
Abstract
Background and Purpose:
There is a growing interest in minimally invasive treatment of primary obstructive megaureter (POM) in children. The absence of long-term follow-up data, however, makes it difficult to establish the indication for an endoscopic approach. The aim of our study is to determine the long-term efficacy of endourologic high-pressure balloon dilation of the vesicoureteral junction (VUJ) in children with POM that necessitates surgical treatment.
Methods:
We retrospectively reviewed the clinical records from children with POM who were treated with endourologic high-pressure balloon dilation of the VUJ from March 2003 to April 2010. To determine the long-term, a cohort study was conducted in November 2011. Endourologic dilation of the VUJ was performed with a semicompliant high-pressure balloon (2.7 FG) with a minimum balloon size of 3 mm, followed by placement of a Double-J stent.
Results:
We have treated 29 (32 renal units, left [n=16], right [n=10] and bilateral [n=3]) children with a diagnosis of POM within this period. The median age at the time of the endourologic treatment was 4.04 months (range 1.6–39 months). In three cases, an open ureteral reimplantation was needed, in two cases because of intraoperative technical failure and postoperative Double-J stent migration in one patient. The 26 children (29 renal units) who had a successful endourologic dilation of the VUJ were followed with ultrasonography and MAG-3–Lasix (furosemide) studies that showed a progressive improvement of both the ureterohydronephrosis and drainage in the first 18 months in 20 patients (23 renal units) (69%). In two patients who were treated with a 3 mm balloon, a further dilation was needed, with an excellent outcome. The cohort study (at a median follow-up of 47 months) showed that in all patients who had a good outcome at the 18-month follow-up after endourologic balloon dilation remained asymptomatic with resolution of ureterohydronephrosis on the US and good drainage on the renogram, in the children with some persistent hydronephrosis.
Conclusions:
Our study shows that children with POM who were treated with high-pressure ballon dilation of the VUJ who have satisfactory appearance at 18 months maintain these results over time.
Introduction
T
In the last decade, an interest in an initial temporary approach to deal with this challenging issue in pediatric urology has grown, and different surgical 2 and minimally invasive techniques has been reported. 3 The aim has been to provide adequate drainage of the pelviureteral system and prevent any further deterioration of kidney function. Once achieved, then the child (and bladder) are allowed to grow, awaiting a definitive procedure at some future point.
Primary endoscopic balloon dilation of the vesicoureteral junction (VUJ) was first described by Angulo and associates 4 in 1998 as initial therapy for children with complicated POM. Other studies have since confirmed its effectiveness either using the original technique 5 –7 or a variation of the same principle. 8 The experience in treating those patients has shown us this technique could be a valuable approach as a definitive treatment. This is the first reported experience focused on the role of endoscopic balloon dilation of the VUJ as a definitive treatment in children with POM.
The aim of this study was to present our long-term results with endoscopic balloon dilation in children with POM and demonstrate its efficacy as the definitive treatment.
We hypothesize that successful high-pressure balloon dilation of the VUJ in patients with POM that necessitates surgery could be a definitive treatment, without the need of further surgical intervention.
Methods
We retrospectively reviewed all our children with a diagnosis of POM who were treated with endourologic high-pressure balloon dilation of the VUJ and who have had a minimum follow-up of 18 months. Patients for the study were identified from our pediatric urology surgical database that registers all patients operated on in our unit since 2003.
Patients with the diagnosis of POM without any other urologic anomaly since the date high-pressure balloon dilation was introduced (2003) were included for the study.
Clinical details were obtained from the patient records with radiologic and ultrasonography (US) and renography review to confirm diagnosis. Children with other urinary tract anomalies were excluded from this study.
The diagnosis of POM was based on US evidence of significant pelviureteric dilatation (hydroureteronephrosis and a distal ureter measuring >10 mm) and radioisotope study (Tc99m-labeled mercaptoacetyltriglycine [MAG-3] and Lasix [furosemide] washout) showing obstructive curve, with progressive cumulative radiotracer and impaired split renal function. The MAG-3 furosemide protocol at our institution is F0, the drainage is quantified by calculating the T1/2 of the curve, and considered obstructive with T1/2 over 100 minutes; changes in patient position and postmicturition imaging are included for the analysis of the renography results.
