
Abstract
Objective:
The purpose is to report our 10-year experience with surgical management of large or symptomatic adrenal myelolipoma.
Patients and Methods:
Patients receiving surgical treatment for adrenal myelolipoma between December 2001 and September 2011 in our institution were retrospectively reviewed. Patients were divided into two groups: open surgery and laparoscopic surgery. Patient demographic data, lesion size evaluated by computed tomography scan or magnetic resonance imaging, operation time, blood loss, time of returning to diets, perioperative complications, and length of hospital stay were collected and analyzed.
Results:
Forty patients (14 received open surgery and 26 received laparoscopic surgery) were enrolled in our study. Both procedures were successful and no patient in the retroperitoneal laparoscopic group required conversion to open surgery. The mean age of the patients was 52.7 years. The median size of the tumor was 5.0 cm. Forty-three percent of patients suffered from lumbago. There was no statistical difference in perioperative complications between the two groups (p>0.05). Retroperitoneal laparoscopic adrenalectomy patients had a shorter operation time (90.66±37.97 min vs 141.82±62.78 min, p=0.017), less blood loss (150, 100–200 mL vs 450, 300–525 mL, p=0.000), earlier time of returning to diets (2, 2–3 days vs 3, 2–4.5 days, p=0.036), and a shorter hospital stay (6, 5–7 days vs 10, 8–11.25 days, p=0.000) when compared with open surgery patients.
Conclusion:
Both open and laparoscopic surgeries are efficient and safe treatments for large or symptomatic adrenal myelolipoma, and retroperitoneal laparoscopic surgery has the advantages of minimal invasion and rapid postoperative recovery.
Introduction
A
Adrenal myelolipoma was invariably found through autopsy until 1980s, with a relatively stabilized prevalence of 0.08%–0.2%. 2 More and more adrenal myelolipomas have been detected since the wide application of modern imaging techniques. The highest prevalence has reached 8%–15%. 3,4
Open surgery used to be the only choice for patients, with adrenal myelolipoma, who were not suitable for conservative treatment, and some cases of adrenal myelolipomas removed by laparoscopic surgery were reported in the recent years, 5 –7 while large-scale studies in this area were still lacking.
The aim of our study was to further investigate the efficacy and safety of surgical managements of adrenal myelolipoma, providing more valid evidence in treating adrenal myelolipoma.
Patients and Methods
Study design and patients
A retrospective study was conducted to investigate the efficacy and safety of retroperitoneal laparoscopic vs open surgery for treatment of adrenal myelolipoma. From December 2001 to September 2011, the medical records of myelolipoma patients who underwent surgical treatment in the Shanghai Changzheng Hospital were reviewed. Patients meeting the following criteria were included: (1) patients with primary myelolipoma and confirmed by pathology postoperation; (2) tumor size larger than 4 cm or patients having obvious lumbago; (3) the tumor was removed either by open or retroperitoneal laparoscopic operation at our center. Two primary reviewers collected all the data independently.
Clinical data
Demographic data were obtained at the time of admission. The size and location of the lesion, operation pattern, operation time (min), blood loss (mL), time of returning to diets (day), length of hospital stay (day), and complications were obtained postoperatively.
Surgical procedures
Preoperation preparation
The tumor characteristics and surgical options were determined according to the imaging results preoperatively. Endocrine evaluations were conducted to eliminate the possibility of functional adrenal tumor. No biopsy was performed preoperatively. Blood pressure was adjusted to normal level.
Open surgery
With the patient lying in a supine position after general anesthesia, an intercostal incision or transrectal incision was applied. The perinephric fat at the upper pole of the kidney was removed to expose the adrenal gland and the tumor. Afterward, dissect along the adrenal gland and the upper pole of the kidney surface until the adrenal vein was identified. Ligate and cut the adrenal vein, and then resect the adrenal gland and tumor en bloc.
Retroperitoneal laparoscopic surgery
After general anesthesia, the patient was placed in the contralateral position. The standard 3-port retroperitoneal laparoscopic approach was performed (Fig. 1). A vertical 1–2 cm small incision (A point) was done at the posterior axillary line subcostally, the lumbodorsal fascia was blunt dissected using long curved forceps. The index finger of the surgeon probed into the retroperitoneal space and the peritoneum was pushed aside. A balloon was put into the retroperitoneal space and inflated to 800 mL to dilate the space. The surgeon's index finger probed into the dilated space again and, with the help of this finger, incisions at the anterior axillary line, below the costal margin (B point) and at the midaxillary line, 2–3 cm above the iliac crest (C point) were made (Fig. 1). A 10 mm, 5 mm (10 mm for right-sided tumors), and 10 mm trocar was introduced, respectively. The A and B points were for instruments and manipulation, while the C point was for the camera. CO2 insufflation was commenced and maintained at 13–15 mmHg. After cleaning the extraperitoneal fat, the Gerota's fascia was incised. Dissected along the psoas muscle, from the lower edge of the diaphragm to the upper edge of the iliac fossa, the periadrenal fat and the fat surrounding the upper pole of kidney were then removed. When the adrenal gland and tumor were exposed, skeletonize the tumor along its surface. Dissect the tumor according to the tumor size and its relationship to the surrounding tissues: small, well-defined, and surficial tumors could be simply removed without controlling the adrenal vein, otherwise, if the tumor was too large and with severe adhesions to the adrenal gland, the adrenal vein was controlled first by a clip and the tumors were resected en bloc with the adrenal gland.
