
Abstract
Purpose:
To determine the impact of staghorn calculi branch number on outcomes of percutaneous nephrolithotomy (PNL).
Materials and Methods:
Retrospectively, we evaluated 371 patients (386 renal units) who underwent PNL for staghorn calculi. All calculi were showed with CT three-dimensional reconstruction (3DR) imaging preoperatively. From 3DR images, the number of stone branching into minor renal calices was recorded. According to the number, patients were divided into four groups. Group 1: the branch number 2–4; Group 2: the branch number 5–7; Group 3: the branch number 8–10; Group 4: the branch number >10. The number of percutaneous tract, operative time, staged PNL, intraoperative blood loss, postoperative hospital stay, complications, main stone composition, and stone clearance rate were compared.
Results:
A significantly higher ratio of multitract (p<0.001) and staged PNL (p<0.001), a longer operative time (p<0.001) and postoperative hospital stay (p=0.043), and a lower rate of stone clearance (p<0.05) were found in PNL for calculi with a stone branch number ≥5. There was no statistical difference in intraoperative blood loss (p=0.101) and main stone composition (p=0.546). There was no statistically meaningful difference among the four groups based on the Clavien complication system (p=0.46).
Conclusion:
With the stone branch number more than five, the possibility of multitract and staged PNL, lower rate of stone clearance, and a longer postoperative hospital stay increases for staghorn calculi.
Introduction
T
Traditionally, staghorn calculi are classified as partial and complete staghorn according to two-dimensional images, such as a plain film of the kidney-ureter-bladder (KUB), an intravenous urogram (IVU), ultrasonography, and computed tomography (CT). The spatial structure of the calculus is ignored in this classification. In addition, there are some disadvantages regarding image quality. 2 CT technology has been improved especially in the field of three-dimensional reconstruction (3DR) imaging for staghorn calculi. 3 3DR images of the stone have the advantage in showing the branches accurately. They can display the orientation of branches, better demonstrate the presence of parallel branches, and show the appropriate route of the tract to insure complete calculus removal. 4
Although PNL has a high success rate, most urologists continue to have interest in the predictors of PNL outcomes. The studies about effects on the outcomes of PNL for staghorn calculi mainly focused on stone or patient-related factors (such as the stone surface area). 5 –7 However, in our practice, we found the following phenomenon based on 3DR images: the PNL procedures and outcomes of some staghorn stones with more branches, but a smaller stone surface area are dissatisfactory than those of some stones with fewer branches, but a bigger stone surface area. Thus, we consider that the stone branch number maybe a predictive factor of PNL for staghorn calculi.
Materials and Methods
Clinical data
From July 2008 to July 2012, 371 patients (386 renal units) with staghorn stones who were referred to our hospital for PNL were considered for this study. We reviewed the computerized database of the patients. Our exclusion criteria were patients with congenital renal anomalies (such as horseshoe or ectopic kidneys) and stones that branched to only one major calyx. All patients underwent CT. Data were viewed, assessed, and reported using 3DR images. From 3DR images, the number of stone branching into minor renal calices was recorded. The branch number ranged from 2 to 14. According to the branch number, patients were divided into four groups. Group 1: the branch number 2–4; Group 2: the branch number 5–7; Group 3: the branch number 8–10; Group 4: the branch number >10. All patients underwent urine culture preoperatively. The patients with negative results received intravenous second-generation cephalosporins at the time of giving anesthesia. Other patients with urinary tract infections received culture-specific antibiotics for 5 days before PNL.
