
Abstract
Purpose:
To present our initial experience with laparoendoscopic single-site (LESS) urologic surgery using conventional laparoscopic instruments and to assess its feasibility and safety.
Patients and Methods:
In 20 patients, we performed LESS urologic surgery, which included simple nephrectomy in 9, nephroureterectomy in 1 for a refluxing nonfunctioning kidney, radical nephroureterectomy in 1, heminephroureterectomy in 1 for a nonfunctioning upper moiety in a complete duplex kidney, marsupialization of a renal cyst in 1, ureterolithotomy in 1, varicocelectomy in 2, pyeloplasty in 2, vesicovaginal fistula (VVF) repair in 1, and orchiopexy in 1. LESS was performed using a small periumbilical incision, inserting regular trocars, and using a conventional 30-degree laparoscope and laparoscopic instruments. Data were collected prospectively with respect to feasibility, intraoperative or postoperative complications, postoperative pain, analgesic requirement, and recovery.
Results:
Since March, 2012, a total of 20 patients have undergone LESS for various urologic conditions. All cases were completed successfully, without conversion to a standard laparoscopic or open approach. The total operative time for the nephrectomy, nephroureterectomy, pyeloplasty, VVF repair, ureterolithomy, varicocelectomy, or orchiopexy was 134±20.06, 186±40, 135±21, 180, 150, 55, and 60, minutes, respectively. The mean blood loss was 100 mL. No intraoperative complication occurred. The mean pain score on the visual analog scale was 8.35±0.9 (8–10) on day 1, 4.8±1.6 (2–8) on day 2, and 2±1.2 (2–4) on day 3. Similarly, the mean analgesic requirement was 220±41 mg, 85±74 mg, and 30±47 mg of intravenous tramadol, respectively. One patient had surgical emphysema of the abdomen and another had ileus for 4 days. The mean hospital stay was 2.9±1.7 (2–7) days.
Conclusion:
In selected patients, LESS for urological indications using conventional laparoscopic instruments is safe and feasible with no added cost. Additional experience and continued investigation are warranted.
Introduction
Laparoscopic surgery is a well-established surgical technique for a variety of urologic procedures. The first laparoscopic nephrectomy was performed by Ralph Clayman 1 in 1991, and the benefits of minimally invasive urologic surgery have been repeatedly confirmed and established since then. In laparoscopic surgery, each port inserted has a risk of complications such as bleeding, infection, pain, hernia, visceral injury, and compromised cosmetic outcome. 2
In recent years, multiple attempts to decrease parietal trauma and visible scars have been proposed. These efforts include the reduction of the diameter of the port size, the reduction in the number of laparoscopic accesses, 3,4 and the introduction of natural orifice translumenal endoscopic surgery, 5 single incision laparoscopic surgery, or laparoendoscopic single-site (LESS) surgery. 6 The term LESS was coined at the LESSCAR (Laparo-Endoscopic Single Site Surgery Consortium for Assessment and Research) symposium in 2008 to avoid multiple nomenclatures. 6 The main credit for pioneering single-site laparoscopic surgery in urology goes to Rane and coworkers. 7,8 Since then, LESS has been reported in a variety of urological surgeries such as nephrectomy, 9 –12 pyeloplasty, 10 –12 radical nephrectomy, 10,12,13 simple prostatectomy, 14 and donor nephrectomy. 12,15 –17
These procedures have been performed at few centers worldwide. Commonly, the procedure requires specialized custom-made ports such as Unix-XTM (PNAVEL System), R-Port (Olympus), GelPort (Applied Medical), SILS™ Port (Coviden), reticulating instruments with angulations of forward one-third with various tips, and a specialized laparoscope 17,18 to avoid instrument clashing and achieve triangulation of conventional laparoscopy. This not only adds additional surgical cost 17 and burden on the patients in a developing country like India, but also necessitates considerable training to acquaint surgeons with the instruments. We present our initial experience with LESS urologic surgery using conventional laparoscopic instruments.
Patients and Methods
From March to November 2012, a total of 20 patients underwent LESS surgery for various urologic conditions, such as simple nephrectomy in 9, nephroureterectomy in 1 for a refluxing nonfunctioning kidney, heminephroureterectomy in 1 for a nonfunctioning upper moiety in a complete duplex kidney, radical nephroureterectomy for transitional-cell carcinoma of the renal pelvis in 1, pyeloplasty in 2, vesicovaginal fistula (VVF) repair in 1, marsupialization of a renal cyst in 1, ureterolithotomy in 1, varicocelectomy in 2, and orchiopexy in 1. The mean patient age was 35.8±13 (15–72) years; male to female ratio was 12:8. A single surgeon with experience in laparoscopy was involved in all cases.