The conservative treatment protocol of children with POM in our unit includes low-dose antibiotic prophylaxis (trimethroprim) and radiologic follow-up with USS and radioisotope study. A voiding cystourethrogram in all subjects excluded vesicoureteral reflux (VUR), bladder and bladder outlet anomalies.
In our unit, the indication for surgical intervention in patients with a diagnosis of POM was based on progressive increase in hydroureteronephrosis with an obstructive pattern in the renogram associated with loss of split renal function, pyonephrosis, or febrile urinary tract infection (UTI). The annual rate of prenatally diagnosed POM necessitating surgery in our unit has been 12% to 14%. Since 2003, endoscopic high-pressure balloon dilation of the VUJ is the treatment offered to all patients with POM that necessitates surgery; consent was obtained appropriately as per Institutional Board requirements.
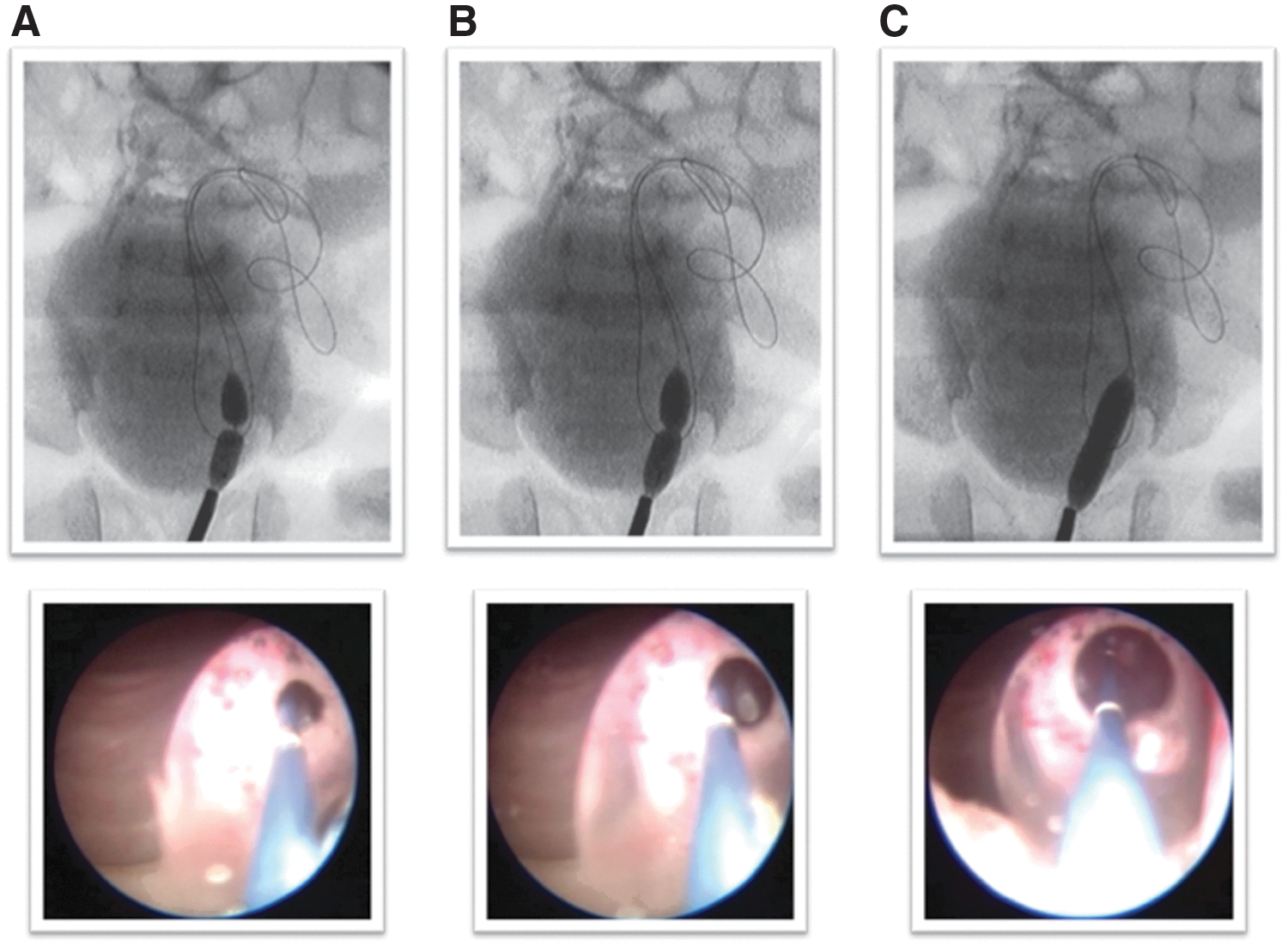
All procedures were performed under general anesthesia with appropriate antibiotic prophylaxis. A preliminary cystoscopy (9.5 FG Storz cystoscope with 5F working channel and 5 degree lens) was done in all children. For some early cases, we then performed retrograde pyelography before the dilation, using contrast through a 3 FG ureteral catheter. A guidewire (0′014″ Choice PT,™ Floppy [LS] J-tip, Boston Scientific, Natick, MA) was negotiated through the VUJ, followed by the dilating balloon. The balloons used were semi-compliant dilation catheters with a size of 2.7F to 3.1 F and a nominal diameter from 3 mm to 7 mm and 2 cm length (Wanda,™ Boston Scientific) (RX Muso,™ Terumo™). Balloons were inflated to their nominal pressures (12 atm) with a pressure inflation device until the release of the stenosis and removed immediately after. No attempt to measure the length of the stenosis was performed. Figure 1 illustrates the typical endoscopic and radiology sequence of dilation images.
The dilated VUJ is then entered with the cystoscope. A Double-J stent (3–5F, 8–12 cm to 16–20 cm, Cook Medical Europe, Limerick, Ireland) was then left in situ. After the procedure, children remained on free drainage through the bladder catheter for 24 hours to prevent complications related to bad bladder empting after the procedure. Nonsteroidal anti-inflammatory analgesics were prescribed as needed.