The procedure of PNL
All PNL procedures were performed under general anesthesia or continual epidural anesthesia. To facilitate puncture, an external 7F ureteric catheter with retrograde injection of saline was inserted in the lithotomy position. Then, the patient was placed in a prone position. With the guidance of a 3.5-MHz ultrasound probe (MEDISON Ultrasound System), a 17.5-gauge coaxial needle (uroVision GmbH) was inserted into the targeted calyx. The principle of selection for the targeted calyx was the shortest skin-to-stone distance and the ability to make the branch-target calyx angles less than 90 degrees as many as possible. The tract dilation was performed with a two-step method in all patients. First, a serial fascial dilator (uroVision GmbH) was used for dilation from 10 to 16F, and the same-sized peel-away sheath was placed as a micropercutaneous tract. In addition, an 8/9.8F rigid ureteroscope was introduced to ensure the tract. Second, a telescopic metal dilator (Richard Wolf ) was inserted to dilate the working access from 15 to 21F, followed by the introduction of a16-cm-long, 24F metal working sheath (Richard Wolf ) as a standard percutaneous tract. Then, under the monitoring of a 20.8F nephroscope (Richard Wolf ) placed into the kidney through the tract, stones were fragmented and cleared using a combination of ultrasonic and pneumatic lithotripter (LithoClast Master; EMS Electro Medical Systems). For some patients, 16F flexible nephroscopy and Holmium:YAG laser were used to clear stones away from the initial puncture. If the stone could not be reached through one tract, additional tracts were created in the same session. Finally, a 6F Double-J stent was introduced antegrade into the ureter and a 14F nephrostomy tube was inserted in all patients. Infrared spectroscopy was used to determine the main stone composition. The stones were considered of a certain variety, if they consisted of ≥51% of one type.
Potential residuals tones were detected by KUB and B-scan ultrasonography 3 days postoperatively. A follow-up was elected for residual fragments smaller than 4 mm, SWL for residual fragments of 4 to 10 mm, and staged PNL for residual stones larger than 10 mm or if they were accessible through the present tracts. All patients were estimated again for residual stones 3 months later. Stone free was defined as no residual stones. Complications were classified according to the modified Clavien classification system.
Evaluation
The operative time was counted from the beginning of puncture to the removal of the last operating sheath. The operative time of staged PNL was the sum of each stage. The intraoperative blood loss was counted with the formula: blood loss (mL)=[hemoglobin concentration of irrigating fluid (g/L)×total volume of irrigating fluid (mL)]/preoperative hemoglobin concentration (g/L). 8 The basic data of patients and stones, the information about the percutaneous tract, operative time, intraoperative blood loss, rate of staged PNL, postoperative hospital stay, the complications, the main stone composition, and the stone clearance rate were record as data, and compared among the four groups.
Statistical analysis
The results are presented as mean±standard deviation. Statistical analysis was performed with SPSS version 15.0 using the Chi-square tests, unpaired t test, Mann–Whitney U tests, and Fisher's exact tests as necessary. p<0.05 considered as a significant level.
Results
Demographic data of patients and stone-related factors are summarized in Table 1. Among 386 renal units (371 patients), there were 138 (35.8%), 106 (27.5%), 77 (19.9%), and 65 (16.8%) in Group 1, Group 2, Group 3, and Group 4, respectively. The body mass index (BMI) was 26.7±4.8 kg/m2 and mean patient age was 42.3±14.7 years. There was no clinically significant difference for the age, BMI, gender, laterality, and renal morphology.
Group 1: the branch number 2–4; Group 2: the branch number 5–7; Group 3: the branch number 8–10; Group 4: the branch number >10.
BMI=body mass index.
As listed in Table 2, there was a statistically significant difference about the percutaneous tract number. It showed that calculi with branch number more than five were inclined to increase the number of tract to achieve a higher stone clearance (p<0.001). Middle calices were the most common access for the first tract in all multitract PNL (p<0.001) and the second tract was performed through upper pole with a rate of approximately 75%. In addition, calculi with a branch number more than five needed a higher rate of intercostal tract (p=0.008). Also, there were clinically significant differences with respect to staged PNL (p<0.001), average operative time (p<0.001), and postoperative hospital stay (p=0.043) when stone branch number was more than five. A statistically significant difference was observed about the stone clearance rate that calculi with branch number more than five had lower stone clearance (3 days: p=0.018; 3 months: p=0.004). In the study, calculi with branch number ≥5 only had a stone clearance rate of approximately 60% 3 days postoperatively. Even with the supplementary therapy of SWL, the stone clearance rate increased to approximately 70% 3 months later.