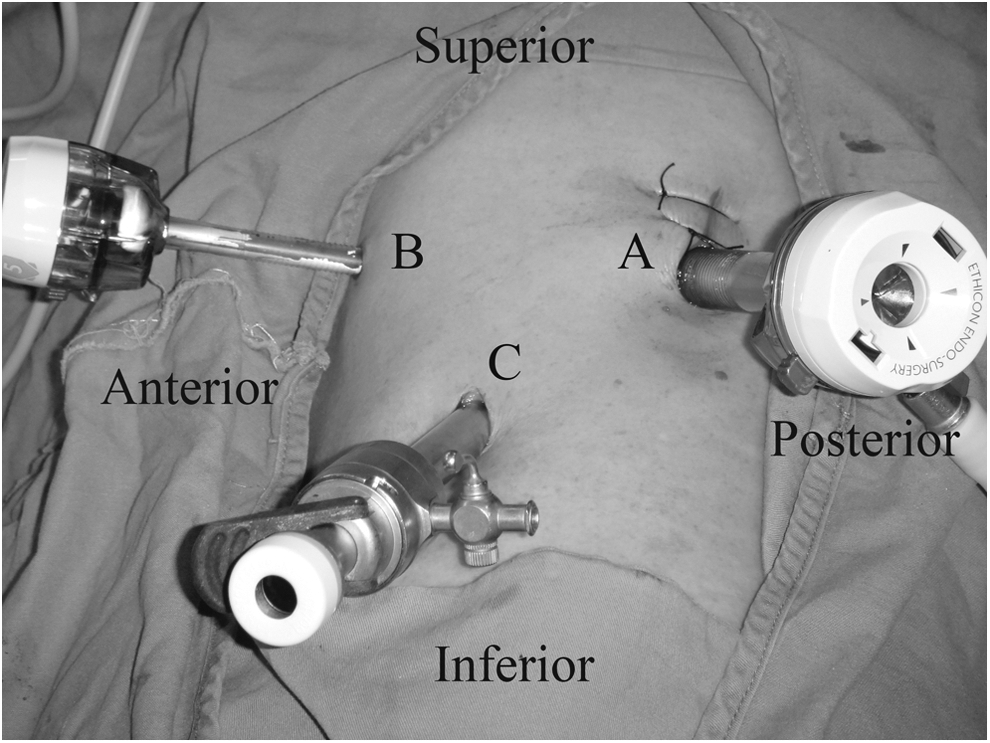
Trocar positioning. The patient was placed in contralateral position. C: 10 mm trocar for camera; A: 10 mm trocar for the laparoscopic harmonic scalpel; B: 5 mm trocar for other instruments.
Statistical analysis
The two-tailed Pearson Chi-square test or corrected Chi-square test was applied to evaluate the differences of categorical variables between groups. The Student's t test was used to evaluate normal continuous variables. The Wilcoxon rank-sum test was used to evaluate non-normal continuous variables. All statistical analyses were conducted using PASW statistics 18.0 software. p<0.05 was considered as statistically significant.
Results
Demographic and clinical characteristics
In all, 40 patients were enrolled into our study, including 15 males and 25 females. The mean age of the patients was 52.7 years (standard difference, SD: 11.08). The mean body mass index (BMI) was 22.83 (SD: 2.65). Fourteen patients received open surgeries and 26 received retroperitoneal laparoscopic surgeries for adrenal myelolipoma. There was no conversion in the retroperitoneal laparoscopic group. Thirty-eight surgeries were performed by urologists, while two performed by surgeons from the Department of General Surgery.
Thirty-one (78%) tumors were located in the right adrenal region, while 9 (22%) in the left. The median size of the tumor was 5.0 cm (QL–QU: 4–6.75). Ten (25%) tumors were larger than 6 cm (Table 1).
BMI=body mass index; SD=standard deviation; QL=lower quartile; QU=upper quartile.
Perioperative data
The average operation time of retroperitoneal laparoscopic surgery was significantly shorter compared with open surgery (90.66±37.97 min vs 141.82±62.78 min, p=0.017). Intraoperative blood loss favors the laparoscopic surgery group (150, 100–200 mL vs 450, 300–525 mL, p=0.000). Table 2.
The overall incidence of postoperative complications was 10%, including 1 pulmonary edema, 1 postoperative bleeding in the open surgery group and 1 chyluria, 1 postoperative bleeding in the laparoscopic surgery group. There was no significant difference in complications between the two groups (14% vs 8%, p=0.507). Table 2.
