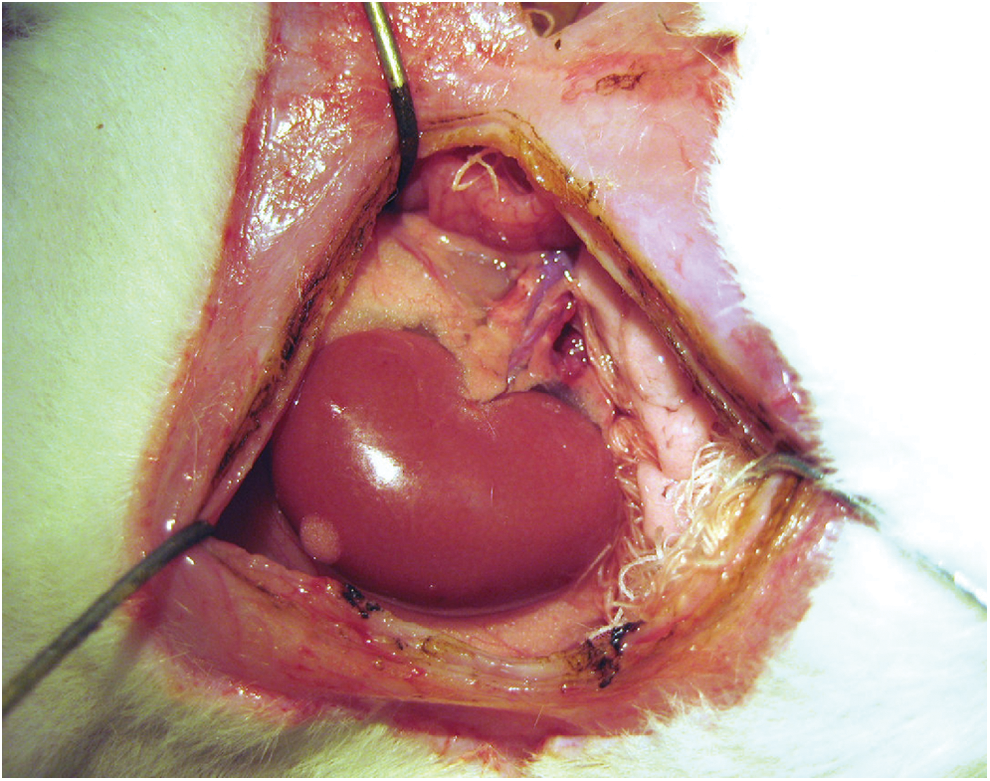
Reperfusion of kidney.
Additional animals were used to study the effect of allopurinol on renal ischemia-reperfusion injury. Rats were pretreated with allopurinol (100 mg/kg) (MP Biomedicals) injected as a bolus at least 1 hour before renal clamping. The procedure included a 30-minute equalization period, followed by measurements of cystatin C and NGAL levels in the rat urine before clamping. A different rat was used for separate intervals of 30, 45, 60 minutes after unclamping the renal hilum, the same as had been performed in the rats that were not premedicated with allopurinol.
The rats were sacrificed at the end of the experiment. All urine samples were preserved with 0.005% butylhydroxytoluene prepared in ethanol and kept frozen (−80°C) until analyzed. The urine samples were subsequently analyzed for cystatin C and NGAL levels using a cystatin C and NGAL enzyme-linked immunoassay kits and BMG Labtech OPTIMA microplate reader.
For the clinical portion of the study, we obtained serum cystatin C samples from 17 patients immediately preoperatively (just before induction of general anesthesia), immediately postoperatively (in the postanesthesia care unit), and on each postoperative day. Three of these patients had their tumors excised off clamp with zero ischemia and served as controls. We then estimated the GFR by using the creatinine-cystatin C equation (Chronic Kidney Disease Epidemiology Collaboration [CKD-EPI] 2012), 1 and compared this value to the GFR as calculated by creatinine alone.
Results
Part I. Cystatin C and NGAL animal experiments, solitary kidney ischemia
With a 15-minute clamp time, cystatin C values increased 11.7 fold compared with controls. With a 30-minute clamp time, the ratio of cystatin C increased 14.5 and appeared to peak at this length of warm ischemia. At a prolonged 60-minute clamp time, the cystatin C levels dropped to a 10.5 ratio (Table 1). The 30-minute period of ischemia consistently demonstrated the greatest increase compared with controls.
The findings with NGAL also demonstrated a peak level of damage at 30 minutes, with a 4.13 fold increase over controls. Our findings in our experiments on SD rats indicated that cystatin C and NGAL appear to be reliable indicators of renal injury, with reproducible maximal levels of damage at 30 minutes. The values for both biomarkers increased at all time points after the clamping and unclamping of the renal artery.