Group 1: the branch number 2–4; Group 2: the branch number 5–7; Group 3: the branch number 8–10; Group 4: the branch number >10.
PNL=percutaneous nephrolithotomy; CaOx=calcium oxalate; di=dihydrate; mono=monohydrate.
In our study, average intraoperative blood loss and main stone composition were similar among the four groups. Complications based on the modified Clavien system were compared according to stone branch number in Table 2, and there was no statistically meaningful difference (p=0.46). No significant difference was found for blood transfusion among the four groups (Group 1: 14 patients–10.2%, Group 2: 14 patients–13.2%, Group 3: 12 patients–15.6%, Group 4: 11 patients–16.9%, p=0.51).
Discussion
A staghorn calculus refers to a stone that occupies the renal pelvis and branches into several or all of the calices. Staghorn calculi are classified as partial and complete staghorn according to stone burden. The spatial structure of calculus is ignored in this classification. Ultrasonography, KUB, IVU, and CT are current routine methods used to provide preoperative images of the stone. However, the ultrasonographic images and parameters of renal calculi are mainly dependent on the experience of operators, and KUB or IVU can only provide two-dimensional images of most calculi without detecting posterior or anterior stone branches. 4 To ensure the safety and success of PNL, all-sided accurate preoperative images are essential. CT technology has been improved especially in the field of 3DR imaging for staghorn calculi. 3DR images of staghorn stone can provide precise pictures of its extent and branching. During the diagnosis and therapy for staghorn calculi, 3DR images can present more information than other methods. First, 3DR images give the location, number of the stone branches, and most importantly, the direction of branches and the relative angles between these branches can be presented vividly in the pelvicalyceal collecting system (PCS). 9 Second, 3DR images may be used to make preoperative plans and contribute to orientation, although it is not to be suggested as a routine procedure. 10 The close relationship of stone branches within PCS, the existence of secondary stones in calyces, and the length and width of the stone branches can be obtained from 3DR images. All these variables are useful in deciding the most appropriate calyx and angle for puncture.
The patient and stone-related factors are the main focus of the effects on the percutaneous tract number in the past investigations. Akman 5 reported that previous open renal surgery was found to be a significant factor leading to a higher rate of the multiple tracts. Also, in the studies of Nahas 6 and Hegarty, 7 they all showed that large stone burden played a pivotal role that causes multiple tracts. In addition, our study showed that the stone branch number influenced the ratio of multiple tracts and staged PNL in a statistically significant manner (p<0.001). In this study, we found the following strategies preoperatively according to 3DR images of the calculi: (1) stones with less branches (usually branch number <5) were inclined to undergo single-tract and one-off PNL; (2) calculi with more branches (usually the number ≥5) needed multitract and staged PNL (Figs. 1, 2). Intraoperatively, we also found the following three points: (1) the more branches with branch-target calyx angle less than 90 degrees the calculus had, the more probability to perform multitract and staged PNL there would be (Fig. 1). This point will be what we focus on in our future study; (2) a flexible nephroscope is an important tool to spare tracts. In the study of Xu 11 and Barnaba, 12 they all concluded that PNL and flexible ureteroscopy or nephroscopy are safe and effective for the management of staghorn stone, and this technique spares percutaneous tracts to a large extent; (3) for small branches in the posterior calices not being reached from the target calyx, we pushed them into the pelvis using the needle or guidewire under ultrasonographic guidance to spare percutaneous tracts.