The time of returning to diets favors retroperitoneal laparoscopic surgery group (3, 2–4.5 days vs 2, 2–3 days, p=0.036). The hospital stay was shorter in retroperitoneal laparoscopic surgery group than that in open surgery group (10, 8–11.25 days vs 6, 5–7 days, p=0.000). Table 2.
All specimens were confirmed myelolipoma by pathological examinations postoperatively, including 8 cases in the open group and 10 cases in the laparoscopic group accompanied with hemorrhage and necrosis.
Follow-up data
The follow-up time was 3 months to 10 years (mean time was 2 years). The patients were all asymptomatic, with normal blood tests. Ultrasonography (US) and computed tomography (CT) revealed no recurrence and canceration.
Discussion
Adrenal myelolipoma is a kind of benign tumor with unclear etiology. It is generally believed that, metaplasia of adrenocortical cells caused by the response of adrenal capillary reticuloendothelial cells to necrosis, infection, and stress was the direct force initiating the growth of myelolipoma. 8
Myelolipoma accounts for 3%–5% of primary adrenal masses. 9,10 Most reported tumor sizes were under 4 cm, ranging from 1 to 14 cm, larger tumors are rarely seen. 11 Patients with adrenal myelolipoma are usually asymptomatic. However, when the tumor is large, accompanied with hemorrhage or other changes, symptoms such as abdominal pain might emerge. In the present study, nearly half of the patients were admitted due to lumbago and abdominal pain.
Most asymptomatic tumors could be found by imaging techniques. US is considered as the preferred method for screening. The CT performance of myelolipoma is characterized as a well-defined mass with fat-containing components, mixed with myeloid tissues at various scales. CT is also very sensitive to intratumoral calcifications and hemorrhages. Magnetic resonance imaging (MRI) has its unique advantages over US and CT. The three-dimensional positioning data from MRI can provide the tumor extent as well as the relationship between the tumor and adjacent organs, thus facilitating the selection of surgical incision and operation procedure. 12 Usually, adrenal myelolipomas do not cause endocrine disorder. However, myeloid tissues can also be found in specimens from patients with functional adrenal gland diseases such as Cushing's syndrome. In this case, the hormone level might be abnormal. 13 –15 Thus, for differential diagnosis, routine endocrine tests are necessary for adrenal myelolipoma patients.
The options for the treatment of the adrenal myelolipoma include conservative management and surgical resection. As a noninvasive treatment, conservative management could avoid surgery-related complications; however, it is no use to relieving symptoms, which could be solved through surgical resection. Besides, surgical management could also reduce the risk of hemorrhagic shock caused by spontaneous rupture, and what is more, no recurrence was reported after surgery. The indications for surgical resection remain controversial. Some believed that operation should be suggested to patients whose tumor was larger than 4 cm. 15 Whereas others argued that if the tumor diameter was less than 10 cm, abdominal US or CT should be given every 1–2 years, otherwise, operation should be suggested, because larger myelolipomas are linked to increased risks of hemorrhage and hemorrhagic shock. 16 In our study, around 50% of patients were admitted due to lumbago, and postoperative pathology also revealed a higher rate of tumor hemorrhage.
Open surgery used to be the unique surgical option. For larger tumors, the ipsilateral adrenal should also be removed together with the tumor. Laparoscopic surgeries have been the gold standard for adrenal diseases since 1990s. Adrenal myelolipoma is a relatively rare disease, from case reports to original research, more and more publications described the efficacy and safety of laparoscopic surgery for treatment of this lesion. 5 –7,17
Tumors larger than 6 cm used to be the contradiction for laparoscopic adrenal surgeries; however, this has changed due to the accumulation of experience in laparoscopic adrenal surgery. 18,19 In this study, 10 patients with a tumor larger than 6 cm received laparoscopic surgeries, and no increased risk of bleeding and other complications were found. For larger tumors, several laparoscopic technical points need concern. The vessels of the right adrenal are short, more attention should be paid to protect the inferior vena cava from tearing when dissecting, and for the tumor located in the left, the relationship between the tumor and the tail of pancreas or spleen should be noted in case of pancreas and spleen damage. Meanwhile, injuries to the kidney and its blood vessels should also be avoided.
Many studies have been carried out to compare transperitoneal and retroperitoneal laparoscopic surgery for treatment of adrenal diseases. The transperitoneal route could provide a larger working space and better view of anatomical landmarks for surgeons, while the retroperitoneal approach, on the other hand, provides direct access to the adrenal gland and allows extraperitoneal dissection without bowel manipulation and, both trans- and retroperitoneal approaches can yield satisfactory surgical outcomes in experts' hands. No significant difference was found in major indicators between the two surgical routes. 20,21 It is reported that the prognosis of myelolipoma is good. In our study, the longest follow-up time was 10 years, no recurrence and canceration were observed.
Conclusion
Both retroperitoneal laparoscopic and open surgeries were efficient and safe for treatment of large or symptomatic adrenal myelolipoma, retroperitoneal laparoscopic surgery has the advantage of minimal invasion and rapid recovery.
Footnotes
Disclosure Statement
No competing financial interests exist.