
Abstract
Purpose:
To evaluate the utility of two ipsilateral ureteral stents placed for benign and malignant ureteral obstruction.
Methods:
We performed a retrospective analysis of all cases of tandem ureteral stent (TUS) insertion at our institution from July 2007 through January 2013. Student t, Fisher exact, and log-rank test were used.
Results:
TUS insertion or exchange was performed in 187 cases. There were 66 patients (75 renal units) who underwent successful TUS insertion. Malignant ureteral obstruction (MUO) was the cause for obstruction in 39 renal units (34 patients) vs benign ureteral obstruction (BUO) in 36 renal units (32 patients). Four patients with BUO and 15 patients with MUO underwent stent exchanges at a mean 145 and 128 days, respectively. Serum creatinine levels were stable poststent placement (P=0.4). Degree of hydronephrosis improved (paired t test P<0.03) after stent placement for both benign and malignant cohorts. TUS placement was noted to fail (flank pain with worsening hydronephrosis or increasing creatinine level) in five renal units with MUO (12.8%) and none with BUO. Stent failure (either conventional or TUS) suggested worsening survival in those with MUO. Median survival for those with MUO and a history of stent failure (10 of 14 died, 71%) was 66 days compared with 432 days for those without a history of stent failure (8 of 20 died, 40%) (log-rank test P=0.007).
Conclusion:
Our experience with the TUS, the largest to date, demonstrated that they are highly successful in both benign and malignant causes of obstruction, comparing favorably with metallic ureteral stents. Stent failure may be predictive for shorter survival.
Introduction
Further, many cases of MUO, and many benign etiologies for ureteral obstruction (BUO) or stricture, are refractory to decompression with the conventional double pigtail ureteral stent. 1 As a result, several new strategies have been developed to better withstand the compressive forces associated with recalcitrant ureteral obstruction. While the literature has recently seen an abundance of reports on the use of metal coil stents, there is very little published experience on the use of tandem ureteral stents (TUS) for the decompression of MUO or other high severity benign obstruction. We explore our experience with the use of TUS in obstructive uropathy, both malignant and benign.
Methods
TUS insertion is performed commonly at our institution. While some variations in the technique have been described, we use a technique similar to the one described by Fromer and associates. 3 Briefly, cystoscopy is performed, and the ureteral orfice (of the obstructed renal unit) is cannulated with a guidewire until its proximal end is coiled within the renal pelvis or upper pole calix. We prefer the use of a Sensor wire (Boston Scientific, Natick, MA) for its soft hydrophilic tip, which can bypass ureteral strictures with less trauma and lower likelihood of perforation, and a stiffer body that is more resistant to slipping out. A dual-lumen catheter is then advanced over this wire, and retrograde urography is performed to delineate the area of stenosis and the renal pelvis. A second wire, typically a super-stiff wire, is advanced through the second lumen of the dual-lumen catheter and advanced until a coil is formed in the renal pelvis. The dual lumen catheter may be advanced past the area of stenosis to assess for and dilate the obstruction and to facilitate easier passage of the second wire.
Thereafter, two 6F ureteral stents are advanced over the two wires and deployed when in the appropriate position, simultaneously. If passage of the two stents is not feasible because of severe stenosis, exchange of the Sensor wire for a second super-stiff wire may be attempted. If subsequent passage is still not feasible, balloon dilation of the previously identified stenotic region may be performed with an 18F Uromax Ultra high pressure balloon (Boston Scientific, Natick, MA). Inflation until the balloon is fully dilated, to a maximum of 20 atmospheres of pressure, is usually sufficient. If passage of TUS is ultimately not feasible, a single 6F to 8F conventional stent is placed, and TUS placement is reattempted at the next scheduled stent change.
Institutional Review Board approval was obtained. A retrospective chart review of all cases performed at our institution between 2007 and 2013 identified those cases in which TUS were placed. Patient demographics including age, sex, and laterality were tablulated along with cause of obstruction, level of obstruction, requirement for balloon dilation, stent duration, stent failure rate, and technical failure rate. Pre- and poststent hydronephrosis, as graded by the Society for Fetal Urology Classification (SFU), 4 and serum creatinine (sCr) level were also listed. Degree of hydronephrosis was based on the latest image prestent and the most recent image poststent, but before subsequent stent exchange, if applicable. Similarly, sCr was based on the most recent value prestent and the most recent value poststent but before subsequent stent exchange.
