
Abstract
Purpose:
The recovery of potency following radical prostatectomy is complex and has a very wide range. In this study, we analyzed in detail the precise pattern of recovery of potency following robot-assisted radical prostatectomy (RARP).
Materials and Methods:
Prospectively collected database of patients with a minimum follow-up of 1 year after RARP were evaluated retrospectively. Of 503 patients identified, 483 patients completed the sexual health inventory for men (SHIM) preoperatively and postoperatively every 3 months for the first 12 months. Overall potency, usage of phosphodiesterase type-5 (PDE-5) inhibitors, and return to baseline erectile function were evaluated. Potency was defined as having erection that is sufficient for sexual intercourse more than 50% of attempts, while quality potency was defined as being potent without the use of PDE-5 inhibitors.
Results:
Preoperatively, the overall potency and quality potency rate were 67.1% and 48.1%, respectively. Postoperatively, the overall potency rate was 61.4%, while the quality potency rate was 37.2%. In multivariate regression analysis, independent predictors of potency recovery were young age (<60), preoperative potency status, and bilateral preservation of neurovascular bundles (NVBs). In men with SHIM>21, the overall potency and quality potency rate were 79.7% and 41.2%, respectively. More importantly, only 21.4% of the men with normal erection preoperatively (SHIM>21) returned to baseline erectile function (SHIM>21) 12 months after surgery.
Conclusions:
This study indicates that young age (<60), preoperative potency, and bilateral preservation of NVBs were positive predictors of potency recovery following RARP. However, an overwhelming majority of men experience a deterioration in the overall quality of erection after RARP.
Introduction
P
Postprostatectomy sexual dysfunction is the most common complication in these patients affecting their quality of life and sense of well-being. 6 Despite advances in surgical techniques in the era of robot-assisted radical prostatectomy (RARP), ideal management of these patients continues to remain a challenge. Several factors contribute to the postprostatectomy potency, including pre-existing erectile dysfunction, medical comorbidities, surgeon techniques and experience. 6 –8 Age is one of the most important determinants of erectile function. 9 For instance, a patient in his 40s undergoing a bilateral nerve sparing procedure is twice as likely to maintain potency as compared to a patient in his 70s. 6
Pathophysiology of postprostatectomy erectile dysfunction suggests that injury to cavernosal nerves leads to neuropraxia and cavernosal hypoxia. 10 The subsequent collagen accumulation and fibrosis results in cavernosal veno-occlusive dysfunction. 11 Therapeutically, maintaining regular oxygen-rich blood flow to corpora seems to promote smooth muscle integrity and prevent fibrotic changes. 10,11 Multimodal strategies have been advocated as means to promote return to baseline sexual function. Such penile rehabilitation programs include oral phosphodiesterase type-5 (PDE-5) inhibitors, intracavernous injections, intraurethral alprostadil, and vacuum erection devices. 12
Current literature suggests a wide range in the rate of recovery of potency following radical prostatectomy, 11% to 86% and the time required between 6–24 months. 9,12 –14 In our single institution, single surgeon series, we investigated the independent predictors of potency recovery and quality potency (potent without PDE-5 inhibitors) in RARP patients.
Materials and Methods
Patient selection
Between 2008 and 2010, a total of 503 consecutive patients with a minimum follow-up of 12 months after RARP by a single surgeon were identified. In these patients, all pre- and postoperative data were collected prospectively and analyzed retrospectively after obtaining the approval of the Institutional Review Board. During each follow-up visit, patients completed the self-administered questionnaires, including the Sexual Health Inventory for Men (SHIM) and the American Urologic Association symptom score (AUASS). The surveys were administered by the medical technicians and collected by the nursing staffs during each visit pre- and postoperatively. The office technicians were blinded to the preoperative erectile status of the patient and the type of surgery.
Surgical procedure
The procedure for the preservation of neurovascular bundle (NVB) was performed using both interfascial and intrafascial nerve sparing techniques. Intrafascial nerve sparing was performed as previously described. 15 Bilateral nerve sparing was carried out in patients with the Gleason sum ≤7, PSA ≤10, clinical stage T2a or less. Bilateral NVBs were spared intrafascially if the number of positive biopsy cores ≤3 (with a minimum of 12 cores) and no core with 50% or more malignant tissue. The NCCN guideline was used to determine the necessity of pelvic lymph node dissection.
