
Abstract
Purpose:
To compare the performance of voluminous benign prostatic hyperplasia patients who have received laparoscopic simple prostatectomy (LSP) with the patients who have received bipolar transurethral resection of the prostate (B-TURP) in their perioperative and 3-year follow-up period.
Methods:
Ninety patients with prostate volumes >80 mL (range 80–130 mL) were randomly assigned to either LSP or B-TURP surgery type. The patients were followed up at 1, 3, 6, 12, 24, and 36 months postoperatively. Perioperative and follow-up characteristics were then recorded and compared.
Results:
More blood loss, greater resected adenoma volume, and shorter catheterization duration were recorded in LSP group than that of B-TURP group (140.1±81.5 vs 93.1±54.0 mL; 65.3±13.8 vs 49.0±12.7 mL; 3.3±1.2 vs 3.8±1.0 days; p<0.05). None of the patients in LSP group reported complications out of 30 days, while 1 case of urethral stricture, 36 cases of retrograde ejaculation, 1 case of bladder neck contracture, and 2 cases of recurrence were recorded in B-TURP group. At 1, 3, 6, and 12 months postoperatively, there were no significant differences in terms of postvoid residual urine volume, maximal urinary flow rate (Qmax ), and International Prostate Symptom Score between the two groups (p>0.05). In contrast, the differences became significant at 24 and 36 months (p<0.05).
Conclusions:
Compared with B-TURP, LSP with Madigan technique is accompanied by less residual adenoma, shorter catheterization time, and more blood loss. Further, the risk of late complications is lower with LSP and, in terms of functional outcomes, LSP appears to be better than B-TURP beyond 2 years.
Introduction
T
With the progression of peritoneoscopic techniques and the drive to apply minimally invasive approaches to most surgical procedures, the feasibility and safety of laparoscopic simple prostatectomy (LSP) compared with the OP has been demonstrated again and again during the past nearly 10 years, since the first report regarding LSP was published by Mariano et al. (2002). 7 –10
On the other hand, as one of the promising innovations of TURP in itself, bipolar TURP (B-TURP) gets rid of the restriction of operative duration and the risk of TURS in traditional monopolar TURP (M-TURP), and is as safe and effective in tackling the large prostate (>60 mL) as has been reported in the resection of small and medium-sized adenoma. 5
As far as we know, no group to date has focused on the control study between LSP and B-TURP for large prostatic glands. We initially compare the perioperative and follow-up parameters of patients between LSP and B-TURP for BPH >80 mL, and report the complications and functional outcomes of the two surgical modalities during a 3-year follow-up period.
Materials and Methods
General things
From June 2008 to April 2010, a total of 90 patients (age range 56–88 years) were recruited into our study, who had a diagnosis of BPH with standard indications for surgery and prostate volumes >80 mL (range 80–130 mL) determined by transrectal ultrasonography (TRUS). Standard indications for surgery were symptoms associated with BPH and recurrent retention (24 patients, 26.7%), upper tract hydronephrosis (5 patients, 5.6%), recurrent hematuria (17 patients, 18.9%), recurrent urinary tract infection (11 patients, 12.2%), and failed medical management (43 patients, 47.8%). All the patients with failed medical management had received finasteride of 5 mg/day for over 6 months before surgery. The patients were excluded with neurogenic bladder, urethral stricture, vesical tumor, prostatic carcinoma, bladder calculus, vesical diverticulum, and previous prostate, bladder neck, or urethral surgery. The recruiters randomly received either LSP or B-TURP, according to the odd and even hospital numbers. All the surgeries were conducted by the same surgical group, after receiving the institutional ethics committee approval and informed consent of all the study subjects.