Part II. Cystatin C and NGAL animal experiments, solitary kidney ischemia with allopurinol
With both cystatin C and NGAL, allopurinol did appear to serve as a renal protectant in those rats that underwent a renal artery clamp time of 30 minutes or greater (Fig. 4). There was a decrease in cystatin C ratios from 14.5 without allopurinol to 9.1 with pretreatment of allopurinol. With NGAL, there was also a demonstration of decrease of the marker from a 4.13 ratio down to 2.11 with pretreatment of allopurinol at 30 minutes.
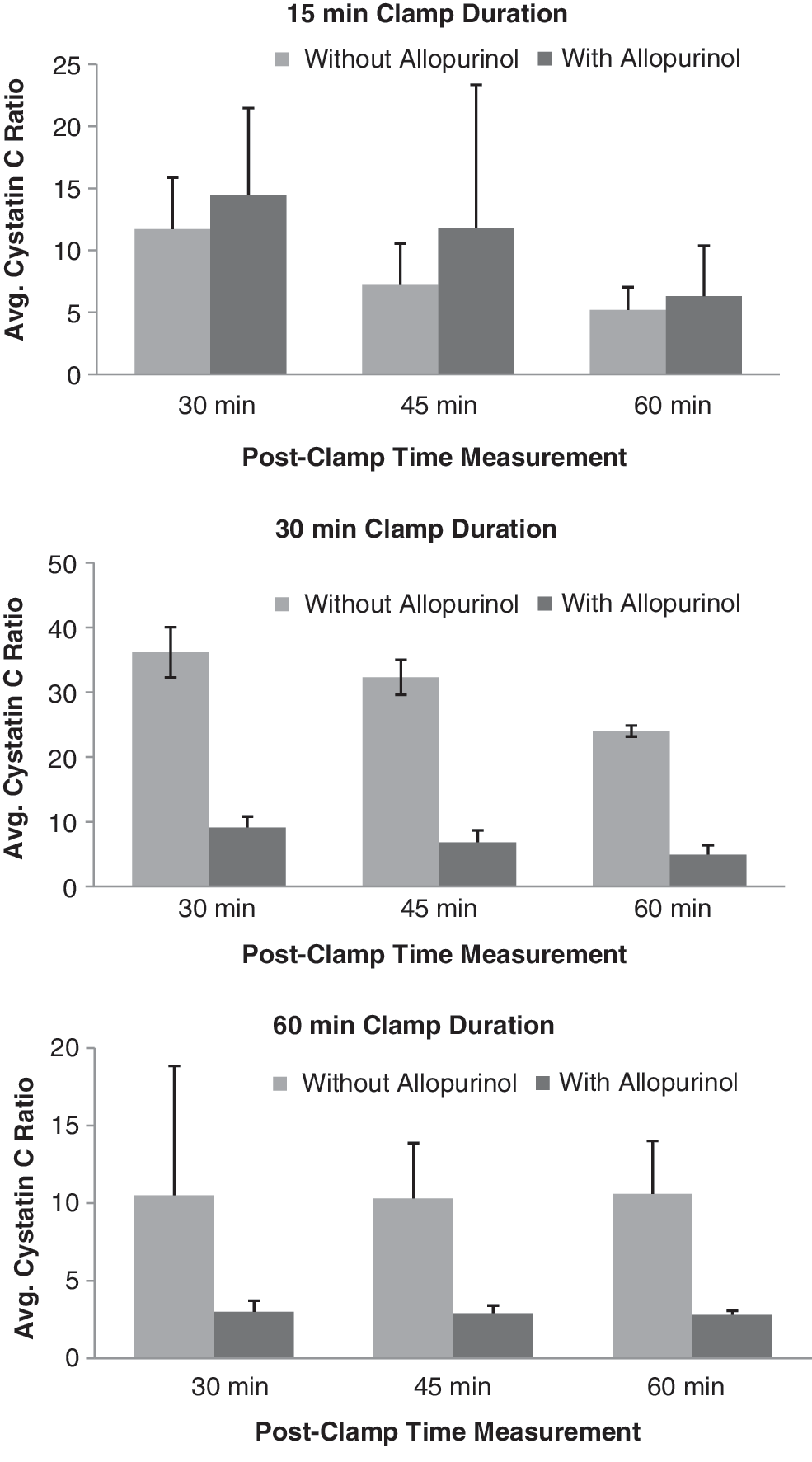
Protective effect of allopurinol in the cystatin C group. Effect is only seen at 30 minute clamp duration and greater. X-axis represents the ratio of cystatin C at that time interval compared with the preclamp value.
