
Abstract
Background and Purpose:
Urologists are becoming increasingly aware of the importance of pretreatment percutaneous renal biopsy of small renal cortical neoplasms. A barrier to the routine performance of ultrasonography-guided percutaneous renal biopsy has been the technical challenges associated with the procedure. We evaluated a new modified needle, which incorporates an echogenic needle tip designed to improve the needle tip's visibility under ultrasonographic visualization. We evaluated and compared the ultrasonographic imaging quality of the echogenic needle (EN) and a standard needle (SN).
Methods:
Forty-eight participants were recruited to perform ultrasonography-guided needle targeting and drainage of a simulated cyst within a phantom model. The simulated cysts were embedded in an opaque gel mold. Each participant was blinded to the type of needle being deployed and was asked to identify and aspirate the simulated cyst with each needle under ultrasonography guidance. Each needle was tested at three ultrasound-aiming angles, (0, 15, and 30 degrees). The quality of needle visibility under ultrasonographic imaging was assessed via a questionnaire, including needle preference and a visibility score (1–10) at each aiming angle. Participants were stratified by level of ultrasound experience.
Results:
For each angle tested, the EN received higher visibility ratings. The mean visibility scores for the EN vs the SN were 6.44 vs 5.52 at 0 degrees (P=0.001), 7.77 vs 6.96 at 15 degrees (P=0.0004) and 8.33 vs 7.54 at 30 degrees (P=0.0001). Participants reported significantly greater comfort using the EN needle compared with the SN (P=0.001). These results held true regardless of the sequence of needle tested first. Also, there was a significant difference in visibility scores by angle (P=0.0001). Larger angles (30>15>0) resulted in higher scores.
Conclusions:
In this in vitro trial, the application of the EN improved needle visibility for users of all levels of experience. Clinical correlation is pending.
Introduction
A novel ultrasound transducer (Preirus system, Hitachi Aloka, Mitaka-shi, Tokyo, Japan) facilitates needle deployment through an intuitive system incorporating a perforated transducer probe, which allows the needle to pass directly through it. A virtual dotted line of the needle path is projected on the ultrasonography screen. This system is familiar to urologists because it is similar to the virtual dotted line, which makes targeting in prostate needle biopsies intuitive in nature. Previous testing in our laboratory has documented that this facilitated ultrasound targeting (FUT) technology allows even inexperienced ultrasound users to accurately deploy needles with precision. 7 While we have previously documented the intuitive nature of FUT, users noted that the exact position of a standard needle tip could still be difficult to discern.
As such, we evaluated a modified needle design, which incorporates an echogenic needle (EN) tip (Echotip, 18-gauge, Cook Medical, Spencer, IN) and compared it with a standard needle (SN) design (Trocar Needle, 18-gauge, Cook Medical, Spencer, IN) for renal targeting. Theoretically, the enhanced visualization conferred by the Echotip may facilitate precise needle placement to achieve a safer percutaneous access to the kidney. We examined and compared the ultrasonographic imaging quality of the EN and a SN to assess the efficacy and visibility of each needle for operators of varying levels of ultrasound experience. In addition, we evaluated the influence of different insonation angles with regard to the visibility of the needles.
Methods
All studies were performed with approval from our internal Institutional Review Board. Phantom models consisting of Metamucil© (The Procter & Gamble Company, Cincinnati, OH), Knox gelatin© (Kraft Foods Group, Inc., Glenview, IL), and water were used. The models created an echogenic medium that simulated kidney parenchymal tissue in sonographic texture, needle resistance, and visual opaqueness. Six water balloons (Ankyo Development Ltd., Kowloon, Hong Kong) simulating cystic lesion targets were embedded within the opaque mold. Targets were standardized by using a 10 mL syringe to infuse approximately 2 mL of blue dyed water into each balloon. The blue dye helped to serve as a visual cue for a successful puncture because blue dye was released when the needle stylet was removed.
A total of 48 participants of varying levels of ultrasound experience were recruited to perform UG needle targeting using the phantom models (Fig. 1). Subjects' level of training, experience with ultrasound, specialty, and hand dominance was documented before performing needle targeting. Using the FUT's novel transducer probe, participants identified and deployed each needle into the “cyst” under ultrasonography guidance. Subjects were blinded to the type of needle being deployed, and the sequence of needle testing was randomized for each user using a random number generator. Once the balloon was punctured, the needle stylet was removed, and a 10 mL syringe was used to aspirate the blue dyed fluid. Each subject ultimately targeted all six “lesions” in the phantom model by deploying both the EN and SN at the three ultrasound-aiming angles, which the FUT probe allows: 0, 15, and 30 degrees. Subjects were also asked to assess needle visibility at each different angle (Fig. 2).
Needle targeting setup using kidney phantom model with Echotip needle (left) and standard needle (right).