Surgical procedures
LSP with Madigan technique
After an 18F Foley catheter was introduced to drain the bladder, the patient, under general anesthesia, was placed in a slight Trendelenburg position, followed with routine sterilizing and draping. There were no variations in the number or position of operative ports, compared with the Millin technique that utilizes extraperitoneoscopic approach previously reported. 11 High-flow carbon dioxide insufflations were used up to 10 to 15 mm Hg. The laparoscope was inserted through the infraumbilical 10-mm trocar, and the whole process was conducted visually. To start with, the Retzius space was dissected bluntly, and the influential fatty tissues were swept gently, with the aid of ultrasonic scalpel and hemostatic forcep. After opening the endopelvic fascia on the lateral sides of the prostate, the vesical-prostatic junction was clearly identified via moving the catheter. Two hemostatic sutures of 2-0 Vicryl were placed in the region of the dorsal vein complex, and two more cross sutures were located at 5 and 7 o'clock positions if necessary. A transcapsular incision of 3 to 5 cm was deepened by coagulation, as close as possible to the junction of bladder neck and prostate, aiming to adequately expose the plane between the surgical capsule and the gland but to keep away from vessels. The isthmus was opened toward the apex by ultrasonic scalpel, so that the prostate was divided into two separate lobes. Then the nattier blue urethra could be distinctly recognized between the two lobes. Each lobe was sharply and carefully peeled off the urethra, until the whole adenoma was freed, and the urethra was fully preserved. Figure-of-eight sutures of 3-0 Vicryl were placed in case of urethral cleavage. The specimens were placed outside the capsule and then running sutures of 2-0 Vicryl were placed to close the prostatic capsule, securing the wall of the urethra. The nodules were placed into a bag and extracted through the suprapubic port with the aid of a claw forcep, and overlarge glands were morcellated manually if necessary. Then a suction drain was inserted into the Retzius space through a lateral trocar. About 30 to 60 mL of saline solution was injected into the balloon, and the catheter was pulled and fixed to the thigh within 24 hours. Continuous bladder irrigation (CBI) was not necessary only if the urethra had been cleaved.
B-TURP
The patient received continuous epidural anesthesia and was placed in the lithotomy position. Gyrus PlasmaKinetic system was utilized in the procedure, with settings of 160 W for cutting and 80 W for coagulating. A 26F resectoscope was inserted into the bladder to screen the pathological vesical mucosa and the position of urethral orifices and then retrograded to observe the range between bladder neck and the proximal of verumontanum under direct vision. The resection was started at the 6 o'clock of bladder neck, until deepening into the surgical capsule. The mid lobe and the lateral lobes were resected in a clockwise direction. By and large, the operative modality was similar to the conventional M-TURP. At the end of the procedure, the scattered gland tissues were sucked out via ELLIK. A 22F three-way Foley catheter was inserted and CBI with saline solution was performed. Certainly, traction and fixation of the catheter was essential, with the aid of injecting 30 to 60 mL of saline solution into the balloon according to the size of gland and was relieved within 24 hours.
Data collection and analysis
Preoperative evaluation
Patients' age, red blood cell count, hemoglobin, urinalysis, postvoid residual urine volume (PVR), maximal flow rate (Qmax ), prostate volume on TRUS, and secrum prostate specific antigen (PSA) level were determined before every operation. Transrectal ultrasound-guided needle biopsy of the prostate was performed to rule out adenocarcinoma whenever the secrum PSA level was >4 ng/mL or digital rectal examination findings were suspicious. International Prostate Symptom Score (I-PSS), quality of life (QoL) score, and International Index of Erectile Function (IIEF) were administered to all the patients.
Intraoperative and postoperative evaluations
Operation time, estimated blood loss (EBL), confusions to OP, red blood cell count and hemoglobin of postoperative day 1, catheterization time, CBI duration, suction drain removal, and postoperative hospitalization duration were recorded, as well as intraoperative complications. Hemorrhage was defined as bleeding during the procedure that required transfusion. And the intraoperative blood loss of B-TURP was estimated with Ungjaroenwathana et al. 12 methodically. CBI was discontinued only when the catheter drainage became clear, and suction drain was removed only if the drainage within 24 hours was <10 mL. All patients were discharged from the hospital the next day or the third day after catheter removal, barring unforeseen complications. We also recorded complications in postoperative hospital time.
Pathological analysis
Excised adenoma were weighed and recorded. All pathological analyses were implemented by two or more experienced pathologists.