Double-J stents were removed at 4 to 6 weeks at a second cystoscopy. At Double-J stent removal, the VUJ was calibrated by direct cystoscopic examination. When the cystoscope could be introduced through the VUJ, it was considered a satisfactory result. If the VUJ could not be entered with the cystoscope at the time of the Double-J stent removal, a new dilating catheter was introduced and inflated to its nominal diameter to assess the diameter of the VUJ (calibration), and no further Double-J stent intervention was performed.
All children then underwent a standard follow-up protocol; this included a clinical review and US at 3, 6, 12, and 18 months after the Double-J stent removal and a MAG-3–furosemide study at 12 and 18 months. Voiding cystourethrography (VCUG) was performed only if patients presented with UTI or persistent obstruction seen on a diuretic renogram.
The data included for the study were US findings, MAG-3–furosemide results, VCUG when performed, and clinical data (UTIs).
The US parameters recorded were the retrovesical diameter of the distal ureter and the anteroposterior renal pelvic diameter, and the grade of hydronephrosis as per the Society for Fetal Urology, 9 preoperatively and at 3, 6, 12, and 18 months after the endoscopic treatment.
The data analyzed from the MAG-3–furosemide study were the split renal function, T1/2, and the shape of the curve in the examinations performed preoperatively and at 12 and 18 months postoperatively.
Aiming to determine the long-term results, a cohort study was designed including those patients who had a successful endourologic dilation of the VUJ. For the cohort study, a planned review of this subset of patients was performed in November 2011. For this purpose, patients included in the cohort study were reviewed in clinic, all urinary tract related symptoms (UTIs, symptoms of bladder dysfunction) were recorded and US was performed. If any residual ureterohydronephrosis was detected at US, a MAG-3–furosemide study was performed.
