
Abstract
Background and Purpose:
To investigate the efficacy, safety, and cost-effectiveness of fulguration compared with traditional transurethral resection of a bladder tumor (TURB) among patients who had recurrent lesions after an initial TURB due to bladder cancer.
Patients and Methods:
For the period from March 2001 to January 2012, we reviewed the records of 42 patients who underwent a fulguration procedure for a recurrent Ta small bladder mass after excluding those with ≥1-cm sized masses at recurrence and those with masses at more than three sites. The included fulguration patients were matched with 42 TURB patients who presented with similar preoperative factors. The perioperative outcomes, including complications, recurrence-free survival rate, and total medical cost during each procedure, were compared.
Results:
The mean tumor size was similar between the two groups (0.54 cm in the fulguration group vs. 0.61 cm in the TURB group, p=0.161). During the follow-up periods, 12 patients (28.5%) in the fulguration group and 11 patients (26.2%) in the TURB group experienced tumor recurrence. The recurrence-free survival rate was similar for both groups (p=0.880). The mean total medical cost of fulguration was much cheaper compared with the TURB group (393.3 vs. 1164.6 US dollars, p<0.001).
Conclusions:
Fulguration under local anesthesia for a small-sized recurrent mass is safe and efficacious in properly selected patients. In addition, it also significantly reduces the medical cost and avoids unnecessary anesthesia. Although the two treatments yielded similar oncological results, this finding should be validated in a large-scale, well-designed prospective study.
Introduction
Patients and Methods
Study population
A retrospective cohort study of bladder cancer patients treated between March 2001 and January 2012 was performed to evaluate the perioperative and recurrence-free survival outcomes of two patient groups: recurrent bladder tumor patients who underwent fulguration and a matched cohort of patients who underwent repeat TURB. All patients included in this study had undergone TURB as the initial treatment for Ta bladder tumor. We excluded those patients with T1 stage bladder cancer and muscle-invasive bladder cancer at the initial TURB, those with ≥1-cm sized masses at recurrence, and those with masses at more than three sites. We also excluded those patients with a follow-up period of less than 1 year. All data were obtained from our prospectively maintained, Institutional Review Board-approved database. A total of 42 consecutive fulguration patients were matched with 42 TURB patients who presented with similar preoperative factors, including age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, and tumor characteristics (T stage, grade, tumor size, and history of intravesical treatment).
Fulguration technique
All procedures were performed in an operating room after sterile preparation. All patients were placed in the lithotomy position, and 10 cc of lidocaine jelly was instilled into the urethra of all male patients before insertion of the instrument. In female patients, a cotton bud coated with lidocaine jelly was inserted into the urethra. Antibiotics were not routinely used, and no parenteral sedation or analgesia was used. The single patient who complained of severe pain and discomfort received an intramuscular ketoprofen injection. After introducing a Wolf 19 Fr cystoscope, specimens were taken from all patients at the suspicious recurrence site using the biopsy forceps, and the bladder tumor was fulgurated with a size 4 Fr Wolf fine electrode (Richard Wolf Medical Instruments Corporation, Wimbledon, United Kingdom), which was inserted through the working port.
Outcome analysis
We reviewed the perioperative outcomes—operative time and complications—and compared the outcomes of the two cohorts. We tested the distribution of parameters using the chi-squared test and the Student's t-test. Complications were reviewed for any adverse event occurrences following fulguration or traditional TURB, and postoperative surgical complications were defined according to the Clavien classification system. 11 Tumor recurrence was defined as positive transurethral resection and/or biopsy during the follow-up period. 12 The probability of a recurrence-free survival was estimated using the Kaplan–Meier survival technique, and the log-rank test was used to determine the statistical significance. The total medical cost, including the admission cost for each group, was compared with the Student's t-test. All statistical tests were performed using the Statistical Package for Social Science (version 15.0; SPSS, Chicago, IL). All tests were two-sided with a significance level defined as p<0.05.