General surgical procedure
For all operations, the patient received general anesthesia and was placed in a conventional lateral position as for a multiport laparoscopic donor nephrectomy. A 2 to 3 cm semicircular incision was made in the groove between the umbilicus and abdominal wall and deepened until the rectus fascia (Fig. 1A). A flap was raised in the subcutaneous level adequate enough to accommodate the ports (Fig. 1B). Pneumoperitoneum was established using a Veress needle inserted through the rectus fascia (Fig. 1C). Three separate vertically aligned conventional ports (one 10-mm and two 5-mm ports) were inserted through this single incision (Fig. 1D). For the right side, an additional 5-mm port was inserted, and laparoscopic alligator forceps was used for liver retraction. The final ports alignment for a different procedure was as shown in Figure 2. Intraperitoneal CO2 was maintained at 13 to 15 mmHg. For surgery, a conventional 10-mm 30-degree rigid laparoscope (Storz) and working instruments were used. A harmonic scalpel (Ethicon) was used for dissection.

Port insertion method.
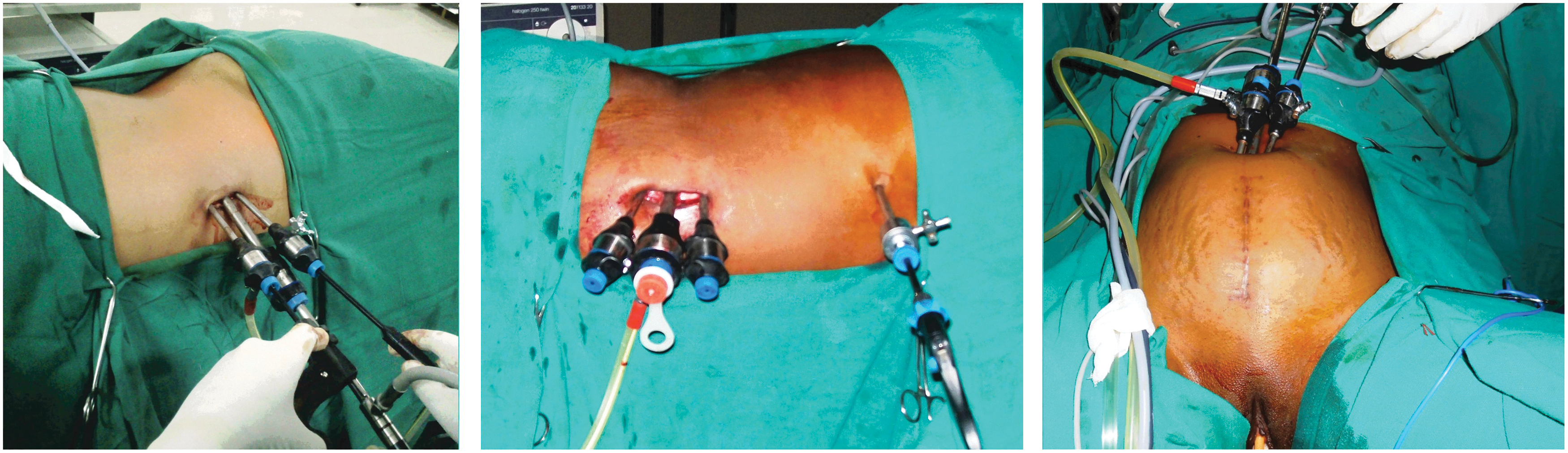
Final arrangement of working ports. Central camera port (10 mm); working ports (5 mm)×2 for left side, right side, and pelvic surgery, respectively.
A simple nephrectomy (Fig. 3) proceeded in the standard fashion by first reflecting the colon medially, identifying and dissecting the ureter and gonadal vein toward the renal hilum. The renal artery and vein were dissected. For vascular control, a 10 mm laparoscope was exchanged with a 5 mm and inserted with the lower 5-mm port, a hemoclip applicator was introduced through the 10-mm port, and vascular control obtained. The rest of the dissection was performed using a harmonic scalpel, and the specimen was retrieved via the umbilical incision, which was extended a small amount for the removal.
