
Abstract
Background and Purpose:
During robot-assisted partial nephrectomy (RAPN) and laparoscopic partial nephrectomy (LPN), clamping of the vascular pedicle before excision of the tumor is the key to minimize blood loss and maintain adequate visualization. Multiple options for hilar control exist, including recently introduced robot-specific bulldog vascular clamps. The relative efficacy of these new clamps has not been assessed. We conducted a comparative analysis of robotic and laparoscopic vascular clamps focusing on clamp force and flow across a clamped model vessel.
Methods:
We compared 10 different vascular clamps used in RAPN and LPN: The Klein robotic; Klein laparoscopic short, medium straight, medium curved, and long; Aesculap short straight, short curved, long straight and long curved; and a laparoscopic Satinsky clamp. Force testing was performed at 1 cm and 2 cm distances from the fulcrum and at the tip. To simulate a clamped vessel, a quarter inch Penrose was clamped and the proximal end attached to a pressure flow monitor. Flow across the tubing at various pressures and leak point pressure (LPP) were recorded. Comparative analysis was conducted using descriptive statistics and t tests.
Results:
The Klein robotic clamp exerted significantly less clamp force along the length of the clamp compared with the laparoscopic placed Klein, Aesculap, and Satinsky clamps (P<0.001). In our vascular model, the Klein robotic clamp had a LPP of 8.3 mm Hg vs 36.3 mm Hg (Klein lap) and >170 mm Hg (Aesculap) (P<0.001). At all pressures, the robotic clamp allowed more flow compared with laparoscopic clamps.
Conclusions:
Robotic vascular bulldog clamps produce significantly less clamping force than laparoscopic bulldog or Satinksy clamps and thus allow more flow across the clamped segment. This difference appears to be intrinsic to the clamp itself. This may translate into poorer hemostasis intraoperatively.
Introduction
Robot-assisted surgery has emerged as an attractive alternative to traditional laparoscopic and open surgery. Since the first robot-assisted radical prostatectomy (RARP) was performed in France in 2000, use of the robot has expanded exponentially. Urologically, the da Vinci robotic system has been described for use in nearly the entire breadth of our field, including radical and partial nephrectomy, prostatectomy, cystectomy with urinary diversion, advanced reconstruction, complicated ureteroscopy, single port and natural orifice surgery, and even vasectomy.
During the past 10 years, there has been widespread adoption of the da Vinci robotic system. 1 –3 As of March 2013, there are 2025 da Vinci robotic systems in use in the United States alone. 4 As the system has become more available, laparoscopic partial nephrectomy has given way to robot-assisted laparoscopic partial nephrectomy as a more common approach at large academic institutions. 2 Additional features such as robotic arms that can apply clips, robotic suction irrigators, and robotically applied vascular clamps have been added to increase the functionality of the da Vinci platform. Many of these additional features, however, have not been compared with the laparoscopic instruments they are meant to replace.
During robot-assisted partial nephrectomy (RAPN) and laparoscopic partial nephrectomy (LPN), clamping of the vascular pedicle before excision of the tumor is a key step in minimizing blood loss and maintaining adequate visualization. This is especially important in minimally invasive surgery, so the reliability of equipment is of the utmost importance. After adopting the robotically applied clamps, we noted several occasions with higher than anticipated bleeding. We hypothesized that there may be differences in the efficacy of the clamps used. Previously, a large disparity in clamp force was seen when comparing different laparoscopic clamps. Robotically applied vascular clamps, however, were not included in the analysis. 5 The investigators noted differences between clamp type, manufacturer, as well as jaw/teeth features that changed clamp force and translated into disparities in flow across their model vessels.
We sought to assess efficacy and differences in robotic vascular clamps when compared with laparoscopic vascular clamps by focusing on clamp force and flow across a clamped model vessel. We propose that these differences in efficacy may affect clamp selection and may affect surgical planning.
Materials and Methods
We compared 10 different vascular clamps used in RAPN and LPN at our institution: The Klein robotic (Klein Robotic, Inc., San Antonio TX), the Klein laparoscopic (short, medium straight, medium curved, and long), the Aesculap (Aesculap, Inc., USA, Center Valley, PA) laparoscopic (short straight, short curved, long straight and long curved), and a laparoscopic Satinsky (Aesculap) clamp. All clamps used for the study came from active hospital inventory and are currently used in surgery at our institution. Notably, the Klein robotic clamps were used three times operatively before force/flow testing. All other clamps had been in active inventory for more than 1 year.