Results
A total of Ta 42 patients who underwent fulguration were reviewed and matched to a contemporary cohort of Ta 42 patients who underwent traditional TURB by the same surgeon. The demographic data are summarized in (Table 1). There were no significant differences between the two cohorts with respect to age, BMI, ASA score, or tumor characteristics. A total of 42 patients who underwent fulguration had experienced a mean of 1.3 TURB procedures, whereas patients who underwent traditional TURB had experienced 1.7 previous TURB procedures. The patients with Ta high grade from both cohorts had received Bacilli Calmette-Guerin (BCG) therapy before being included in this analysis to prevent recurrence and progression.
TURB=transurethral resection of a bladder tumor; BMI=body mass index; ASA=American Society of Anesthesiologists; BCG=Bacilli Calmette-Guerin.
As shown in (Table 2), the mean tumor size was similar between the two groups: 0.54 cm in the fulguration group and 0.61 cm in the traditional TURB group (p=0.161). After fulguration, 22 lesions (47.6%) among a total of 42 lesions were found to be either unknown lesions due to an insufficient tissue sample or benign lesions, most of which involved mild dysplasia and BCG granuloma. After traditional TURB, 31 lesions (73.8%) were malignant, and the frequency of malignancy was higher in the TURB group than in the fulguration group (p=0.025). All patients, including those treated with fulguration, received local anesthesia. Among the TURB group, most patients (40/42, 95.2%) underwent spinal anesthesia before the procedure. Two patients required general anesthesia due to failure of the spinal anesthesia and spinal problems. The total procedure time, including anesthesia time was significantly shorter in the fulguration group than in the TURB group (21.8 vs. 61.2 min, p<0.001). All patients who underwent TURB stayed in the hospital for more than 1 day due to the spinal or general anesthesia (mean hospital stay: 1.3 days). However, none of the patients in the fulguration group required a hospital stay. Complications were similar between the two groups. All complications reported in the fulguration group involved the ketoprofen injection used for pain control. After injection of pain-controlling agents, all patients tolerated the procedure well.