Part III. Clinical patients undergoing robot-assisted partial nephrectomy
For our measurements of cystatin C in our surgical patients undergoing partial nephrectomy, we elected to incorporate the use of cystatin C into the CKD-EPI 2012 4 equation in an effort to obtain meaningful data on GFR postoperatively. This newly formulated GFR was then compared with GFR estimates based on creatinine alone. The overall trend demonstrated an increase in the GFRs calculated with the combined use of cystatin C and creatinine, compared with those calculations made from creatinine alone. Average change in creatinine in these patients was minor, given the fact that there was a normal contralateral kidney. In fact, average preoperative creatinine was 1.05 mg/dL and postoperatively rose only to 1.17 mg/dL. Using the CKD-EPI 2012 1 equation with incorporation of cystatin C values into the calculations, we observed a 12.1% increase in the GFR on postoperative day 2 compared with the GFR calculated by the Modification of Diet in Renal Disease equation. With regard to the values themselves, the average cystatin C values for those patients undergoing renal artery clamping did increase each day, with an average value of 1.033 preoperatively and an average of 1.229 on postoperative day 2, whereas the values for controls—patients with no clamping of the renal artery and who underwent off clamp excision—remained flat throughout the postoperative period.
Discussion
One of the few modifiable factors in limiting the degree of renal damage incurred during minimally invasive partial nephrectomy is warm ischemia time (WIT). Historically, the “safe” amount of WIT has been thought to be 30 minutes. The urologic literature reports a wide range of acceptable WITs, however. Godoy and associates 2 report 40 minutes to be a reasonable cutoff, whereas, Lane and colleagues 3 think any ischemia time greater than 20 minutes may compromise long-term function of the kidney.
While a nuclear renal scan (NRS) with a radiotracer such as Mag-3 or dimercaptosuccinic acid is one option for determining renal damage after laparoscopic or robot-assisted partial nephrectomy, this method is cumbersome for the patient (and sometimes clinically irrelevant for an individual patient), in addition to being prohibitively expensive in this era of limiting costs. And while NRS is considered the gold standard, there is still some variability in the interpretation of this test between radiologists.
Historically, clinicians have relied on the serum creatinine level to monitor renal damage after partial nephrectomy. There are many factors, however, that can confound and skew creatinine levels postoperatively. Given that patients with stage III chronic kidney disease (CKD) have an increased risk of death, it is important to accurately identify those patients who will need closer follow-up after partial nephrectomy. 1,4 Because creatinine can be affected by diet, muscle mass, race, age, and sex, scientists and clinicians have searched for more accurate methods of identifying those patients with decreased GFR. Other problems with the use of creatinine to monitor the degree of renal injury in the acute setting include the fact that there is a lag time associated with renal damage and a resultant rise in creatinine. Also, it takes an approximately 50% reduction in kidney function before an increase in creatinine is seen. The need for early detection of renal injury has recently led to the goal of identifying novel serum and urine biomarkers, an almost “troponin-like marker,” with high sensitivity and specificity for diagnosing renal cellular injury. 5
Cystatin C first underwent consideration as a predictor of GFR in 1985. 6 It is a nonglycosylated 13 kDa basic protein that is a member of the cystatin superfamily of cysteine protease inhibitors and is produced by all nucleated cells. Cystatin C is filtered by the glomerulus, then undergoes essentially complete tubular reabsorption and catabolism (without secretion). Thus, it is not normally present in the urine in appreciable amounts. 7 Unlike creatinine, cystatin C does not appear to be significantly affected by those previously mentioned factors of sex, muscle mass, and diet. 8 Clinically, it may be measured in the urine or the serum when attempting to make determinations of acute kidney injury (AKI). Most of the studies in the literature have used serum levels in assessing renal damage.
In their recent article, Inker and coworkers 1 found that by combining the variables of creatinine and cystatin C into one equation, they could better predict GFR compared with equations based on either of those variables alone. They found the results to be more accurate and also noted improved precision when using an equation that combined both variables. The authors noted that this equation maybe especially useful in those patients who were at high risk for CKD and in those who had GFRs of 60 to 74 mL/min without albuminuria. These patients could in turn be more accurately classified and referred to a nephrologist if stage III CKD was confirmed.