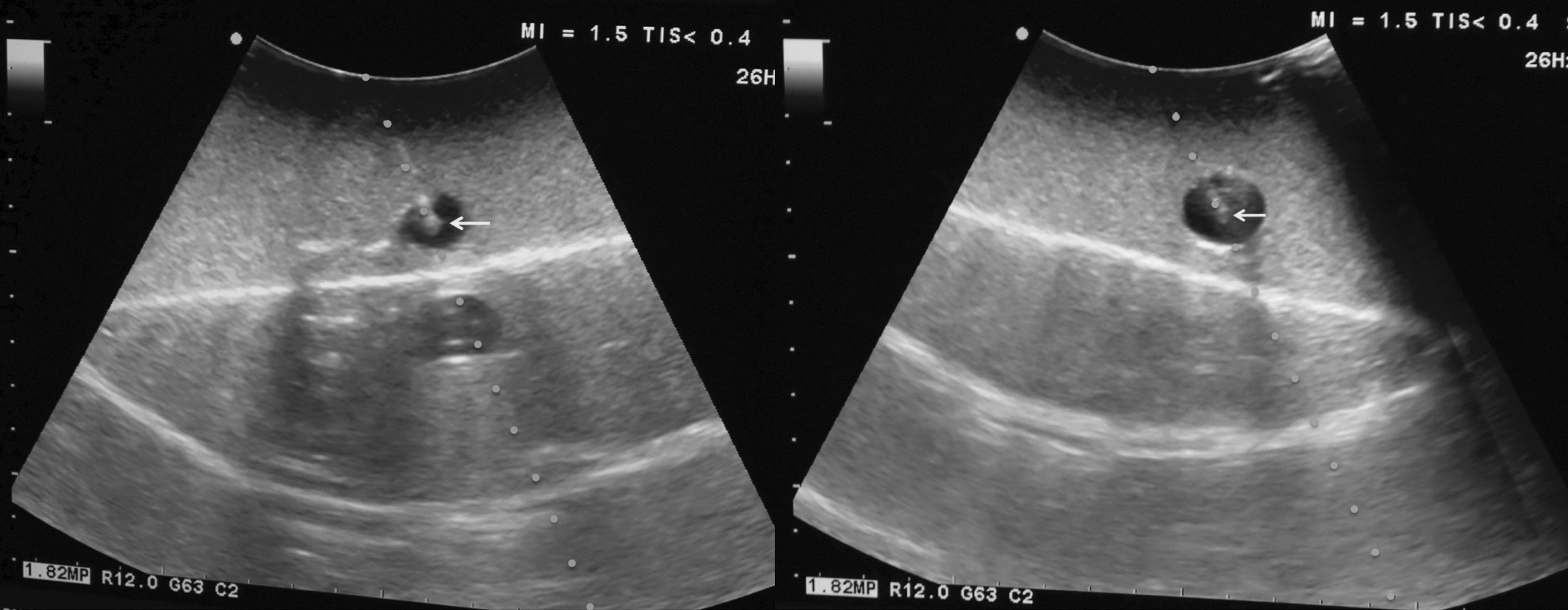
“Cyst” aspiration at an insonation angle of 30 degrees using the Echotip needle (left) and standard needle (right). Arrow in figure depicts location of needle tip.
Scoring was performed using a questionnaire, which included a visibility score from 1 (poor visibility) to 10 (excellent visibility) at each angle. Overall needle preference on completion of all tasks was also asked. Subjects evaluated their comfort level for each needle during the task on the following five-point scale (1–5): 1, not at all comfortable; 2, somewhat comfortable; 3, comfortable; 4, very comfortable; 5, able to use with full proficiency. On completion, participants were stratified by level of ultrasound experience. As a pilot study, no formal power analysis was performed. Rather, we recruited as many subjects as possible of different levels from our institution. Statistics were conducted via a matched pairs t test and a repeated measures analysis of variance to compare the visibility scores at each different angle as well as needle preference. An allowable error of 5% was considered significant.
Results
Of the 48 participants, there was a median of 1 to 2 years of ultrasound experience. Participants included 10 undergraduates, 11 medical students, 12 residents, 6 fellows, and 9 attending physicians. Subjects were stratified by ultrasound experience into four groups: Ultrasound naïve (no experience), 1 to 2 years, 3 to 6 years, and experienced ultrasonographers: More than 6 years of experience. The groups were established rather arbitrarily so that we could stratify participants into relatively similar sized groups. Of the subjects, 19/48 (39.6%) reported having no previous ultrasound experience, 9/48 (18.8%) had 1 to 2 years, 11/48 (23%) had 3 to 6 years, and 9/48 subjects (18.8%) had more than 6 years of ultrasound experience. Among postgraduates, there were 3 radiologists, 2 emergency medicine physicians, and 17 urologists. Of the experienced category, 66.7% (6/9) have performed more than 51 ultrasound cases per year. All subjects successfully targeted the six embedded simulated cysts within the kidney phantom models.
Needle tip visibility was subjectively rated significantly higher at each angle when the EN needle was compared with the SN using a matched pairs t test (Fig. 3). When stratified by years of experience, the sum visibility scores for the EN and SN are significantly different (P=0.0001). There is no difference observed between scores reported for the respective needle type across experience years (P=0.1594), however, demonstrating that level of ultrasound experience does not affect subjective visibility scores (Table 1). With regard to the angle of insonation, there is a significant difference in visibility between the different angles (P=0.00005), with superior visibility at increasing angles (30>15>0). The difference between angle visibility varied significantly with experience, with the greatest visibility differences between angles observed by participants with the least amount of experience (P=0.0318).