Follow-up assessment
Follow-up was, respectively, performed at 1, 3, 6, 12, 24, and 36 months after surgery, and the items were composed of PVR, Qmax , serum PSA level, I-PSS, QoL, and IIEF scores. Early and late complications were recorded. We defined early complications as that occurred within 30 days after surgery, and the late ones as that happened out of 30 days. Clavien system 13 was utilized to classify the complications.
Statistical analysis
The Statistical Package for the Social Science 16.0 software was utilized for data analysis. Quantitative statistical description was applied to evaluate all study variables, and statistical results were presented as mean±SD or median (min-max) according to the distribution types. The differences of variables between the two groups were analyzed with independent-sample t-test, or Mann–Whitney test. Paired-sample t-test was utilized to analyze the differences of variables before and after the treatment within the same group. Proportions were compared with Chi-square test or Fisher's exact test. The differences in all analyses were considered statistically significant only if p-value<0.05; if not, then the instances were explained.
Results
Baseline characteristics and perioperative outcomes
Preoperative baseline characteristics of both groups are shown in the upper portion of Table 1. There were no significant differences between the two groups in terms of age, prostate volume, PVR, Qmax , serum PSA level, RBC count, hemoglobin, I-PSS, QoL, and IIEF-5 scores.
Median (min-max) for non-normally distributed variables. The rest normally distributed variables are presented as mean±SD.
Independent-sample Mann–Whitney test. The rest p-values were acquired by independent-sample t-test.
B-TURP=bipolar transurethral resection of the prostate; CBI=continuous bladder irrigation; EBL=estimated blood loss; IIEF=International Index of Erectile Function; I-PSS=International Prostate Symptom Score; LSP=laparoscopic simple prostatectomy; PSA=prostate specific antigen; PVR=postvoid residual urine volume; Qmax =maximal urinary flow rate.
The lower part of Table 1 presents the intraoperative and postoperative variables. No significant difference was discovered in terms of operation time between the two groups (101.7±22.8 minutes for LSP group vs 95.4±18.6 minutes for B-TURP group; p=0.154). The excised prostate volume of LSP group is 65.3±13.8 mL, greater than that of B-TURP group (49.0±12.7 mL; p<0.001). More EBL was recorded in the LSP group (140.1±81.5 vs 93.1±54.0 mL in the B-TURP group; p=0.001). Parallelly, perioperative decrease in RBC count and hemoglobin of LSP group were more than that of B-TURP group; they were, respectively, (1.3±0.5)×1012/L vs (0.7±0.5)×1012/L (p=0.001) and 2.0±0.9 g/dL vs 1.4±0.8 g/dL (p=0.001). One patient in LSP group experienced blood transfusion, and the incidence of blood transfusion was 2.8%. During hospitalization, patients in LSP group experienced shorter duration of catheterization than patients in B-TURP group (3.3±1.2 vs 3.8±1.0 days; p=0.026). Only three patients in LSP group received CBI because of urethral cleavage, while every patient was conducted CBI in B-TURP group, and the mean CBI duration was 28.9±12.2 hours. In addition, patients in LSP group experienced suction drain duration of 25.3±9.4 hours. There was no difference in terms of postoperative hospitalization between LSP and B-TURP groups (4.3±1.2 vs 4.7±1.0 days; p=0.116).
Pathological results
All the 90 cases were diagnosed with BPH. BPH plus chronic prostatitis was diagnosed in 9 (25.0%) patients of LSP group and in 12 (23.7%) patients of B-TURP group. And excised specimen weight was 65.3±13.8 g and 49.0±12.7 g, respectively.
Complications
Numbers of the occurrence of complications during various study periods were specifically noted in Table 2. No significant differences were determined between the two groups in terms of intraoperative and postoperative early complications (p>0.05).
Fisher's exact test, bcontinuity correction, cPearson's chi-square.
TUIP=transurethral incision of prostate.