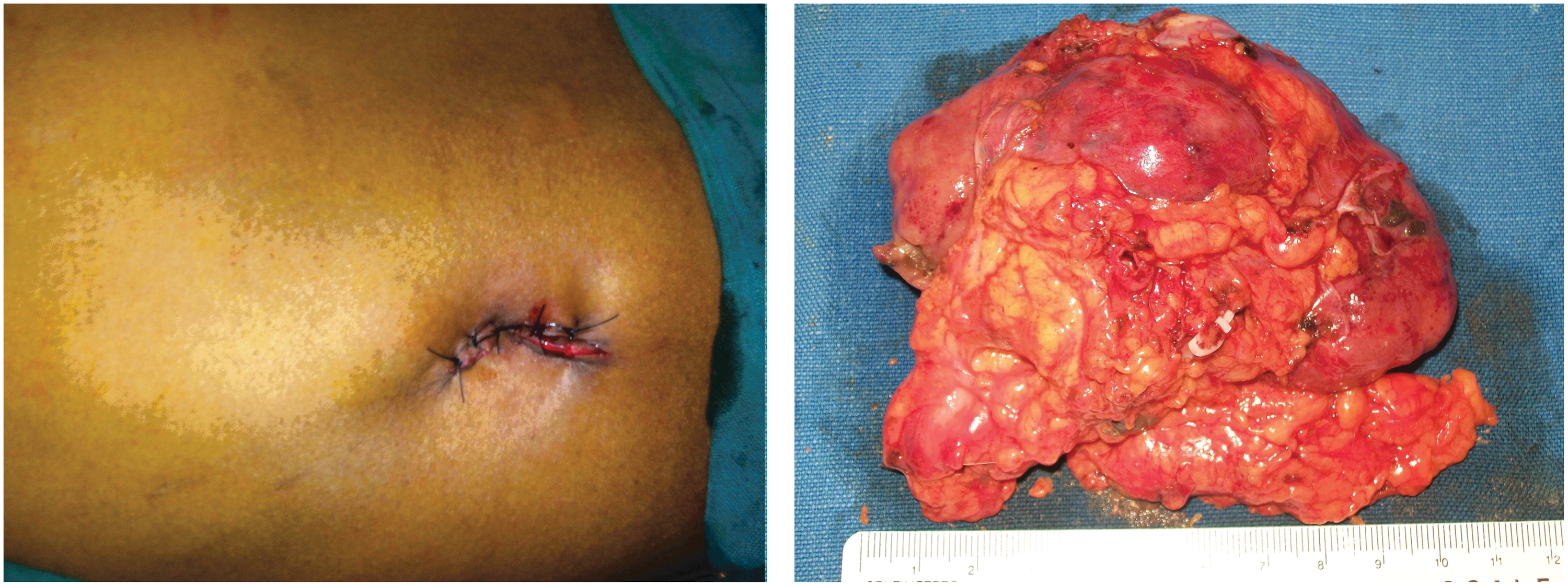
Laparoendoscopic single-site simple nephrectomy incision and specimen removed through the umbilical incision used for ports.
A heminephroureterectomy (Fig. 4) was performed in a 23-year-old patient who presented with a symptomatic nonfunctioning refluxing moiety in a complete duplex hydronephrotic kidney. Both ureters were identified; the upper moiety dilated ureter was dissected from the lower moiety ureter keeping vascularity intact until bladder insertion, clipped, and cut. The upper moiety was dissected off the lower moiety and the specimen removed in total through the umbilical incision. Similarly, other procedures were performed in standard laparoscopic fashion. An additional 5-mm port was inserted for liver retraction on the right side nephrectomy; no additional skin incision was used. The umbilical incision was closed.

Laparoendoscopic single-site nephroureterectomy for duplex nonfunctioning moiety on the left side.
A LESS dismembered Anderson-Hynes pyeloplasty (Fig. 5) was performed in two patients with pelviureteral junction obstruction, using a method similar to that of conventional laparoscopy. A 6/26F Double-J stent insertion was performed with an initial puncture needle used for percutaneous nephrostomy and dilating up to a 10F fascial dilator. Intracorporeal suturing was performed without using an additional port. A drain, placed through the umbilical wound, was removed when drainage was either nil or less than 50 mL.

Anderson-Hynes laparoencoscopic single-site pyeloplasty on the right side for pelviureteral (PUJ) obstruction.
LESS VVF repair (Fig. 6) was done by the O'Connor's transvesical approach in one patient with supratrigonal VVF of 1.5 cm after a transabdominal hysterectomy. After adhering intestines and omentum were taken off from the vagina and urinary bladder, the bladder was bivalved up to the fistula. Both vagina and bladder were separated well and closed separately after interposing the omentum in between. Intracorporeal suturing was performed without using an additional port. A drain, placed through the umbilical wound, was removed when drainage was nil. No suprapubic catheter was kept; only a per-urethra catheter was kept for 14 days.