Force testing
Force testing was performed using a Dillon GL100 (Brecknell-GL100) handheld force gauge at 1 cm and 2 cm distances from the fulcrum and at the tip. Each clamp was tested three times at each distance and then the force was averaged for each distance. There were two separate but identical Klein robotic and Aesculap short straight clamps available. Each clamp was included in analysis.
Flow/leak point pressure (LPP)
To roughly simulate a clamped vessel's compliance and elasticity as well as tissue thickness, a quarter-inch Penrose drain was clamped and the proximal end attached to a dynamic infusion cavernosometry and cavernosography machine (DICC) (model 1721 Cavropump by Life Tech Inc.) that assessed flow and pressure while simultaneously generating pressure by infusion. Flow across the vessel at various physiologic pressures from 75 to 170 mm Hg was assessed as well as LPP, defined as >5 mL/min.
Comparative analysis was conducted using descriptive statistics and t tests.
Our experimental setup can be seen in Figure 1. Pictured is the DICC machine attached to our Penrose drain vascular model using standard hospital intravenous line tubing. The inset highlights the Aesculap long straight clamp being tested.
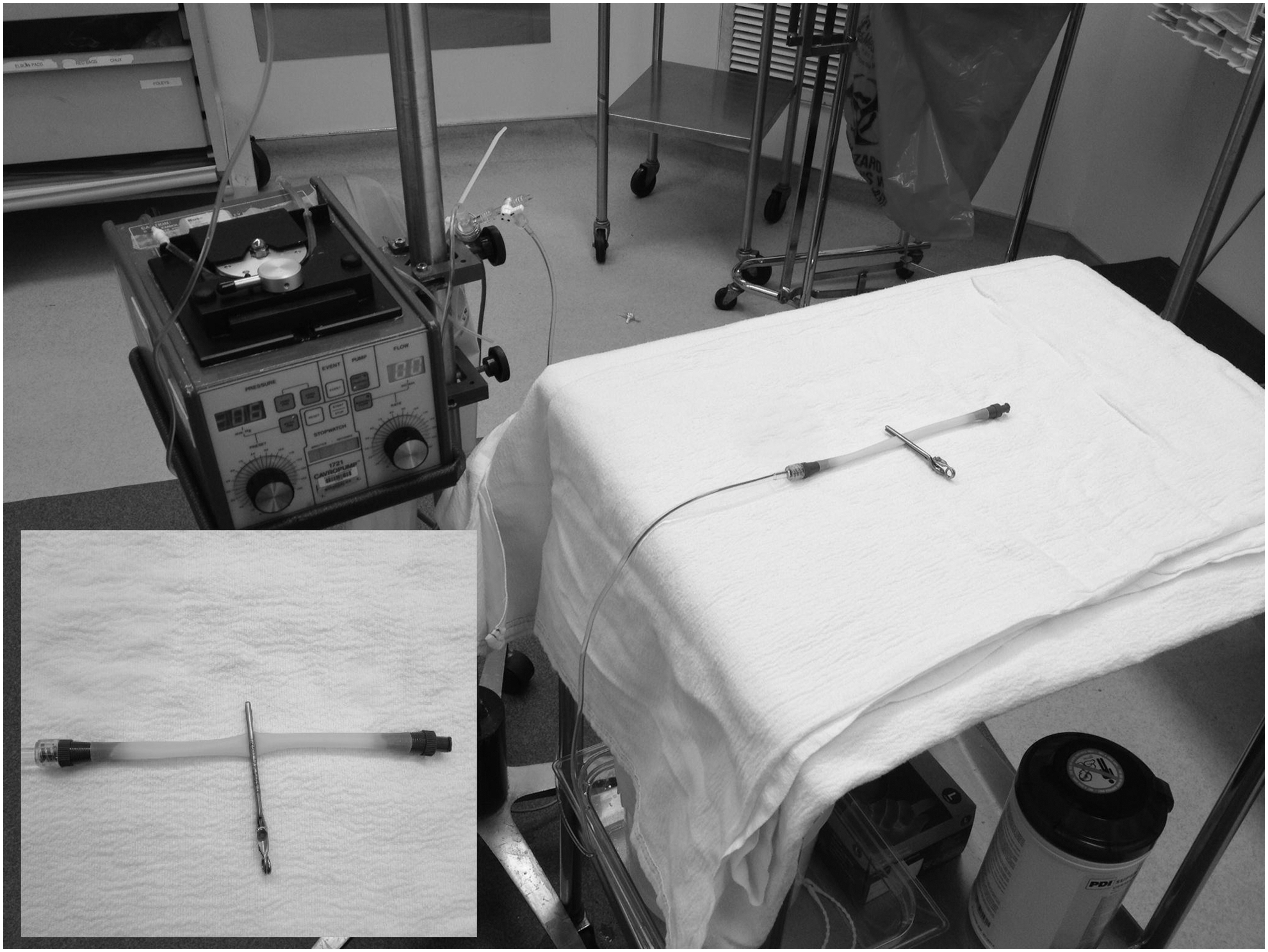
Experimental setup. Inset features long straight Aesculap vascular clamp.