In our study, late complications were observed in the B-TURP group merely. One patient reported urethral stricture 3 months after operation, and regular urethral sounding was necessary. In the medium follow-up period, 36 patients (66.7% vs 0.0% in LSP; p<0.001) complained of retrograde ejaculation. One patient developed bladder neck contracture and was treated with transurethral incision of prostate. Besides, two patients (3.7%) experienced recurrence after 2 years and had to receive reoperations.
Functional outcomes
Table 3 lists serum PSA level, PVR, Qmax , I-PSS, QoL, and IIEF-5 scores measured during the 3-year follow-up. For both groups, the PSA, PVR, Qmax , I-PSS, and QoL were significantly improved at all follow-up intervals compared with the baseline characteristics (p<0.001). At 1, 3, 6, and 12 months, there were no significant differences in terms of PVR, Qmax , and I-PSS between the two groups (p>0.05). In contrast, the differences became significant at 24 and 36 months (p<0.05). No significant differences were observed in terms of PSA, QoL, and IIEF-5 between the two groups at each follow-up interval (p>0.05). Three-line figures were designed to show the change trend of Qmax , I-PSS, and QoL between the two groups in various periods (Figs. 1 –3).
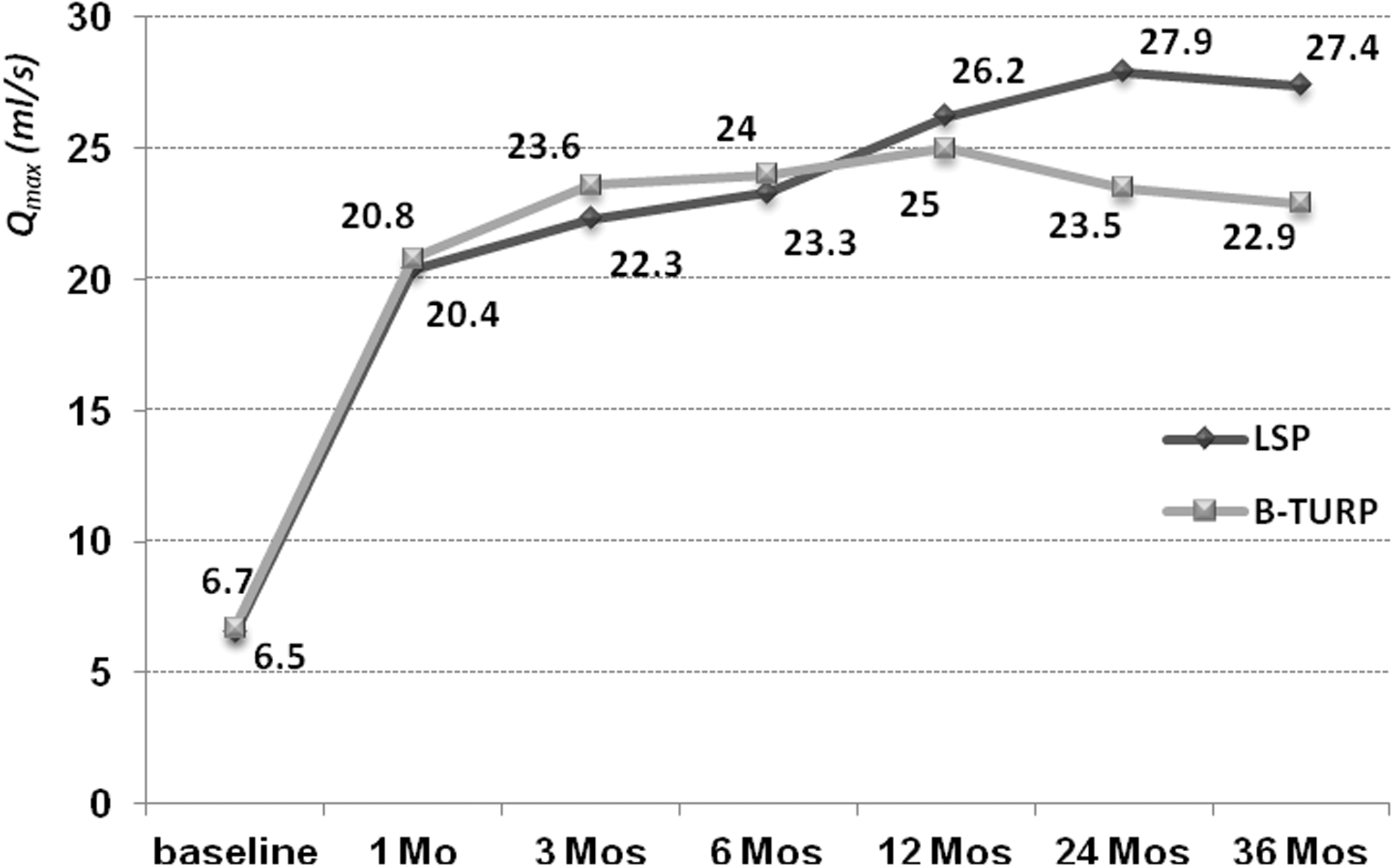
Efficacy profile: mean maximal urinary flow rate (Qmax ).