Comparison of mean visibility scores between needle types at different angles of insonation. When tested to see if there is a significant difference in visibility by angle using repeated measures analysis of variance with two repeated measures (angle and tip type), there is significantly better visibility (P=0.0001) with the EN compared with the SN and with increasing angle (P<0.00005). Error bars represent±standard error.
EN=echogenic needle; SN=standard needle; LS=least squares; SE=standard error.
Scores differ significantly by needle type (P=0.0001).
Furthermore, participants reported significantly greater comfort using the EN compared with the SN (P=0.001) (Table 2). User's comfort by needle type differed significantly across experience categories (P=0.0144), with the greatest difference in comfort level reported by the most experienced group. Of note, these results held true regardless of the sequence of the needle tested.
Comfort is significantly higher for the echogenic needle (EN) than for the standard needle (SN) (P=0.0012).
LS=least squares; SE=standard error.
Discussion
Difficulty in achieving optimal needle visualization continues to be an obstacle for safe and successful needle deployment in UG procedures, especially when target lesions are small and deep in the tissues. 1,3 Often, practitioners rely on the visible portion of the needle and tactile feedback of nearby tissues during insertions to estimate the needle location. 3 Previous studies using models for vascular access and percutaneous nerve blocks have demonstrated that echogenic enhancements can confer an increase in needle visibility. 8 –10 Various modifications reported for optimizing the visualization of the needle tip under UG include polymeric coatings, dimpling, and roughing of the needle surface. 4 Theoretically, these various innovations should help to optimize the reflection received by the probe by creating a larger reflective surface for the sound waves to scatter or, as in the case of polymeric coating, by trapping microbubbles of air. 1,3,8 The EN tested includes scoring of the needle tip and hundreds of microscopic dimples on the needle surface to enhance echo reflectivity.
In the current study, for all levels of experience, the subjective evaluations demonstrated that EN improves needle visibility compared with the SN. Quantitative photodensity measurements made in the literature using arbitrary echogenic units (EU) support this finding by revealing that the echogenicity of dimpled needle tips (834 EU) is significantly greater than that of a SN (468 EU). 9,10 As such, the EN shows promise in improving efficacy and precision during needle targeting irrespective of the skill of the operator. Indeed, the superior visibility of the EN promotes safer scanning techniques by reducing the likelihood of making subtle movements to maintain the needle's visibility 8 and allowing the operator to only advance the needle tip under precise real-time monitoring. 2
With regard to differences in angles, we found that visibility improved with increasing angle of isonation, a finding consistent with the literature. 8 –11 Similar results were found using a free-hand targeting approach with a needle to probe angle of 55 to 60 degrees providing optimal needle visibility. 11 Indeed, previous investigators have demonstrated that smaller angles of insonation compromise the imaging quality of all types of needles. When a standard smooth needle was tested at a suboptimal insertion angle, the needle visibility was reduced to a level below the “good visibility threshold” 8 –10 ; however, with the modifications of the Echotip needle, consistent visibility at clinically important angles has been observed. 10 Given that achieving an ideal angle is often complicated by suboptimal conditions rendered by patient anatomic abnormalities or overlying structures such as bone, 12 use of the EN may prove particularly beneficial because the clinician may be better served with a needle tip that is more easily localized.
A weakness inherent to the present study is the different appearance of the two needles, which could potentially provide a source of bias for more experienced participants. We did not disclose which needle was which to the participants, however, and we do not believe that most noticed. Furthermore, application of the technology in an in vitro environment presents another limitation to the study. In a clinical setting, the different echogenicity of human parenchymal tissue may yield greater or less visibility of the access needle compared with the phantom model. 13 Nevertheless, the increased visualization of the EN at all three tested angles in vitro may have great clinical relevance, because it may compensate for unfavorable scanning conditions as well as improve procedural ease and the comfort level of its operator. Certainly, clinical correlation of these findings will be important to confirm the results of this in vitro study.
While there are many examples of how the EN technology could facilitate UG procedures, one specific application is in PCNL. During PCNL procedures, enhanced needle visibility is fundamental in achieving end-calix puncture success and could help to reduce bleeding after dilation of the PCNL tract. 5 This, in turn, could improve operative field visibility during subsequent endoscopic procedures, improve stone clearance, and reduce the risk of postoperative bleeding and other complications arising from percutaneous procedures. Further application of this technology for biopsy of renal cortical neoplasms could potentially improve safety and reduce patient morbidity by reducing the number of passes into the targeted lesion, and improve diagnostic yield through precise targeting.
Conclusion
In this in vitro trial, subjective evaluations demonstrated that the EN conferred greater visibility at all angles tested and improved the user's comfort compared with the SN. The EN, when used in combination with the FUT, may help the urologist reduce the technical difficulties with UG needle deployment and increase the adoption of UG procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.