Definitions
Potency before and after RARP was defined as the ability to achieve penetration and maintain erection in ≥50% of attempts using question #2 and #3 on SHIM. 16,17 In men with a SHIM score >21, the erectile function was considered normal. Quality potency, called functional erection, 18 was defined as potency without the use of PDE-5 inhibitors.
Penile rehabilitation
Our institutional penile rehabilitation program includes sildenafil 50 mg every other night for the first 3 months following the removal of the urethral catheter. After the 3-month follow-up visit, PDE-5 inhibitors were used on demand in the following order: tadalafil 20 mg (month 3–6), sildenafil 100 mg (month 6–9), and vardenafil 20 mg (month 9–12). Immediately following the removal of Foley catheter, sildenafil was started based on the literature that sildenafil may be neuroprotective. 19,20 Because each of the three commonly used PDE-5 inhibitors has varying pharmacokinetics based on the CYP3A5 genotype that may result in differing clinical responses, 21 PDE-5 inhibitors were switched at each follow-up visit if there was no satisfactory response. PDE-5 inhibitors were stopped when the patient was satisfied with the quality of the erection.
Statistical analysis
Factors that potentially impacted the recovery of potency were analyzed with univariate and multivariate Cox regression analysis. Statistical analysis was performed using the SPSS 12.0 software (SPSS, Inc., Chicago, IL), and statistical significance was defined as p-value <0.05.
Results
The clinicopathological characteristics of 503 patients are shown in Table 1. In this cohort, the mean age was 59.3 years; the mean AUASS was 9.1 and mild in 51.6%, moderate in 38.7%, and severe in 9.7%. Preoperatively, 202 men had a normal erectile function (SHIM >21) (41.8%), while 324 (67.1%) men were potent. Postoperatively, 470 (93.4%) patients were discharged home within 1 day.
PSA=prostate-specific antigen; AUASS=American Urologic Association symptom score; SHIM=sexual health inventory for men; NVB=neurovascular bundle; GS=Gleason score.
Postoperative potency
Of the 503 patients, 483 (96%) men underwent our institutional penile rehabilitation program. One year after RARP, 61.4% of the men were potent. The overall potency rate was 11.5%, 30.1%, 44.7%, and 61.4% at 3, 6, 9, and 12, respectively (Fig. 1). When stratified by the preoperative SHIM score, men with normal erection (SHIM 22–25) had an overall and quality potency rate of 79.7% and 41.2%, respectively (Fig. 2). As expected, both the overall and quality potency rates decreased in men with a lower SHIM score preoperatively. Interestingly, in men who were impotent preoperatively (SHIM 1–7), a small fraction recovered erection that is sufficient for penetration (overall and quality potency rate of 14.9% and 6.4%, respectively) (Fig. 3).

Recovery of overall and quality potency in all patients.