The research protocol was approved by the Committee of Bioethics at our institution. Data are expressed as median (and interquartile range [IQR]) and mean (±standard deviation) where appropriate; for statistical analysis, a chi-square was performed for qualitative variables and a t-test for quantitative, two-tail analyses. The analyses were performed using the IBM software SPSS 18.
Results
From March 2003 to April 2010, 29 (32 renal units) children with isolated POM were treated with endoscopic balloon dilation. There were 18 (62%) boys and 11 (37%) girls, and the POM was left-sided (n=16), right-sided (n=10), or bilateral (n=3), making a total of 32 ureteral units. Median age at the time of endoscopic intervention was 4.03 (IQR 11,76) months.
Clinical indications for intervention included progressive increase in hydroureteronephrosis with an obstructive pattern on the renogram associated with loss of split renal function 21 with further deterioration of split renal function (n=4), recurrent UTI (n=2), and pyonephrosis (n=2).
Endoscopic intervention was indicated in the remainder because of increasing pelviureteral dilatation, thinning of renal parenchyma with persisting obstructive curve on renography with associated impairment of the split renal function. The median differential renal function of the affected side in these patients was 36% (range 24%–43%). In all cases, the shape of the renogram curve was obstructive, with T1/2>100 minutes.
There were 29 children with the diagnosis of POM that necessitated surgical management in whom endoscopic dilation was the intended treatment (32 renal units). In two children, ages 6 and 16 months, endoscopic dilation could not be performed because of failure of the guidewire to pass through the VUJ; they went on to successful open ureteral reimplantation. In the remaining 27 children (30 renal units), a successful endoscopic dilation was performed with a median operative time of 28 (IQR 10) minutes. In one of the cases, the Double-J stent could not be inserted because of accidental exit of the guidewire, and a percutaneous nephrostomy was placed instead with a good postoperative outcome.
We had one postoperative complication. In one of the patients in whom the dilation was performed successfully, the Double-J stent migrated into the renal pelvis. Subsequently, an open ureteral reimplant was then needed because of acute onset of abdominal pain and associated increase in pelviureteral dilatation.
At Double-J stent removal and VUJ calibration, the 9.5F cystoscope could be introduced through the VUJ in 17 ureters. In the remaining 11 ureters, a dilating catheter was inserted and inflated (5–6 mm) at the time of stent removal. A soft minimal narrowing was noted at balloon inflation in eight. In these cases, the narrowing disappeared at minimal pressure and no Double-J stent was inserted.
A case review of 26 children (29 renal units) who had successful endoscopic dilation was performed.
There was progressive improvement of both hydroureteronephrosis and drainage (assessed by renal US and renography) in 20/29 (69%) renal units. Figures 2 and 3 illustrate the US and renography images of case #9 of these series preoperatively and the results at 18 months postoperative follow-up.

Case 9 of the series. Image of ultrasonography of the distal ureter before the procedure and the mercaptoacetyltriglycine–furosemide scan.

Case 9 of the series. Image of ultrasonography and the mercaptoacetyltriglycine–furosemide scan at 18 months postoperative follow-up.
There was persistent hydroureteronephrosis in four patients with persisting obstructive features on renography but without VUR. Two were early in the series and dilation was with a 3 mm balloon initially. Further endoscopic dilation with a 6 mm balloon was straightforward and effective. In the other two patients, reimplantation was performed at 12 and 14 months postendoscopic treatment; neither of these two children needed tapering at theopen procedure.
Five children presented with UTI during follow-up, and cystography showed secondary VUR. Subureteral endoscopic injection of Deflux® (Oceanea, Dublin, Ireland) was successful in three patients, but failed in two who needed open ureteral reimplantation.
The statistical analysis revealed that there were not significant differences in the success rate related to sex (Fisher exact test P=0.36) or age (P=0.085) of the patient at the endoscopic procedure.