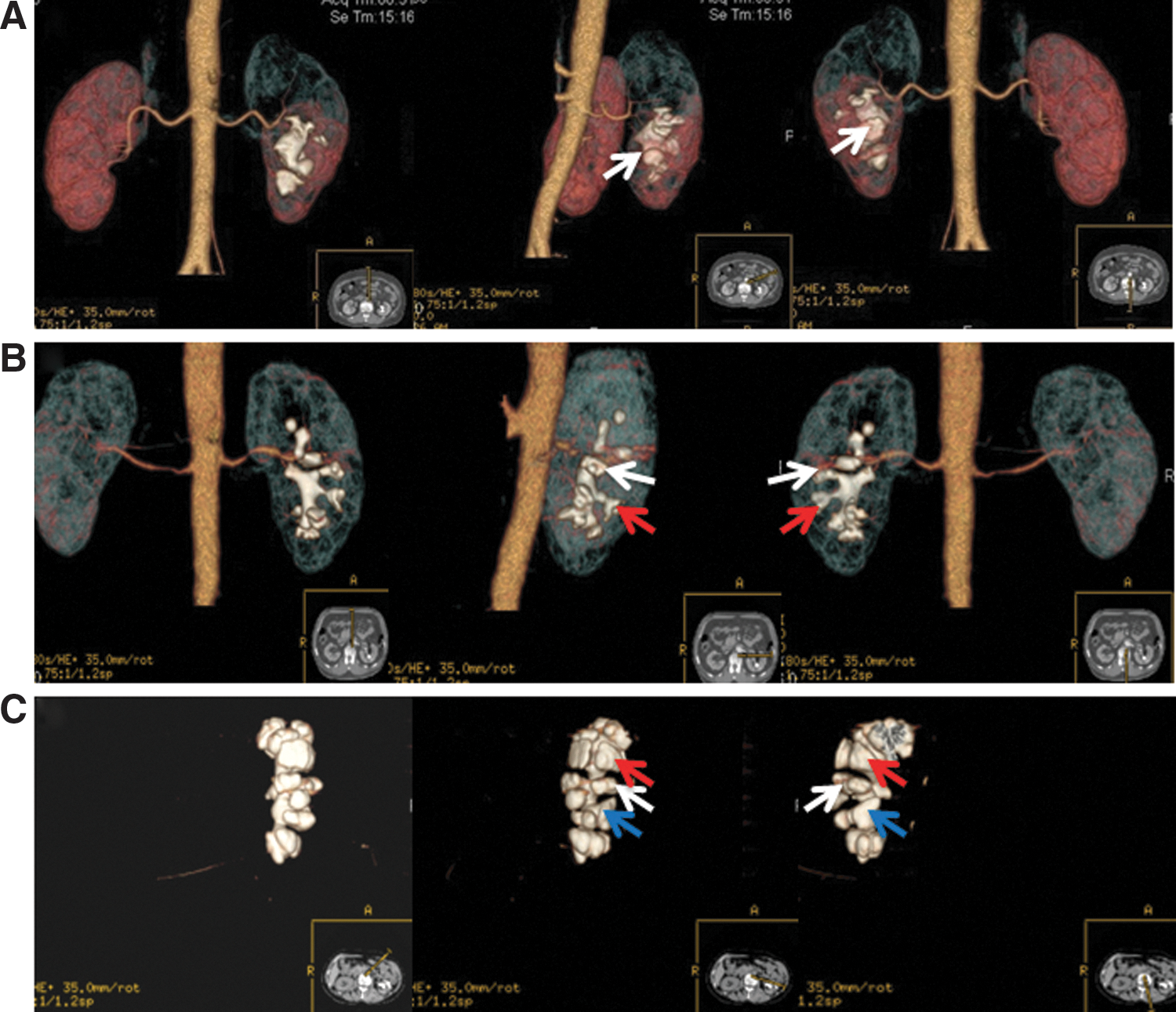
The rotational aspects of three-dimensional reconstruction images show stones with different branch status.

Comparisons of the percutaneous nephrolithotomy (PNL) outcomes among the four groups.