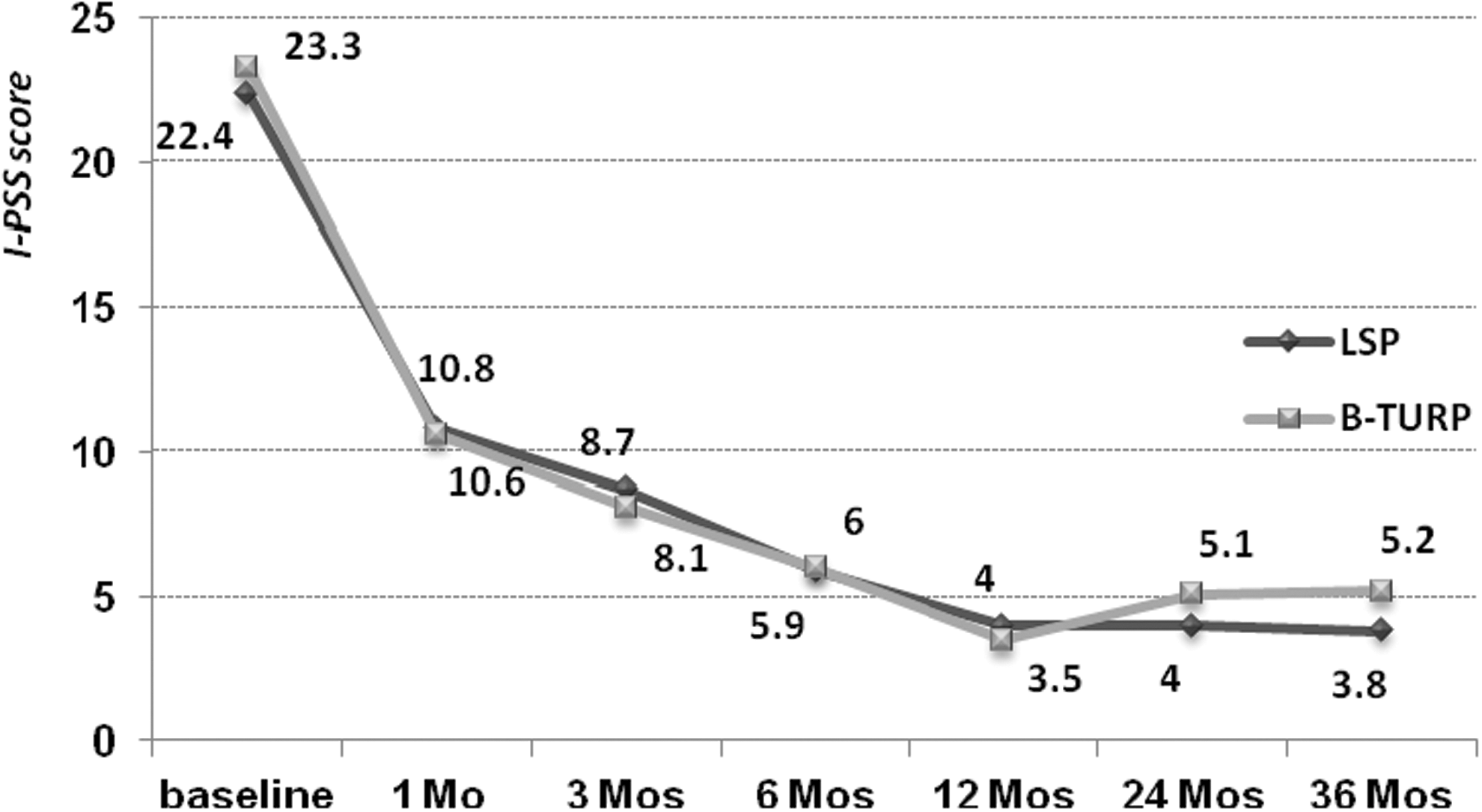
Efficacy profile: mean International Prostate Symptom Score (I-PSS).