Laparoendoscopic single-site vesicovaginal fistula repair showing dissecting off fistula tract, intracorporeal suturing of the fistula, and skin incision.
The success of all 20 cases of LESS was evaluated by determining the number of cases of conversion to open abdominal surgery, the operative time, the surgical complications, the dose of analgesics needed after surgery, the duration of hospital stay, the duration of the postsurgical recovery period, and the time needed to return to routine life. Safety was evaluated by assessing the complications that occurred before and after surgery. The pain experienced by the patients was analyzed by using the preoperative and postoperative 10-point visual analog scale (VAS) score, in which no pain and the worst pain are scored at 0 and 10 points, respectively.
Results
A total of 20 patients underwent LESS surgery (Table 1) for various urologic conditions. All cases were completed successfully, without conversion to a standard laparoscopic or open approach.
Details of Laparoendoscopic Single-Site Surgery
LESS=laparoendoscopic single-site; SD=standard deviation; OT=operative time; VVF=vesicovaginal fistula; B/L=bilateral.
For the 20 cases of LESS surgery, the mean operative times for simple nephrectomy (9), nephroureterectomy (3), pyeloplasty (2), VVF repair (1), marsupialization of a renal cyst (1), ureterolithotomy (1), varicocelectomy (2), orchiopexy (1) were 134±20.06, 186±40, 135±21.1, 180, 45, 150, 70, and 60 minutes, respectively (Table 1). The hospital stay was 3.28±0.88 days for nephrectomy, 4±1 days for nephroureterectomy, 2 days for varicocelectomy, and 3 days for pyeloplasty, VVF repair, ureterolithotomy, marsupialization of a renal cyst, and orchiopexy, respectively (Table 1). The maximum estimated blood loss for all patients during surgery was approximately 150 mL. None of the patients needed a blood transfusion. There were three cases of postsurgical complications (15%)—namely, prolong ileus in one, surgical emphysema of the abdominal wall in two, and wound infection in one. All responded to conservative treatment. There were no major complications.
For all patients, the postsurgy VAS scores and analgesic requirement for intravenous tramadol on days 1, 2, and 3 were as shown in Table 2. All of the 20 patients in whom LESS surgery was performed successfully began oral intake 8 to 10 hours after surgery, and the return to routine life occurred on average 4.28±1.88 days after surgery. The survey on the level of satisfaction felt by the patients revealed that 15 (75%) felt very satisfied and the remaining 5 (25%) felt somewhat satisfied. One nephroureterectomy patient had associated thimble bladder and stricture at the lower end of the opposite ureter for which he underwent augmentation cystoplasty and ureteral reimplantation.
Analysis of Pain and Analgesic Requirement
VAS=visual analog scale; SD=standard deviation; IV=intravenous; LESS=laparoendoscopic single-site; VVF=vesicovaginal fistula; B/L=bilateral.
Discussion
Although the LESS technique was first attempted and reported on 10 years ago, limitation of ergonomic surgical skills and low reproducibility have limited its widespread use. Rane and associates 7 first reported LESS nephrectomy. After this, many centers reported this modality of surgical management for various urologic problems. Initially, several terms were used to describe laparoscopic surgery through a single incision site; however, in 2008, LESSCAR proposed that the term LESS be used. 6
The biggest challenges with LESS using conventional instruments are crowding and clashing of instruments external to the portal of entry and limitations in the ability to triangulate to the target organ internally as is done with conventional laparoscopy, and LESS using conventional instruments provides an in-line instrument deployment and visualization of the operating field. 12,18,19 A variety of modifications in the instruments and port specifications have been suggested to overcome these limitations in LESS.