In summary, as shown in Diagram 1 (Supplementary Material is available online at
In 22 patients (25 ureters) treated, no open surgery was needed; these patients were included for the cohort study.
The cohort study included the children having successful high-pressure balloon dilation of the VUJ that did not need open reimplantation (22 patients/29 patients) with median follow-up of 47 (IQR 39,07) months.
No episodes of UTI or symptoms of bladder dysfunction were noted in any of the patients at the review in clinic.
The evolution of ureterohydronephrosis (posterior-anterior [PA] renal pelvic diameter, ureteral diameter, and T1/2) at 18 months postoperative follow-up and at cohort study is summarized in Table 1.
The US results analysis was completely normal, with absence of pelvic or ureteral dilation in (n=12 children), or minimally dilated (n=11). In the group of patients who presented residual dilation on US, the diameters recorded were <9 mm lower ureter and pelvic dilation <13 mm. This group then went on to renography, which showed no obstructive features in any case (Fig. 4.).

Case 9 of the series. Ultrasonography at 43 months postoperatively.
A minimally invasive approach of POM including endoscopic dilation of the VUJ and endoscopic management of VUR had an initial success rate of 86%.
Discussion
High-pressure endoscopic balloon dilation of the VUJ in children with POM remains controversial despite the fact that some reports have shown favorable 4 –7 results. These reports have focused on the usefulness of this technique as an initial temporary approach to avoid the morbidity associated with open ureteral reimplantation, mostly in small children with severely dilated ureters and small bladders.
The major concerns related to this technique are the possible recurrence of stenosis and creation of VUR.
This study demonstrates that all patients who have good outcome 18 months after the procedure have maintained results, without recurrence of pelviureteral dilatation or urinary tract related symptoms (UTIs, bladder dysfunction symptoms) after 47 months median follow-up.
This study, which is the largest to date, demonstrates the value of endoscopic dilation of the VUJ as both an initial temporary approach and also a definitive measure.
The underlying pathophysiology of POM remains obscure. 10 Nonetheless, serial pre- and postnatal US has elucidated much of its natural history. 11 This suggests that POM may resolve spontaneously in >70% of cases, without any deleterious effect on renal function. 12 Still, there remains a group who do show deterioration of renal function, progressive increase in dilatation, and infectious complications. 13 These do need intervention, typically within the first year of life.
The classic surgical approach has been open ureteral reimplantation (±ureteral tapering). This procedure, however, is often difficult and has significant morbidity with >12% needing repeated surgery and having longstanding bladder dysfunction. 1 Dysfunctional voiding has also been reported as a complication after open ureteral reimplantation, 14 and persistent reflux with associated UTIs has also been reported. 15 Refluxing ureteral reimplant has been described as a more physiologic alternative but carries the same potential risk of secondary damage of the ureter. 16 Urinary diversion with end cutaneous ureterostomy is also a possible albeit temporary option, 2 but has been associated with urosepsis and the need for further surgery.
Insertion of a Double-J stent alone, as an internal diversion, has been used in children with POM. 3 Castagenetti and associates 3 reported satisfactory drainage with no need of tapering after internal drainage in 10 children (5 inserted endoscopically), but at the cost of a high morbidity rate. In almost half the cases, however, no actual reimplant was needed, and renal function was preserved in all.
Carroll and colleagues 17 reviewed 31 children with POM treated with endoscopic placement of Double-J stents. In all but one, there was demonstrable improvement of dilatation and renal drainage. Indeed, in 15 children the hydroureteronephrosis resolved without need for further surgery. Farrugia and coworkers 18 reported that from a series of 19 obstructive megaureters managed by stent placement for a median of 6 months, 56% did not need further surgery. Nevertheless, technical complications with ureteral stent placement in POM has been commonplace for others and an important drawback, 19 with reported significative perioperative morbidity.