Renal colic or profound lower urinary tract symptoms, in the absence of worsening hydronephrosis or urinary tract infection, were attributed to stent irritation and tabulated. Follow-up and survival data were also obtained for those with MUO. Cause of death was not obtainable in many cases; hence, survival data were limited to overall survival. Student t test and Fisher exact test were used to compare all continuous and categorical variables, respectively. Kaplan-Meier survival curves were constructed for those patients with MUO. Log-rank test was performed when comparing overall survival as stratified by stent failure history.
Results
Between July 2007 and January 2013, 66 patients (75 renal units) underwent a total of 187 procedures for tandem stent placement or stent exchange; 32 patients underwent a total of 55 procedures using tandem stents for benign purposes and 34 patients underwent a total of 132 procedures for MUO.
There were 32 patients (33 renal units) who underwent a total of 55 procedures for benign causes of obstruction. In these patients, definitive corrective surgery was not feasible because patients were unfit for surgery (inability to obtain medical clearance) or because patients thought that definitive therapy was too risky. Sixteen (50%) patients were male, and mean age was 64 years (standard deviation [SD]=15). Laterality was right in 12 (37.5%), bilateral in 4 (12.5%), and left in 16 (50%) patients. Mean follow-up duration was 28.5 months (median 31.2 months). Causes for BUO necessitating tandem stents were stricture disease in 19 (57.6%), ureteropelvic junction obstruction in 2 (6%), and severe stone disease in 11 (33.3%) of 33 renal units. Level of obstruction was proximal in 13 (41%), mid in 2 (6%), and distal ureter in 17 (53%) patients. Four (12.5%) patients underwent multiple stent exchanges beyond the original placement, ranging from 2 to 11 times. Mean stent duration was 145 days (4.8 months). Tandem stents were placed for failed previous stent placement in seven cases (six were conventional double pigtail and one was a metal coil stent). Balloon dilation was performed in 12 (36%) renal units. Pre- and poststent creatinine (Cr) levels were 2.1 and 2.06 (paired t test P=0.2). Stent irritation was identified in two (6%) patients.
Thirty-four patients (39 renal units) underwent a total of 132 procedures for MUO. Nineteen (56%) patients were male, and mean age was 70 years (SD=15). Laterality was right in 15 (44%), bilateral in 5 (15%), and left in 14 (41%) patients. Mean follow-up duration was 23 months (median 17.4 months). Causes for MUO were cancer of the bladder—11 patients (28 procedures), colon—4 (28 procedures), endometrium—2 (16 procedures), esophagus—1 (3 procedures), stomach—1 (3 procedures), lymphoma—2 (15 procedures), ovary—3 (4 procedures), prostate—3 (4 procedures), uterus—2 (6 procedures), vagina—1 (16 procedures), and cervix—1 (2 procedures). Twenty patients (59% of patients, 103 cases) underwent either chemotherapy or received radiation therapy for their primary malignancy. Level of obstruction was proximal in 6 (15%) patients, mid in 3 (8%) patients, and distal in 30 (77%) patients.
Twenty-eight (72%) ureters needed balloon dilation. Fifteen patients underwent stent exchanges a range of 2 to 16 times. Mean stent duration was 128 days (4.3 months). Fifteen (44%) patients had tandem stents placed for previous stent failure (11 conventional stents and 4 TUS). Ultimately, 5 of 132 (4%) TUS placed failed. Only one (3%) patient ultimately needed percutaneous nephrostomy placement for presumed stent failure; this occurred nearly 10 years after initial tandem stent placement, and was caused by tumor encasing the lower end of both stents. Ten (29%) patients were noted to have stent irritation postoperatively and were treated with a variety of medications including nonsteroidal anti-inflammatory, anticholinergic, or selective peripheral alpha-1a inhibitors. Mean pre- and postoperative sCr level was 1.35 and 1.36, respectively (paired t test P>0.05). Twenty-two of 25 patients with MUO and preoperative Cr >2 demonstrated stable or improved Cr poststent (paired t test P>0.05). Mean SFU grade hydro pre- and poststent was 2.5 and 2.3, respectively (paired t test P=0.02).