Results
We noted differences between laparoscopic and robot-applied vascular bulldog clamps across the 10 tested clamps (Table 1). The robotic clamps produced the least closing force, 0.36 kilogram-force (kgf) (±0.05 kgf), 0.28 (±0.05 kgf), and 0.24 kgf (±0.02 kgf) at 1 cm, 2 cm, and the tip, respectively. All laparoscopically applied clamps had significantly greater closing forces at all measured distances. Overlap was seen between brands depending on the configuration—straight vs curved (Fig. 2). Both the straight and curved Aesculap clamps provided more force than the Klein straight and curved laparoscopic clamps at all distances. These differences were statistically significant (P<0.01).
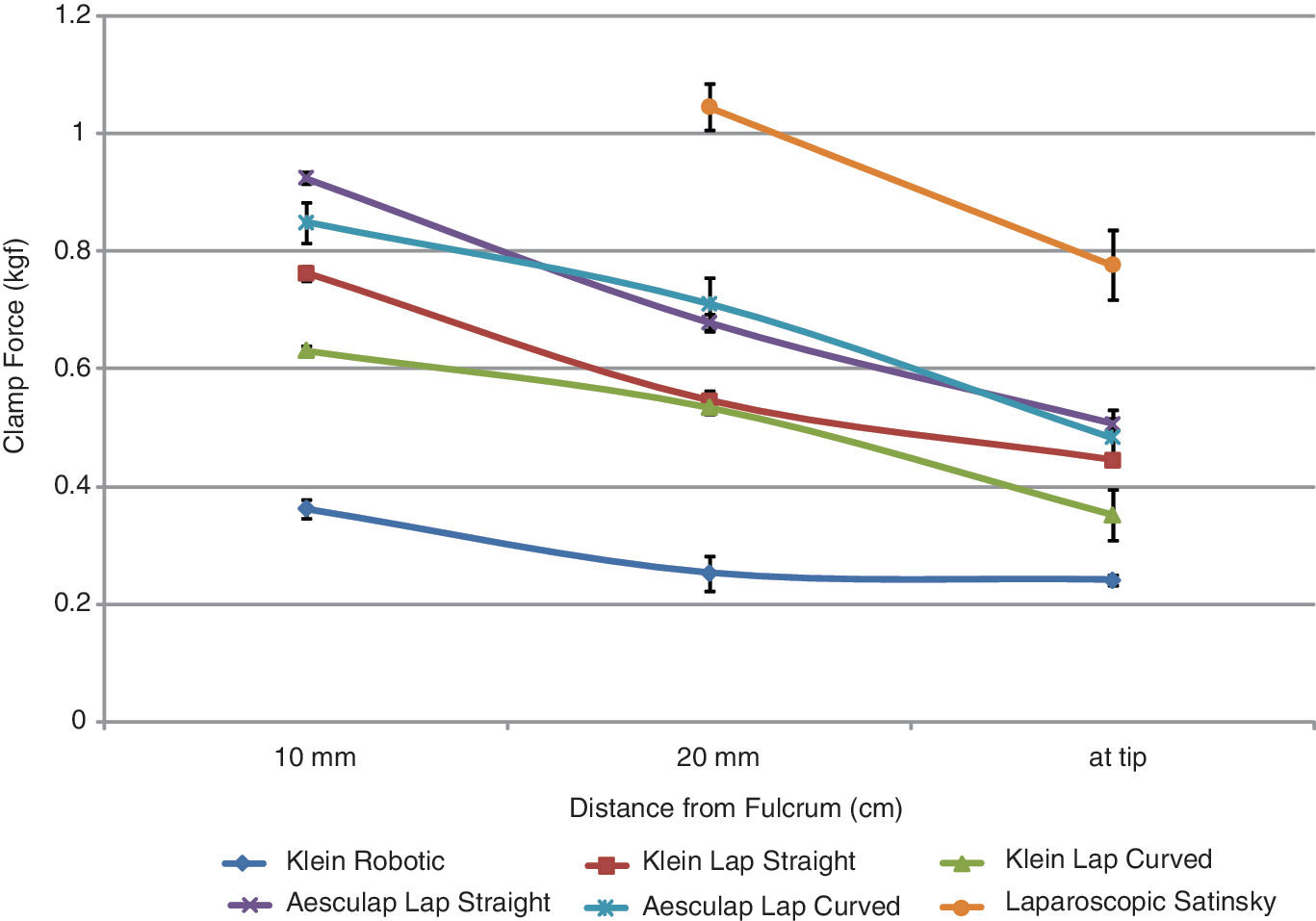
Clamp force at distances 1 cm, 2 cm, and at tip of clamps.