Another important factor in looking at cystatin C as a marker for acute renal injury is determining the time it takes for cystatin C to reflect a change in GFR. This question was investigated by Herget-Rosenthal and colleagues 9 in 2005 when they evaluated patients who had undergone donor nephrectomy—patients who they knew would experience a measurable and dramatic decrease in GFR. They noted that cystatin C rose after 1 day, while creatinine increased 2 days after surgery. Ultimately, further analysis showed that cystatin C increased earlier than creatinine by 1.4 days.
Cystatin C does have limitations in its use as a correlate for predicting GFR. Hypo- or hyperthyroidism can affect production of cystatin C. Cystatin C levels are artificially low in the hypothyroid state and high in the hyperthyroid state. Treated thyroid disease, however, in which that person is in a euthyroid state, does not affect cystatin C. 10 Also, cystatin C concentrations are higher in patients on high-dose steroid therapy; consequently, those GFR estimates would tend to be artificially low compared with the true GFR. 11
NGAL, a 25 kDa member of the lipocalin family, is markedly upregulated in the early postischemic mouse and rat kidney. Serum and urine NGAL levels are elevated earlier than serum creatinine in the setting of delayed graft function after kidney transplantation and also after percutaneous coronary intervention. NGAL is actually produced by hepatic, intestinal, pulmonary tissue, and renal tubular cells. With tissue injury, it is substantially upregulated. NGAL is filtered by the glomerulus and undergoes reabsorption in the proximal tubule. It is secreted in minimal amounts by the thick ascending limb of the renal tubule. 12
The use of NGAL for clinical applications has now been well documented. Most of the studies pertaining to the use of NGAL have come from the cardiothoracic surgery, transplant, and critical care literature. Based on some of these findings, it has been noted that increased levels of serum NGAL may be seen as soon as 2 hours after a renal insult. 13 It seems that urine and plasma levels of NGAL are both equally acceptable as markers of AKI, 14 although there are some reports that urinary NGAL may have a slightly higher predictive value, at least in the critical care environment. NGAL appears to perform better in cases of an isolated renal insult, such as the clamping of the renal artery, rather than in cases of protracted or multiple events (such as those seen in intensive care units). 13 One potential drawback to NGAL is the considerable extrarenal production that can be seen in states of systemic stress, even in the absence of renal damage; it has also been noted to increase in states of chronic, not just acute, kidney dysfunction. Nevertheless, in a large meta-analysis, NGAL did have prognostic significance for clinical outcomes, notably for the need for dialysis and also mortality. 14
We also chose to investigate the potential renoprotective effects of allopurinol in our rat model, and the results of these findings were the most compelling aspect of the rat study. The protective effect of the allopurinol on the kidney as evidenced by decreased levels of cystatin C and NGAL was statistically significant beginning at 30 minutes after reperfusion. Our findings are congruent with previous studies demonstrating the benefits of allopurinol in guarding against ischemia and reperfusion injuries, 15 and in animal studies involving transplant kidneys, those pretreated with allopurinol have been shown to have less damage from ischemia. 16 It is believed that xanthine oxidase may give rise to free radicals during ischemia-reperfusion injury; allopurinol is an inhibitor of xanthine oxidase.
Conclusion
It appears that cystatin C and NGAL have a correlation to AKI based on our animal studies. Our study did have some limitations, however. One significant deficit in our study on these biomarkers after renal ischemia was the period in which we collected urine after renal artery unclamping. Reported time points for which cystatin C levels peak after a renal insult differ from 6 hours to 1 to 2 days, but certainly our results may have become more lucid if we had had the resources to obtain cystatin C levels throughout a longer time point. 7 Also, much larger numbers are needed to more sufficiently power the study.
We think that based on our findings of the renoprotective effect of allopurinol against ischemia-reperfusion injury based on these biomarkers, this should be further investigated in a clinical population of patients undergoing partial nephrectomy with warm ischemia.
In our clinical patients, the GFRs calculated with the use of cystatin C, as compared with creatinine alone, did show a slight elevation in the values, especially by postoperative day 2. Its use in this setting may be useful not only in trying to quantify renal ischemia, but also in following more accurately and closely those patients who are on the borderline of entering stage III CKD. This is of paramount importance, because it has been shown that these patients fare worse, with higher mortality rates, over the long term. Also, more accurately determining the GFR may have implications in the dosing of medications, and in making decisions regarding the allocation of limited resources, such as when to refer patients to a nephrologist and in the ordering of tests to screen for and manage the commonly associated morbidities that accompany CKD. 1 Also, our average WIT at our institution is 19.5 minutes, and more patient accrual with an inevitably larger range of ischemia times may help to further determine the optimal amount of ischemia time that can be induced before irreversible kidney damage occurs.
Footnotes
Disclosure Statement
No competing financial interests exist.