Comparing patient and case characteristics for those who underwent tandem stent placement for BUO and MUO revealed several similarities and differences. Both groups demonstrated similar age, ratio of sex, and laterality. Those with MUO, however, demonstrated a proclivity toward a greater proportion of distal obstruction compared with BUO (77% for MUO vs 47% for BUO, P=0.009). Further, patients with malignancy were more likely to undergo balloon dilation (72% for MUO vs 33% for BUO, p=0.004), have a history chemotherapy or radiation (51% for MUO vs 6% for BUO, P=0.0001), or experience stent irritation (29% for MUO vs 6% for BUO, P=0.023). There was also a greater tendency toward proportion of patients needing multiple stent exchanges in the MUO cohort (44.1% for MUO vs 4% for BUO, P=0.07). These results are summarized in (Tables 1A and 1B) for both benign and malignant cohorts.
UPJO=ureteropelvic junction obstruction; pts=patients.
TUS=tandem ureteral stent; PCN=percutaneous nephrostomy.
Survival analysis was performed on those with MUO. Of the 34 patients with MUO, 18 died or were transferred to hospice or palliative care at a median 321 days. Stratified by history of stent failure, 10 of 14 (71%) patients with MUO died during our follow-up compared with 8 of 20 (25%) patients with MUO but without a history of previous stent failure (P=0.09). Further, median survival for those with MUO and a history of stent failure was 66 days compared with a median survival of 433 days for those with MUO but without a history of stent failure. These data are summarized in (Table 2 Kaplan-Meier survival curves for overall survival for all patients with MUO (Fig. 1) and for those stratified by history of stent failure (Fig. 2) were constructed. The log-rank test demonstrated statistically significant better survival for those free of stent failure (P=0.007).
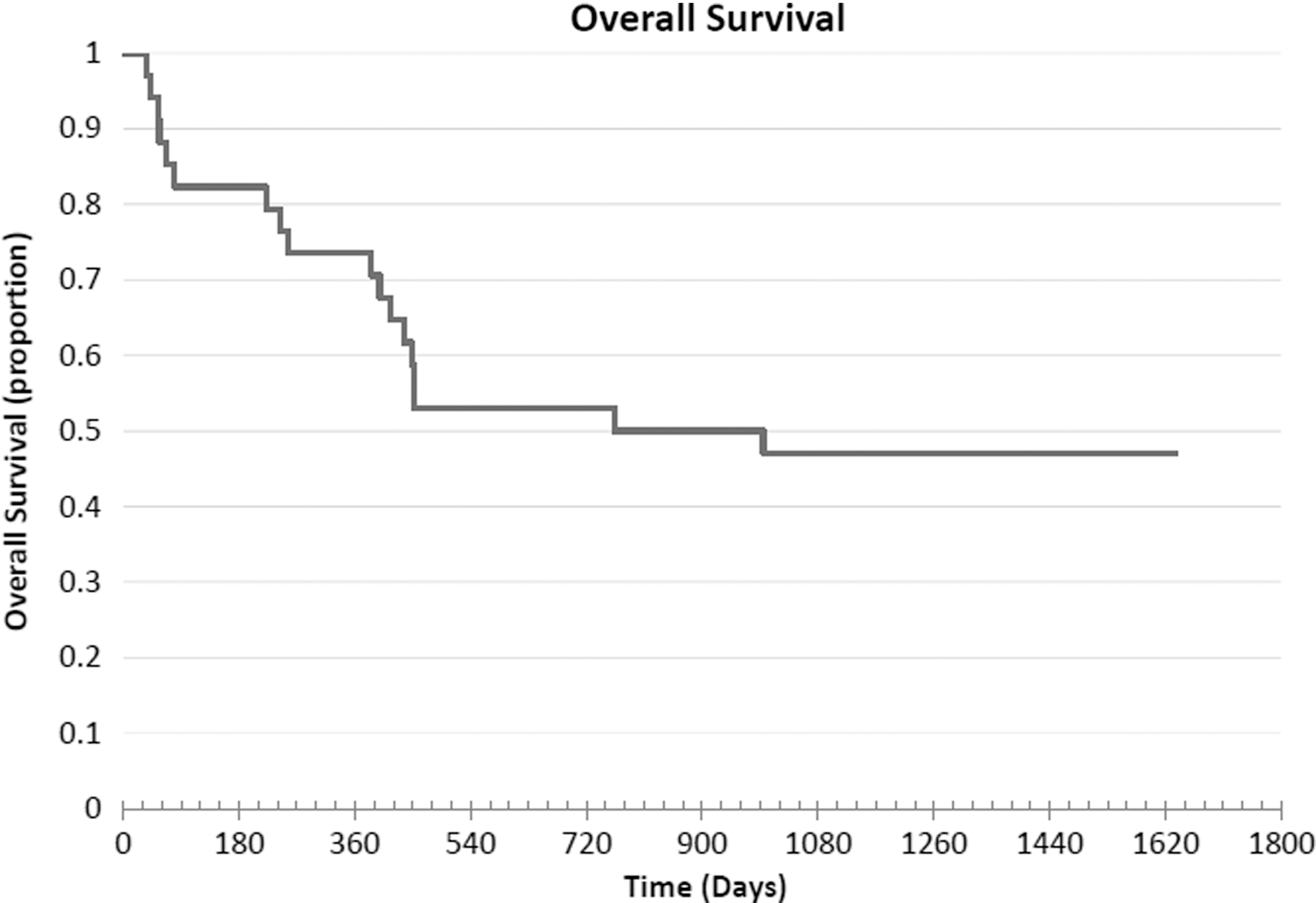
Kaplan-Meier curve for overall survival of patients with malignant ureteral obstruction managed with tandem ureteral stents.

Kaplan-Meier curve for overall survival of patients with malignant ureteral obstruction managed with tandem ureteral stents stratified by history of stent failure.
MUO=malignant ureteral obstruction; pts=patients.
Discussion
Double pigtail ureteral stents have been used for ureteral obstruction since 1967, 5 and several reports have since been published revealing poor sustained patency in MUO with stent failure rates ranging from 16% to 58%. 1,6 –10 As a result, better methods for the decompression of MUO have evolved, including metal coil stents and TUS.