The ultimate goal of surgical treatment for staghorn stones is complete stone clearance. Although endourologic equipments and techniques have been improved, it is challenging for PNL to achieve a stone-free status. There is considerable difference about the stone-free rate of staghorn calculi in the literatures. Al-kohlany 13 reported a lower stone-free rate (49%) when PNL was performed for complete staghorn stones. However, Soucy 14 reported a higher stone clearance rate of 78% with 67% of their patients who had simple partial staghorn stones branching to only one calyx. The total stone clearance rate was 61.6% after PNL monotherapy among our cases. It was lower than the rate published in AUA guidelines, 15 but comparable to the result of 56.9% reported in a PNL global study for staghorn versus nonstaghorn stones. 16 Among the various strategies used for improving the stone clearance, the flexible endoscopy was recommended as a combined therapy to increase efficacy. 17 From Table 2 and Figure 2, it is obvious that the stone-free rate in Groups 2–4 is not satisfactory with the branch number beyond 5, although the flexible nephroscopy was involved. The reasons are as follows: first, we found that there was no enough space for a flexible nephroscope to reach the posterior stone branches in some type of PCS, especially in Sampaio type B1 PCS. Second, we found that 41.8% (46/110) of patients with residual stone had only a clinically insignificant residual fragment (CIRF) in Groups 2–4. Most of these patients were unwilling to accept a second-look flexible nephroscopy or ureterorenoscopy, although the potential perniciousness of CIRF had been informed. Third, in China, flexible endoscopy associated with their calculus-removal devices increases the costs, and that limits their widespread use. By contrast, SWL is still used to manage residual stones in our country.
Staghorn stone had been reported as an important risk factor for post-PNL severe bleeding. 18 The AUA guideline panel on staghorn calculi reported a transfusion rate of 18%. 15 The rate of blood transfusion (10.2%–16.9%) in our study was comparable to the rate published in the guidelines. In our study, the ratio of multiple tracts improved with the branch number increasing, meanwhile, the average operative blood loss has no statistically significant difference (p=0.101) among the four groups. Thus, we could conclude that multiple tracts had not made the blood loss increasing. Although there is the argument against the multitract PNL for a potential to increase bleeding, it has not been substantiated in any published series. Ganpule et al. 19 insisted that a surgeon who can achieve a primary tract can easily create secondary tracts and this does not require a learning curve to be overcome.
In this study, it seems that the postoperative hospital stay are longer in Groups 2–4 than in Group 1 (p=0.043). This can be explained by the staged and multitract PNL for stones with the branch number beyond five. For these patients, the nephrostomy tubes should be removed step by step postoperatively. Several systematic reviews 20,21 have demonstrated that the tube-free PNL is an effective method to decrease the hospital stay. Wang et al. 22 demonstrated simultaneous bilateral tubeless PNL for bilateral renal staghorn calculi, which was associated with short hospital stay and early return-to-normal activity.
The impact of stone branch number on the outcomes of PNL has not been described before, and there is still no evidence about the classification of staghorn calculi based on branch number. In our study, we believed that the more groups we divided, the more reliable the statistical results would be. However, because of the limited sample capacity, we choose 3 as the breakdown between the groups to equalize the number of patients in each group, and which can present the generalizability of this study. The most important limiting aspect of our study is that the spacial relationship of branches was not involved, and we did not take the structure (infundibular width and length) of the calyx occupied by the branch into account. In addition, Clark et al. 23 reported that infundibular width <4 mm might lead to retention of residual stones especially in lower caliceal groups after lithotripsy.
Conclusion
PNL is an effective treatment modality for staghorn calculi; however, the predictors of PNL outcomes continue to be of interest for many urologists. The 3DR images of staghorn stone can provide a precise number of the stone branches. Also, with the stone branch number more than five, the possibility of multiple-tract and staged PNL, lower rate of stone clearance, and longer postoperative hospital stay increases. Therefore, it is necessary for surgeons to be aware and inform patients that PNL of staghorn calculi with branch number more than five may become more complicated.
Footnotes
Disclosure Statement
No competing financial interests exist.