During the median 27.8 months of follow-up period, 12 patients (28.5%) in the fulguration group experienced tumor recurrence; 8 patients experienced a recurrence at the same site, and 4 patients experienced a recurrence at a different site or at multiple sites. In the TURB group, 11 patients (26.2%) experienced tumor recurrence during the 25.1 months of follow-up period. The recurrence-free survival rate was similar for both the fulguration group and the TURB group (Fig. 1) (log rank, p=0.880).
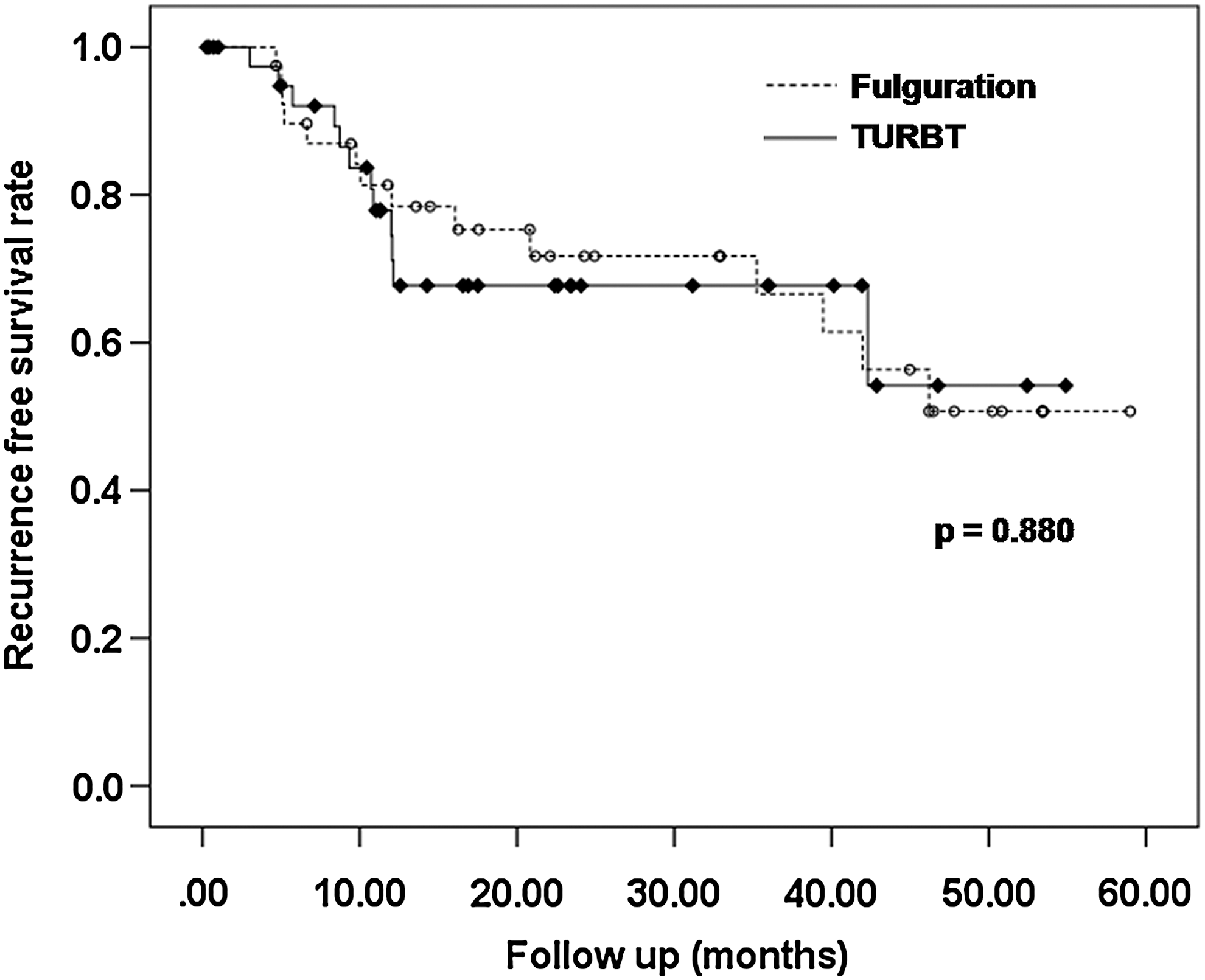
Recurrence-free survival for recurrent small bladder masses after fulguration and traditional transurethral resection of a bladder tumor.
The mean total medical cost of fulguration was much cheaper compared to TURB (393.3 vs. 1164.6 US dollars, p<0.001). In the TURB group, the patients paid much higher medical bills due to the anesthesia and hospital stay.
Discussion
In our study, using the fulguration procedure on men with small recurrent bladder tumors was observed to offer similar tumor control compared with traditional TURB. Meanwhile, fulguration reduced the expense of the procedure by eliminating the hospital stay and avoiding unnecessary anesthesia. Fulguration is a feasible choice for treating small recurrent bladder tumors because all patients who underwent fulguration tolerated the procedure well, with or without painkillers.
Fulguration of small bladder tumors was first reported in 1990 by Herr. 6 They showed that cystoscopy and fulguration were used in the outpatient management of 185 patients, with low-grade and nonmuscle invasive bladder tumors, who were followed for 24 months. This method provided optimal surveillance for recurrence and successful tumor control in selected cases. Bruce et al. 13 showed that many papillary tumors can be removed by suction alone, with diathermy being used sparingly on the base of the tumor, thus reducing patient discomfort. In 1999, Wedderburn et al. 3 showed in their prospective trial that cystodiathermy (another term for fulguration) is a well-tolerated and efficacious treatment for recurrent small papillary tumors of the bladder, and it avoids the need for general anesthesia. Likewise, in our study, fulguration was a well-tolerated procedure in all patients, and it offered similar tumor control during the relative short follow-up period.