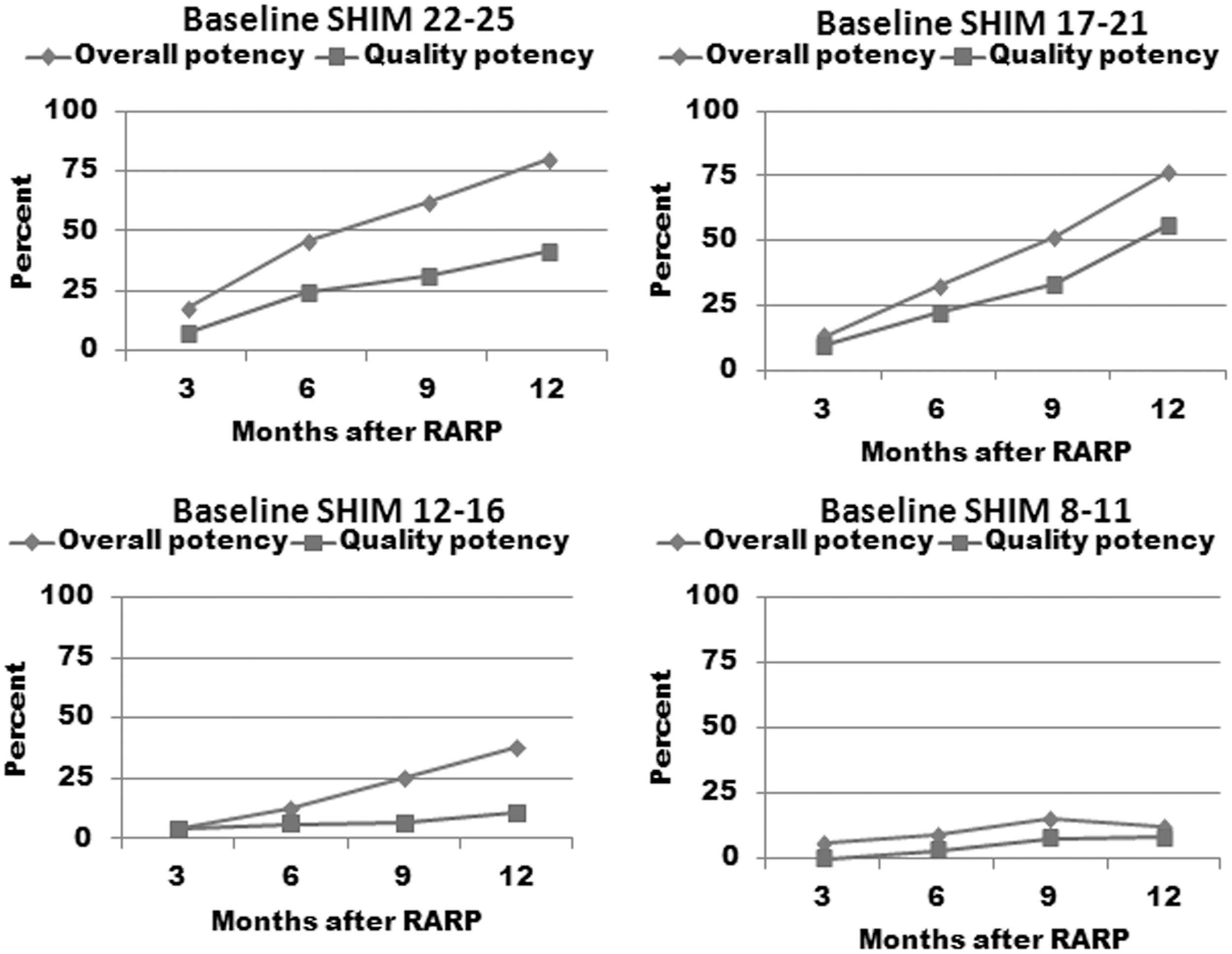
Overall and quality potency stratified by the preoperative sexual health inventory for men (SHIM) score.
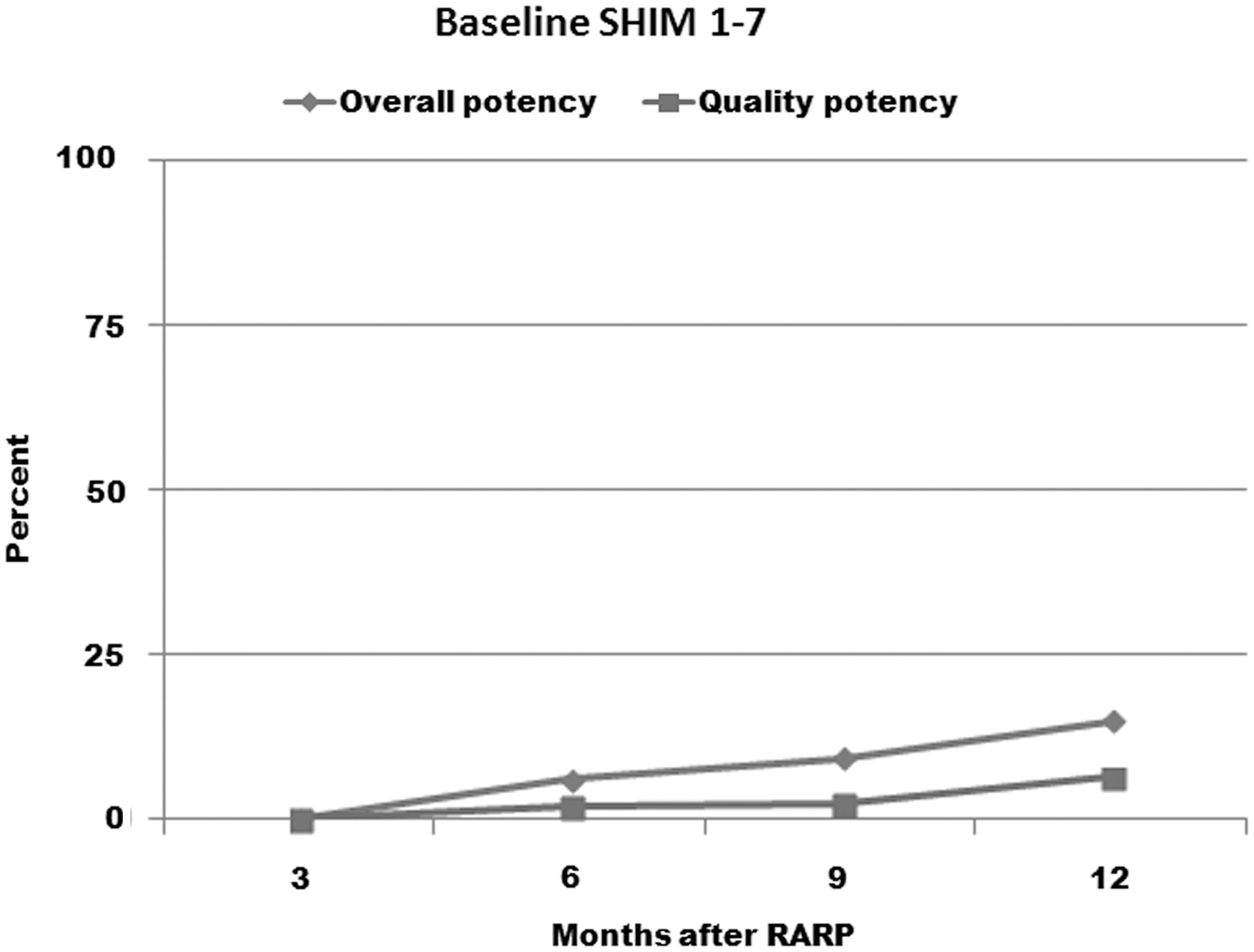
Potency rate in patients who were impotent preoperatively.
On univariate analysis, predictors of potency recovery were age, surgical technique (interfascial vs intrafascial), preoperative potency status, preservation of NVBs, AUASS, pathologic stage, and surgical Gleason score (GS) (Table 2). On multivariate Cox analysis, the age at surgery (OR 0.875, p=0.041), preservation of NVBs (OR 1.655, p=0.036), and preoperative potency (OR 4.459, p<0.001) were independent predictors (Table 2). A flow chart based on these independent predictors is shown in Figure 4.