Forces of 10 Tested Clamps
Lap=laparoscopic; kgf = kilogram-force.
In all clamps, the closing force diminished the further from the fulcrum it was tested, with some clamps producing approximately half as much force at the tip as 10 mm from the fulcrum. None of the laparoscopically or robotically applied bulldog clamps provided as much force as a laparoscopic handheld Satinsky.
When tested in a simulated model of flow with a pressure of 75 to 170 mm Hg, the laparoscopic Satinsky and Aesculap clamps allowed no flow across the vessel at normotensive pressures; very little flow was seen at hypertensive pressures in the Aesculap straight and curved clamps. The Klein laparoscopic bulldog and Klein robotic clamps allowed increasing degrees of flow at various pressures (Fig. 3). At 100 mm Hg, the robotic clamp allowed 45 mL/min of flow, which increased with higher pressures.

Rates of flow for clamps at various pressures.
At 150 mm Hg of pressure, the Klein robotic still permitted flow with clamps placed serially. Two clamps in series slowed flow to 34 mL/min, three clamps to 15 mL/min, and with four clamps in series, there was still greater than 10 mL/min flow.
Similarly, when assessing leak point pressures, defined as >5 mL/min, the robotic clamps fared poorly. The Klein robotic clamp's LPP was roughly 8 mm Hg. For the Klein laparoscopic, the straight clamps allowed significant flow at 36 mm Hg, and the Klein laparoscopic curved clamp allowed flow at 15 mm Hg. All other clamps prevented flow up to pressures of greater than 170 mm Hg.
Discussion
Proper vascular control during any minimally invasive surgery is essential in keeping good visualization for adequate tumor resection and minimizing blood loss. Even further, difficulty controlling vessels can necessitate conversion to an open operation. This conversion can potentially increase the morbidity of the procedure by reducing the classic benefits of laparoscopic surgery, such as shorter hospital stay, less bowel manipulation, and better cosmetic results, and can also lead to increases in infection and even further blood loss. 6 Given that robot-assisted laparoscopic vascular clamps are used during critical portions of major urologic cases—deep venous complex ligation, clamping of the renal hilum before partial nephrectomy—it would behoove both the surgeon and the patient to have reliable clamps with maximum efficacy.
This study was undertaken after several anecdotal episodes in which vascular control during RAPN or radical nephrectomy was not optimal despite good visualization of the vessels and appropriate use and placement of the robotically applied clamps. What we found in the first comparison of various robotic and laparoscopic vascular clamps was a large disparity in clamp strength and subsequently flow limitation abilities among different clamps.
Before this study, Lee and associates 5 showed there was a disparity between laparoscopic clamps and the traditional handheld clamps used in open surgery. Our study similarly showed that there is a significant disparity between emerging and established technology. We, too, found that the laparoscopic Satinsky clamp was the most reliable, confirming both a significantly higher clamp force than the other clamps and also a mean flow rate of zero, including at pressures far beyond physiologic conditions that would be experienced during surgery. On the other end of the spectrum, the Klein robotic clamp allowed alarming flow rates, even when placed in series. During a 20-minute clamp time, even with two Klein robotic clamps in series on the artery, by our measurements, roughly 600 mL of blood would make it past the clamp. Of course, this does not necessarily translate into 600 mL of blood loss because the intrinsic resistance of the arterioles, filtration system, and venuoles add to the resistance and protect against blood loss.