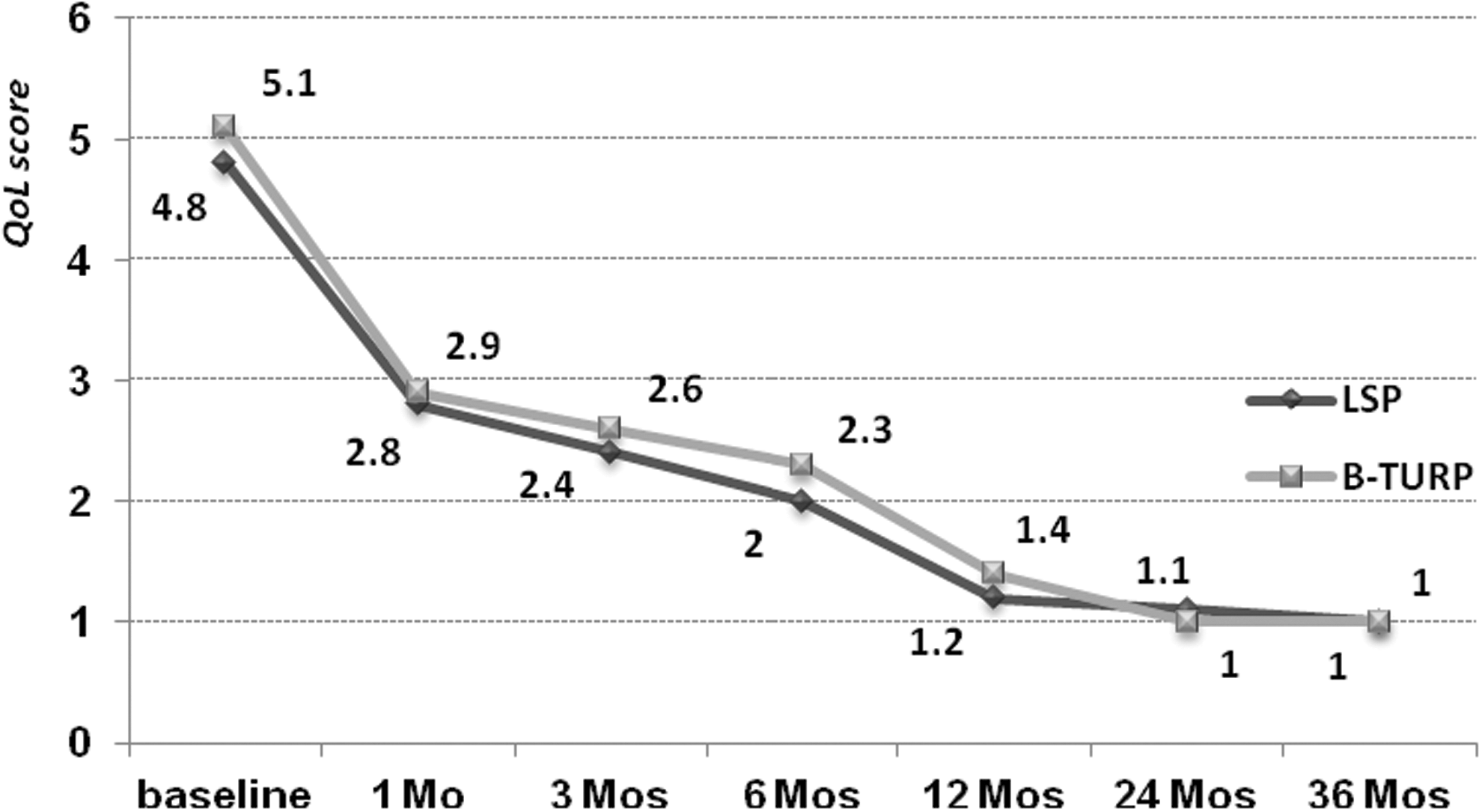
Efficacy profile: mean quality of life (QoL).