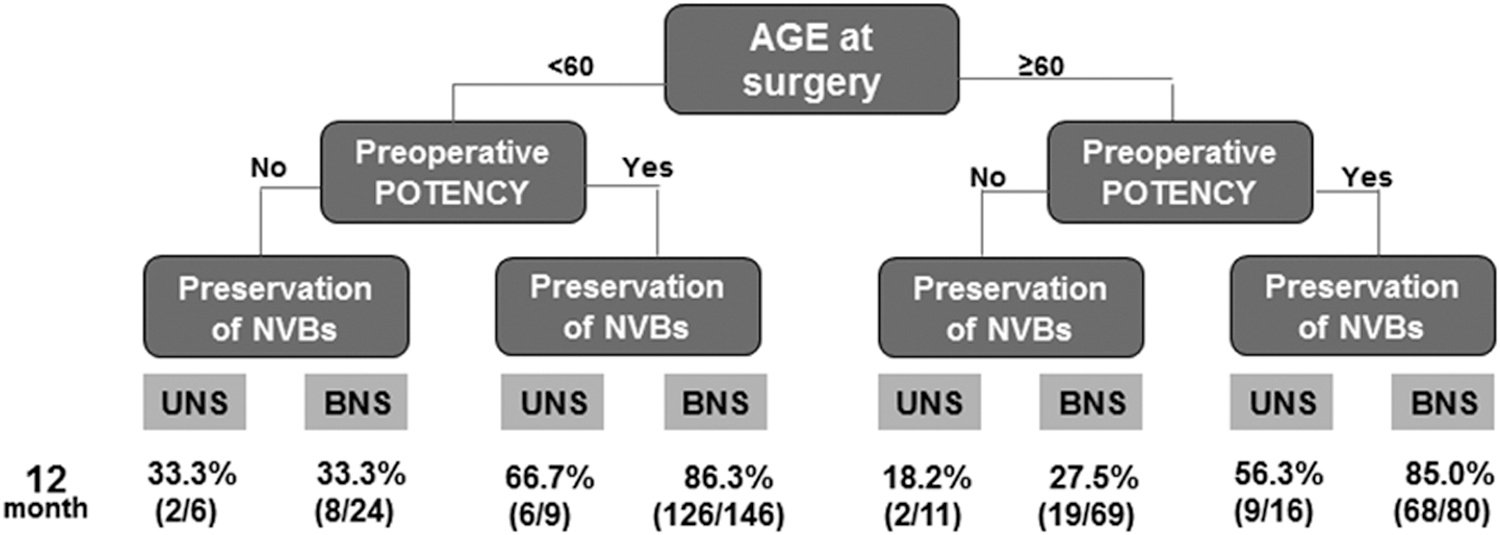
Flow chart to expect postoperative potency as considering independent tripredictors; age, preoperative potency, neurovascular bundle saving.
CI=confidence interval; AUSS=American Urologic Association symptom score; GS=Gleason score.
The change of erectile dysfunction severity on SHIM
To analyze the change of potency following RARP, we next analyzed the change in the SHIM score. The results demonstrated that in men with SHIM>21 preoperatively, only 21.4% fully recovered the quality of erection (Table 3). In patients who were potent preoperatively, the quality of erection decreased by 1–2 ranks (based on the SHIM classification) postoperatively.
SHIM=sexual health inventory for men.
Discussion
In men with prostate cancer considering RP, erectile dysfunction is a serious concern with a profound implication on survivorship. Yet, published studies have used a very broad stroke to define post-RP potency: the ability to achieve erection that is sufficient for intercourse in over half the attempts with and without PDE-5 inhibitors. Since erectile dysfunction is complex and has a wide range, such a dichotomous view on postoperative potency potentially gives men considering RP an unrealistic expectation. In this regard, the present study analyzed in detail the nature of potency in our cohort of 483 patients who underwent RARP. The results demonstrated that the overall potency rates preoperatively and 12 months after surgery were 67.1% and 64.7%, respectively. In men with a normal erectile function preoperatively, 79.7% were potent 12 months after RARP. However, only 41.2% of the men with SHIM>21 were potent without PDE-5 inhibitors. When SHIM scores were compared pre- and postoperatively, the fraction of men with normal erection preoperatively who returned to baseline after RARP was 21.4%. Taken together, these results shed additional light on the nature of sexual function after surgery. 22
Herein, the overall potency rate preoperatively was 67.1%; postoperatively, 64.7% of the men were potent. This virtual lack of difference in the overall potency rate post-RARP was initially surprising as ∼20% of men with normal erection preoperatively were impotent after surgery. However, a more detailed analysis revealed that the decrease in the post-RARP potency rate for men with normal SHIM preoperatively was countered by a significant improvement in postsurgery erectile function in men who were impotent before surgery. Specifically, in men with preoperative SHIM <8, the overall and quality potency rates were 14.9% and 6.4%, respectively. The precise explanation for the improvement in erectile function after RARP in some men who were impotent preoperatively is not clear. One plausible explanation is that the etiology of the preoperative erectile dysfunction in some men was nonphysiologic, that is, psychogenic. With our institution's treatment philosophy of counseling and penile rehabilitation program using PDE-5 inhibitors immediately after surgery, a minority of patients with nonphysiologic erectile dysfunction may be able to recover potency eventually. Additional studies are underway to verify this concept.