Both metal coil stents and TUS aim to better withstand the presumed compressive forces that overcome conventional double pigtail ureteral stents. Metal coil stents rely on mechanically stronger material and a coil design that allows for buckling of concentric coils to resist kinking and subsequent stent occlusion. 6 TUS offer an additional parallel lumen that may better endure compression. In addition, TUS allow for more extraluminal flow by allowing for more space between the two stents. 3 Both designs have been supported by in vitro studies revealing improved intraluminal and, in the case of TUS, extraluminal flow in the face of compression. 7 –9
Nearly a dozen articless have reported on the clinical outcomes of metal ureteral stents since the original report in 2007 by Wah and colleagues. 10 –17 The reports range in size from 2 to 59 renal units and cite stent failure rates that range from 0% to 100%. Liatsikos and coworkers 18 reported stent failure rate of 0% for MUO in a prospectively observed cohort of 25 with MUO (50 patents overall). They did report, however, encrustation in 12 patients and 9 stent exchanges that were classified as difficult. Interestingly, their BUO cohort experienced a 66% stent failure rate. Besides the report revealing 100% stent failure in two pediatric patients with MUO, 19 most articles suggest a failure rate of approximately 20% to 40%. The most recent publication by Goldsmith and colleagues 14 reported 12 stents of 37 (nearly 33%) that failed at a median of 14 weeks.
Despite it being an older technology compared with metal coil stents, only five articless and one case report have been published on the clinical utility of TUS. TUS were successfully used in the decompression of a kidney with a persistent urine leak that had previously undergone a partial nephrectomy. 20 One publication reported on experience with the use of TUS for BUO, and there were four articles for MUO.
Three of the studies were small retrospective case series evaluating TUS for MUO in a combined total of 16 patients (22 renal units). 3,21,22 Mean follow-up ranged from less than 6 to 16 months. One report described a failure in the initial attempt at placement that was managed with the placement of an 8F conventional stent. 21 Another report detailed no stent failures, complications, or lower urinary tract symptoms, although their cohort of seven had 43% mortality by 3 months. 22 A third small series was notable for the development of significant lower urinary tract symptoms in 40% of their cohort of five and one stent that had to be removed because of pyonephrosis. 3 In another interesting report, placement of a new stent alongside a failed stent in 18 renal units with MUO resulted in slower progress to stent failure compared with stent exchange in 30 renal units. 6
TUS use was described for BUO in a series of 19 patients with ureteral stricture postrenal transplant. 23 The authors cited a patency success rate of 58% at nearly 1 year with TUS and concluded that TUS were feasible for the management of recurrent and recalcitrant ureteral stenosis after kidney transplantation.