Median (min-max) for non-normally distributed variables. The rest normally distributed variables are presented as mean±SD.
QoL=quality of life.
During the 3-year follow-up, two patients in the LSP group and one in the other group died of irrelevant illness (one patient died of hepatoma; the other two died of cardio-cerebrovascular events), and another two patients moved to the other districts, declining for revisit. The proportion of defaulters in the two follow-up groups is both 5.6%. At last, 85 patients (34 patients in LSP group and 51 in B-TURP group) completed the whole follow-up procedure.
Discussion
Urological domain seems to be approaching an era characterized by minimally invasive surgical procedures. It is somewhat understandable that the popularity in finding alternatives to OP for BPH due to a large-volume prostate is spiraling up, although the AUA and EUA guidelines suggest that open approach should be the treatment of choice in patients with a prostate larger than 80 to 100 mL. 1,6
A series of emerging minimally invasive techniques represented by HoLEP, PVP, B-TURP, PkEP, and LSP were confirmed continually to be feasible, safe, and effective for large glands, and naturally there was no lack of control studies among the just mentioned surgical modalities. Elmansy et al. 3 compared the objective and subjective outcomes of HoLEP group with that of PVP group and then considered that HoLEP appeared to be better in the early objective functional results (significant higher Qmax and lower PVR during the entire follow-up) for patients with prostates >60 mL. Zhu et al. 4 developed a prospective randomized contrast trial with 5-year follow-up in a cohort of 80 patients, and came to the conclusion that PkEP was associated with less EBL, shorter hospital stay, and catheterization for BPH patients with prostates larger than 70 mL, and seems to be superior to B-TURP at follow-up longer than 3 years, with fewer reoperations necessary. However, as far as we know, until now there has been no study that compares LSP and B-TURP in the treatment of large prostates. To address this point we developed the present study.
In our study, all the surgeries were conducted by the same group, the core members of which had more than 5-year experience of laparoscopic and transurethral endoscopic surgeries. Even so, we excluded from study the initial 15 cases of LSP with Madigan technique performed before June 2008. In this way, we limited the potential learning curve bias, and the similar means were adopted in the study of Porpiglia et al. 14 During the 3-year follow-up, lost to follow-up proportions in both groups was 5.6%. Therefore, follow-up bias got limited.
Generally intraoperative blood loss is recognized as an important indicator of evaluating surgical safety. The present study revealed that the mean EBL in LSP group was more than that of B-TURP group (140.1 vs 93.1 mL; p=0.001), and the perioperative decrease in RBC count and hemoglobin further demonstrated the result. Effective hemostasis of B-TURP contributed to that bipolar PlasmaKinetic coagulating loop could be used to seal all bleeding points regardless of surgical duration compared with M-TURP. 15 To reduce blood loss in LSP procedure, we carried out at least two reliable techniques: (1) preventative sutures were placed in the region of the dorsal vein complex and 5 and 7 o'clock positions of vesical neck, 16 (2) and the transcapsular incision was placed as close as possible to the vesical-prostatic junction. 17 In the available literatures, the EBL of LSP with Millin and transvesical techniques ranged between 134 and 411.6 mL. 8 –11,18,19 Quan et al. 17 applied Madigan technique to LSP; the mean EBL decreased to 112.5 mL. It seems to be acceptable for the blood loss in our LSP procedure. In spite of a certain gap, it is possible that blood loss in LSP with Madigan technique decreases to even less than the level in B-TURP with the accumulation of experience.