Since the first introduction of NVB sparing RP by Dr. Patrick Walsh in 1982, postradical prostatectomy potency has increased significantly. 23,24 For example, in the landmark article that first reported on NVB sparing RP, the potency rate was 39%. 23 However, more recent reports, including RARP and open RP report postsurgical potency rates above 80% to 90%. 25,26 Such significant improvement in potency after surgery has been mostly attributed to surgical refinement and improvement. However, the current study suggests an alternative explanation: the introduction of PDE-5 inhibitors. Currently, the most widely used definition for potency following RP includes the use of PDE-5 inhibitors. When this commonly used definition of potency was applied to the present cohort, the overall potency rate in men with normal erectile function preoperatively (SHIM>21) was 79.7%. In contrast, only 41.2% of these men were potent without the use of PDE-5 inhibitors. In short, without PDE-5 inhibitors, less than half of the men who had preoperative SHIM>21 were potent. Accordingly, the significant improvement is potency rates reported by many surgeons, especially since the wide adoption of RARP, may be due to advances in medications and not surgical techniques. Similar analysis of data from other institutions is necessary to confirm this hypothesis.
In a recent study addressing a return to baseline sexual function measured with the Extended Prostate Cancer Index Composite (EPIC), 85% of preoperatively potent men who had RP with bilateral NVB sparing were potent at 24 months, while only 27% returned to baseline EF. 27 Similarly, in our analysis, 21.4% of the men with SHIM>21 preoperatively returned to their baseline erectile function following RARP; in men with SHIM 17–21 before surgery, 40.8% returned to baseline postoperatively. Since the overall potency rate of men with preoperative SHIM>21 and 17–21 were 79.7% and 76.5% after RARP, an overwhelming majority of men with normal erection before surgery suffer significant deficit to the erectile function after surgery.
Age, erectile function, comorbidity (diabetes mellitus, hyperlipidemia, etc.) at surgery, surgical technique (preservation of NVBs), and postoperative PDE-5 inhibitor use have been reported to predict the recovery of potency after RP irrespective of surgical types. 7,18,28,29 Among these reported factors, the most consistent independent predictors of postsurgery potency were preoperative age and erectile function. In the current study, univariate analysis demonstrated that factors, which influenced potency recovery following RARP, were age at surgery, preoperative potency and AUASS, preservation of NVBs, the method of nerve sparing (interfascial vs. intrafascial), pathologic stage, and GS. However, multivariate analysis revealed that only age (<60 years) and SHIM score at surgery and preservation of bilateral NVBs were positive independent predictors of potency recovery after RARP.
It should be noted that the preservation of NVBs was more important for the recovery of potency than the surgical technique for saving NVBs. Previously, we and others have reported that the intrafascial nerve sparing technique resulted in a higher potency recovery rate than interfascial. 15,30 However, with a larger sample size in the present cohort, there was no significant difference in the recovery of potency postoperatively in men who underwent interfasical versus intrafascial nerve sparing (60.0% vs 68.2% at 12 month, p=0.132).
A major limitation of the present study is the retrospective analysis of the data. Additional concern includes nonrandomization in the nerve sparing method. However, there was no difference in baseline characteristics between the interfascial and intrafascial method when we additionally analyzed the age, body mass index, preoperative PSA, AUASS, SHIM, stage and GS before and after RARP, and preservation of NVBs. Lastly, the impact of the penile rehabilitation program used in our patients is unclear as we did not conduct a randomized clinical trial.
In conclusion, in men with normal erection before surgery, the overall recovery rate of potency 1 year after RARP was 79.7%. However, more than half of these men required PDE-5 inhibitors and only a quarter returned to the baseline erectile function. These results suggest that most men experience significant deficit on erection after RARP.
Footnotes
Acknowledgments
This work has been supported, in part, by generous grants from the Tanzman Foundation, Jon Runyan's Score for the Cure, and by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2013-003819) and supported by a grant from the Next-Generation BioGreen 21 Program (No. PJ009621), Rural Development Administration, Republic of Korea.
Disclosure Statement
For all authors, no competing financial interests exist.