Specialized low profile access ports that allow the passage of flexible, articulated, and curved instruments such as Unix-XTM, R-Port, GelPort, SILS Port are used for access. Triangulation from a single port can be achieved with articulated or steerable instruments, such as the ones from Cambridge Endo (Framingham, MA), the Real Hand line from Novare Surgical Systems (Cupertino, CA), the Roticulator from Covidien (Norwalk, CT), and the SITRACC system from EDLO (Porto Alegre, RS, Brazil). Standard rigid laparoscopes are approximately 30 cm in length and need a connection to a light cord and camera component, which exacerbates an already crowded space leading to instrument clashes. This can be circumvented either by use of a specialized longer bariatric length laparoscope (45 cm; Stryker, Kalamazoo, MI) or an extended length (50 cm) bronchoscope (Storz, Tuttlingen, Germany) to distance the camera holder and endoscope components from the surgeon and free up valuable working space, or by use of the EndoEYE™ 5-mm deflectable tip endoscope (Olympus, Center Valley, PA). The EndoEYE flexible laparoscope offers 100 degrees of angulation, and its digital design obviates the need for additional camera and light cord attachments. This increases maneuverability within the operative field while minimizing use of the valuable space external to the patient. 18,19
There are limitations, however. First, it involves additional cost, 17 escalating the end surgical cost of the procedure, depriving benefits of LESS to those least able to afford it, which constitute the majority of our patients. Second use of articulating, extra-long and, curved working instruments necessitates familiarization of working with them. In an experimental study, Stolzenburg and colleagues 20 found prebent and flexible instruments to be more time-consuming for the performance of laparoscopic tasks compared with standard laparoscopic instruments.
Our technique of port insertion is similar to one described by Raman and associates 8 and Dubey and coworkers 17 in which 5-mm or 10-mm standard working ports are directly inserted through the rectus fascia, under the periumbilical skin flap. In comparison with most of the published series, we have used standard rigid laparoscopy working instruments and laparoscope along with a harmonic scalpel, thereby decreasing the amount of investment needed for setting up infrastructure for starting a LESS program. To increase ergonomic maneuverability and to decrease clashing of instruments, ports are inserted at different planes, and the camera person does the navigation by sitting and operating at a distance to avoid clashing with the surgeon. Inline visualization of LESS may not be cumbersome for the surgeon proficient with standard laparoscopy after a few cases.
In 2009, Desai and colleagues 10 described their first 100 cases of LESS surgery using the R-Port for various urologic conditions; it provided outcomes equivalent to those of standard laparoscopy and offered an additional benefit of better cosmesis and quicker convalescence. With regard to the 20 LESS surgery cases described here, surgical indications are comparable to those of any other series, and all the surgeries were successfully performed without any major complications or conversion to open surgery or conventional laparoscopy. In comparison with other series in which they routinely or when necessary used an additional port, either for retraction of tissue or for intracorporeal suturing, we were able to perform the procedure without an extra port.
LESS surgery using conventional instruments is associated with several advantages. First, only one incision is involved as in any other LESS surgery, it elevates patient satisfaction in terms of aesthetic outcome, and reduces pain after surgery. Indeed, in the present study, the postoperative VAS scores and analgesic requirement revealed a substantial reduction of pain after surgery, and the majority of our patients stated that they were very satisfied with the operation. Second, the operative time needed for LESS in our series is reasonable in comparison with other series in which they used a custom-made port or specialized instruments. Third, there was no additional expenditure for the institute to start a LESS program, resulting in no additional operative cost to the patients. Fourth, a surgeon who is proficient in standard laparoscopy can very well and quickly adapt to LESS surgery. Fifth, although the number of patients we operated on is smll, from our series we can very well say that this modality of LESS surgery with conventional instruments is feasible and can be performed for the majority of urologic conditions safely with an outcome equal to other LESS surgeries. Sixth, there is no theoretical increase in incisional hernia because ports are placed separately in different planes.
There are certain drawbacks using conventional instruments in LESS surgery. First, there will be clashing of instruments, but this can be decreased by inserting the ports at different planes, with the camera person performing the navigation by sitting and operating at a distance to avoid clashing with the surgeon. Second, there may be a gaseous leak from the port sites that hinders surgical progress; this sometime leads to surgical emphysema but usually subsides with conservative management. Third, all ports are inserted blindly, so to avoid any bowel injury, it is a prerequisite to insert all ports after adequate pneumoperitonium and through scanning of the abdomen after inserting the camera port.
In our series, we have not used any longer instruments, 16,17 often mentioned in studies. This may be because most of our patients were moderately built. Similarly, pain scores and analgesic requirement on day 1 was more compare with published reports. 10,12,13 Pain is not related to the indication for surgery but related to the duration of surgery, whether it is because of insertion of multiple facial ports under one incision or from friction at the site of the facial and port interface because of continuous manipulation needs. This needs further investigation.
Conclusion
In selected patients, LESS urologic surgery using conventional laparoscopic instruments is safe and feasible with no added cost. Additional experience and continued investigation are warranted.
Footnotes
Disclosure Statement
No competing financial interests exist.