Our results indicated that the resected adenoma volume of LSP was 65.3±13.8 mL, significantly greater than that of B-TURP (49.0±12.7 mL; p<0.001). The resected adenoma volume of LSP was equal to 64.1% of the prostate volume estimated on preoperative TURS. In fact, the proportion was promoted to 79.1% by Quan et al. 17 Therefore, as the operation time was similar, LSP appeared to be more efficient than B-TURP.
Postoperatively, CBI was not necessary for patients with LSP except for three cases due to urethral cleavage (respectively, lasting 6, 6, and 12 hours) in our study, while for B-TURP the mean time of CBI was 28.9 hours. The main reason was that the urethra wall got preserved for the largest possible, which reduced postoperative hematuria effectively. And this also leads to shorter catheterization time in LSP group. There seems to be certain differences for catheterization time in both the B-TURP and LSP groups between our study and some foreign reports. A possible explanation is that the abilities of blood coagulation and natural healing are different among different races. In addition, the superiority of postoperative hospitalization in LSP group was not seen in our study.
When patient data on complications were extracted and analyzed, the morbidity 3 months after surgeries raised certain concerns for us. It was surprising that no one who undergoes LSP with Madigan technique reported late complications. Compared with B-TURP, LSP with Madigan technique preserved the integrity of urethra and the vesical neck, avoided injury on urethral inner and external sphincters effectively, and protected the sound physiology and anatomy, and all these contributed to the low incidence of urethral stricture, retrograde ejaculation, and bladder neck contracture with LSP technique. In addition, two cases (3.7%) had to receive reoperations as a result of recurrence in B-TURP group as opposed to none in LSP group, although the difference was not statistically significant. Zhu et al. 20 reported reoperation rate of 4.5% after 3-year follow-up carried out in 132 patients with B-TURP. Another 5-year follow-up study 4 declared that the recurrence rate after B-TURP was 5%. However, to date few recurring cases were reported in the available literatures on LSP modality. The difference could be induced by less residual adenoma in LSP group.
In terms of functional outcomes, our follow-up results confirmed that both surgical procedures were highly effective for treating large prostates. Because we observed significant improvements at all follow-up intervals compared with the baseline characteristics in terms of the PSA level, PVR, Qmax , I-PSS, and QoL score. Within 1-year follow-up, there were no significant differences in all the values between the two surgical modalities, which demonstrated that both LSP with Madigan technique and B-TURP had comparative short-term treatment efficacy. However, significant differences in terms of PVR, Qmax , and I-PSS score were observed between the two groups at 2 and 3 years postoperatively, which suggested that durability of LSP with Madigan technique appears to be better than B-TURP. In either surgical procedure, IIEF-5 scores did not change over the entire study period, confirming that both LSP with Madigan technique and B-TURP did not affect patient erectile function, which was in accordance with series of previous research results. 4,11,16,17
Still, our study has several limitations as follows: small sample size, single-center trial, and relatively short follow-up period. Multicenter randomized trials with a larger sample size and a longer follow-up are expected to further validate our findings. Minimally invasive surgical procedures are still in development, with the optimal approach for large prostates not yet defined, and more control studies should be made among the surgical modalities for BPH patients with large glands, such as LSP versus PkEP, HoLEP versus PkEP, and so on. For these purposes, randomized control trails and cohort study are needed.
Conclusions
Results suggest that both LSP with Madigan technique and B-TURP are feasible, safe, and effective minimally invasive surgical procedures for BPH patients with prostates larger than 80 mL. Compared with B-TURP, LSP with Madigan technique is accompanied by less residual adenoma, shorter catheterization time, and relatively more intraoperative blood loss. Further, the risk of late complications is lower with LSP and, in terms of functional outcomes, LSP with Madigan technique appears to be better than B-TURP in the follow-up beyond 2 years.
Footnotes
Disclosure Statement
No competing financial interests exist.