Our current study is the largest experience with TUS for any cause with the longest follow-up (28.5 months for BUO and 23 months for MUO). In fact, more renal units were evaluated in this current study compared with all combined previous studies examining TUS. Further, only two studies evaluating metal coil stents for MUO examined more renal units. Our freedom from stent failure (87% for MUO and 100% for BUO) is favorable in comparison with conventional stents and metal coil stents. Mean stent duration was greater than 4 months. By convention, at our institution, these stents are routinely scheduled to be exchanged at 3 to 4 months, although no encrustations were identified in our series and 13 stent exchanges were performed at 6 months or greater without incident. Fifteen cases of 133 (11%) underwent stent exchange sooner than 3 months, although no identifiable cause for early stent exchange was identified other than the five failures. Serum creatinine was stable after stent placement, and hydronephrosis was noted to improve. Complications were not identified in our cohort, and stent irritation occurred in 2 and 10 patients with BUO and MUO, respectively.
Survival has been extensively reported on in MUO, with most reports citing survival of less than 1 year for those undergoing decompression for malignant obstruction. In our cohort, 18 patients (53% of patients with MUO) either died or were transitioned to hospice level of care at a mean of 388 days (range 36 to 1635 days). Stent failure suggested worsening overall survival and shorter survival. Of the patients with MUO, 14 experienced stent failure whereas 20 never experienced stent failure. Ten patients of the 14 (71%) who had MUO and previous stent failure died at a median 66 days. In contrast, only 8 of 20 (40%) patients with MUO but without stent failure died at a median 433 days. While comparison of the proportion of death in each group only showed a tendency toward significance (P=0.09), survival duration was significantly shorter in the stent failure group (P=0.03). Further, Kaplan-Meier survival analysis demonstrated a significant survival benefit in those without a history of stent failure (P=0.007).
Our results are similar to most reports in suggesting survival of approximately 1 year for those with MUO. Izumi and associates 1 demonstrated that many of the factors that predicted stent failure were significant for overall survival, but a direct link between stent survival and overall survival was never claimed. Our report suggests that tandem stent failure portends a poorer overall survival prognosis.
Our study has several limitations. The heterogeneity of the etiologies of obstruction certainly play a role in the success (or failure) of TUS and may preclude accurate comparison with other studies that may not have the same distribution of causes of obstruction. This heterogeneity also limits our ability to perform robust statistical analysis because it necessitates grouping of what may be heterogeneous parameters into broader categories for statistical comparison. Nonetheless, we report the largest series on the use of TUS and their outcomes. With many publications citing the merits of metal coil stents, critical evaluation of such technology must be checked against other existing options.
The need for stent exchange every 4 months may be associated with increased cost and exposure to anesthesia-related side effects and risks. While one report suggests that metal stents may offer a cost savings of 50% to 75% annually ($6000×3–6 exchanges per year for conventional polymeric stent placement vs $9500 for a single yearly exchange for metal stents), 24 this may be limited to those patients without complications and with sufficient survival. Our series has not demonstrated the complication rate seen with metal stents, and it is likely that tandem stents can be changed at a greater interval than in our series. TUS insertion does require an additional stent with each placement and often a ureteral balloon dilator on initial placement, but these costs account for less than 1% each of the above mentioned cost per stent placement or exchange (data for cost of each item obtained from hospital administration).
Conclusion
The placement of two ipsilateral polymeric stents is highly successful for the decompression of profound ureteral obstruction caused by benign and malignant etiologies. In our experience, TUS placed in those with MUO demonstrate a greater need for balloon dilation for initial placement, greater stent-related symptoms than those with BUO, and less freedom from stent failure. Stent failure with TUS (13% for MUO and 0% for BUO) compares favorably with reported rates of success with metallic ureteral stent decompression (20%–40% for MUO). Stent failure in our cohort suggested increased likelihood of mortality and shorter overall survival. Further evaluation with a multi-institutional, randomized, prospective study is necessary to properly compare TUS with metal ureteral stents.
Footnotes
Disclosure Statement
No competing financial interests exist.