Balloon dilation of benign ureteral strictures in adults is an accepted procedure, with good outcomes. 20
Dilation in children with POM as an initial treatment has been shown to have satisfactory results in small series (Garcia-Aparicio and colleagues 7 and Torino and associates 6 ). For example, Anguerri and coworkers 5 reported six infants who showed a significant improvement in renal drainage at a median follow-up of 31 months with no operative morbidity. Experience in infants under 1 year of age with POM and ureteral diameter >15 mm have also been reported by Torino and colleagues, 6 with excellent outcome in six patients after a mean follow-up of 23.8 months.
Also reported has been the experience of endoscopic dilation and endoscopic endoureterotomy for treatment of pediatric patients with POM. 8,21 It is remarkable the successful experience reported in 17 children (age range 3 months–12 years) after a follow-up of 3.2 years by Christman and colleagues. 8 They show significant improvement in ureterohydronephrosis in 12 of their patients, and no evidence of obstruction in the remaining 5 patients, whose US showed moderate improvement.
Indication for intervention in each child (e.g., increasing dilatation, urospesis) was evaluated in an individual basis accordingly with the published selection criteria for intervention. 11,12
We believe that good outcome is dependent on a careful and consistent technique. In our opinion, the initial use of a small guidewire (e.g., 0.014") and the smallest possible semicompliant dilating catheter and minimal nominal diameter of 5 mm are crucial.
When access through the VUJ cannot be achieved, an attempt at repeated dilation, after a few weeks, as proposed by Carroll and associates 17 with Double-J stent placement, could also be a useful approach. Dilation was possible in all cases in which we managed to access the ureter, and is unlike other reports in which long distal ureteral stenosis precluded endoscopic dilation. 8 In our series, two patients had dilation with a 3 mm nominal diameter balloon; both patients had minimal improvement of the ureterohydronephrosis. These two patients underwent a new endoscopic dilation with a 6 mm nominal diameter dilation catheter, and after this second dilation, the outcome was excellent. From this experience, our practice has been to use dilating catheters with a minimal nominal diameter of 5 mm.
Our preference was to insert a Double-J stent, to prevent acute postoperative complications, although this in itself may cause problems. Nevertheless, our case in which dislodgement of the Double-J stent manifested as acute hydroureteronephrosis necessitating open reimplantation suggests this is worthwhile. The experience with Double-J stent placement suggests that this could be useful to prevent complications related to Double-J stent migration.
It may be a factor contributing to the success of the VUJ assessment at Double-J stent removal, because it has been reported in the experience of Garcia-Aparicio and associates. 7 One of main complications of endoscopic dilation appears to be secondary VUR. 4,7 We only requested cystography when dilatation persisted or in those cases of UTIs; therefore, the true incidence is not known. In our series, it appeared to be 5/29 (17%) renal units. Nevertheless, even VUR can also be treated endoscopically as shown in three of our children and in other series. 22,23
The other main bias of our study is the fact that it is a retrospective case review, with the unfortunate lack of an historic cohort to compare, although the cohort study allowed a most accurate analysis of the outcome of our patients. The follow-up shows that these patient results have been stable for the period of study; however, a new cohort study of this series will be valuable.
This and other minimally invasive experiences in dealing with POM create new questions that multicentric studies and long follow-ups should answer in the future, because early results, minimal morbidity rate, and cost-efectiveness are so encouraging. 21
A minimally invasive approach to POM as set out in our series achieved a success rate of >80%, without recurrence or long-term complications. A minimally invasive endourologic approach to children with POM is a feasible procedure, with a very good success rate and with the obvious advantages such as short hospital stay and minimal discomfort, and the complete absence of bladder dysfunction symptoms.
The analysis of our series shows that it can be considered as a temporary treatment for patients with POM, because it is maintained in patients who have a successful outcome. The most important aspect of our study is to show that, in our experience, those patients with a good outcome at 18 months have maintained results, demonstrating the value of high pressure balloon dilation of the VUJ as a definitive treatment option.
Footnotes
Acknowledgment
We are grateful to Prof. Mark Davenport (London) for editing and stylistic appreciation of the manuscript.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.