More recently, Donat et al. 10 showed that office-based cystodiathermy of small, low-grade papillary recurrences is safe and efficacious in properly selected patients. This approach might improve the patient's quality of life and have a major economic impact on health care. In a prospective study by Donat et al., 10 the recurrence rate of bladder tumors was 46%, and patients who underwent fulguration had a better disease-specific survival rate than patients under surveillance, although this finding was not statistically significant. In our report, the recurrence rate during follow-up (median of 27.8 months) was 28.5%. We consider that this relatively low recurrence rate was the result of two factors. The first was the relatively short follow-up period, and the second was the fact that several benign lesions or unknown lesions were included in our cohorts. In real clinical practice, small masses without a traditional papillary shape are frequently found during bladder cancer follow-up. Often, the mass can be confirmed to be a benign lesion. In addition, many small, low-grade tumors can be safely observed until they exhibit significant growth due to the minimal risk of progression. 14,15 In our report, 47.6% of the fulguration cohort and 26.2% of the TURB cohort were confirmed to have a benign or unknown lesion (due to an unsatisfactory tissue sample). Therefore, fulguration had the advantage of allowing treatment of these nonobvious lesions among patients who had a history of bladder cancer. However, similar recurrence rates despite different malignancy rates were supplementary for a further validation study.
Like previous fulguration studies, our data also showed the benefit of the decreased medical costs of fulguration compared with TURB. In the case of fulguration, patients had reduced hospital medical costs (mean 187.3 US dollars) and related anesthesia costs (mean 584.9 US dollars). Moreover, unnecessary anesthetics are avoided in a group of patients who are at high risk of requiring multiple procedures. Medical staff requirements could also be reduced. During the fulguration procedure, only two members of the staff are required (one doctor plus a resident or nurse), whereas in traditional TURB under spinal or general anesthesia, four or five members of the staff are required (surgeon, anesthetist, anesthetic nurse, scrub nurse, and so on). In addition, the fulguration procedure prevents the unnecessary use of hospital beds and allows operating room space for alternative cases. 5 So ICUD (international consultation on urological disease)–EAU (European association of urology) consultation on bladder cancer 2012 recommend that office fulguration is a good option for patients with a small Ta low-grade urothelial carcinoma of the bladder. 4
Despite our attempts to increase the statistical power using a matched control method, the retrospective analysis was a major limitation of our study. Our study was also limited by a relatively small number of patients in our cohort and the fact that the follow-up was conducted over a relatively short period of time. Another limitation of our study was the low rate of malignant lesions after fulguration or TURB. In spite of the safety afforded by active surveillance for small bladder masses that was noted by Pruthi et al., 15 our protocol may seem to be overtreatment because even nonmalignant lesions are identified and eliminated. However, the presence of questionable lesions in the bladder is a source of stress for both patients and physicians, so fulguration under local anesthesia is an appropriate procedure to use to remove the lesion. Another limitation was that all procedures were conducted in the operating room and not in the office, because procedures in the operating room did not require additional medical costs in this circumstance. However, we recommend the office-based fulguration technique as the technique could be performed easily in the office. 4 And we could not compare the pain scale by an accurate questionnaire because of different methods of procedure and anesthesia; however, after ketoprofen injection, all patients who tolerated during whole procedure were encouraged.
Conclusions
The fulguration under local anesthesia is a safe and well-tolerated procedure among patients with recurrent bladder masses. In selected cases with small bladder masses, fulguration offers a recurrence-free survival rate similar to that of traditional TURB. In addition, fulguration also reduces medical expenses and avoids unnecessary anesthesia. The results of our study should be validated with a larger number of subjects and a longer follow-up period.
Footnotes
Disclosure Statement
No competing financial interests exist. The authors have no conflicts of interest with any institutions or products. No financial support was received by any author.