We confirmed that bulldog clamp strength decreased the farther away the vessel is from the fulcrum when clamped, with the ideal distance being approximately 1 cm from the fulcrum. This was true across all brands. As expected, the clamps with better grip strength also better reduced flow across a model vessel.
We also noted significant differences between different brands of laparoscopic clamps, possibly because of different fulcrum mechanisms, with Aesculap using a coiled spring and Klein relying on resistance of clamp material for closure strength.
The most surprising and concerning finding was the significant difference between the Klein robotic clamps and all laparoscopic clamps, including those of the same brand. Clamps from the same company showing this great a disparity in clamp force suggests a conscious alteration to adapt the clamp to the robotic rather than to the need of the operation. It is reasonable to posit then that the strength of the fulcrum/pin mechanism is limited by robotic grip strength to open and close the bulldog clamp. It is also reasonable to assume that this strength is limited as a result of safety issues in handling delicate tissue.
Interestingly, Mucksavage and colleagues 7 found that grip force differed among the different da Vinci robotic systems (standard, S, Si), was related to the arm instrument design itself, and could be influenced by deflection of the EndoWrist technology. The greatest force generated in their study was with the Hem-o-lok clip applier, roughly 38 Newtons, or 3.9 kgf, significantly higher than any value generated by our clamps. This suggests that an adequate generator force is possible in the robotic arms. The Klein robotic is placed with the ProGrasp forceps, which is meant to handle tissue, but this could explain the inherent limitation of the clamp. The ProGrasp forceps in the Mucksavage study, however, was shown to have a grip strength of approximately 17 Newtons, regardless of the da Vinci system used. This is a strong fact against the robot itself being the force limiting step in our study and effectively narrows the limitation down to the inherent weakness of the clamp itself rather than the placement tool.
As far as the lack of increased total resistance when the clamps are placed in series, the reason is unclear at this time. Using basic physics principles, the placement of a resistive force in series should add up to a near summation of the total resistances. Intraoperatively, this may be influenced by nonideal placement because of lack of physical space, but on the bench, it is unclear why the appropriately placed clamps in series did not yield the theoretic change.
Our findings were certainly generalizable to other brands, because it seems the limitations of the clamps are likely from the clamp design itself. Furthermore, by examining pressures in the physiologic range, these differences in clamp strength are likely to be of clinical importance and explain the intraoperative observations.
Based on the findings of this study, we now favor laparoscopic placement of vascular bulldog clamps over robotic placement at this time. The Aesculap brand laparoscopic clamps have higher grip strength than the Klein equivalent. The limited advantages of robotic placement, such as alternative angles of placement, are offset by the decreased hemostatic control, and in most situations, an assistant can get an adequate approach angle. Particularly when space is limited, a single well-placed laparoscopic bulldog clamp is superior to the time and effort of multiple clamps placed serially. We believe that these findings may alter intraoperative decision-making at a critical portion of robotic surgery of the kidneys.
It should be acknowledged that the disparity seen between the Klein robotic clamp and the other clamps could be potentially because of overuse or a defective clamp. Two different but identical Klein robotic clamps were tested, however, with little variation between the two, and the clamps were essentially new—used only three times before testing. Therefore, we have low suspicion that this is the case. Further, it should be noted that the other clamps were more widely used and retained their closing force.
Our study was limited by a few factors. First, in previous studies, animal vessels were used to better simulate the compliance properties and laminar flow resistance of human vessels. Second, translatability from our benchtop study using a Penrose drain, which does not take into account tissue resistance to flow from the kidney in vivo as previously discussed, could potentially have led to a less accurate true resistance than simply what was exerted by the clamp.
Conclusions
Robotic clamps do not provide the same clamp force and allow for more flow when compared with their laparoscopically placed counterparts. The reason for this was originally through to be almost entirely because of the limitations on the robotic grip strength, but it is more likely inherent in the clip itself. Theoretically, the grip strength mechanism on the robot is adequate to create the force necessary to apply clips with significant grip force potential. Until the clamps themselves are able to exert relatively more pressure, we recommend placing vascular bulldog clamps laparoscopically.
Footnotes
Disclosure Statement
No competing financial interests exist.