
Abstract
Purpose:
Our aim is to evaluate different ureteral access sheaths (UASs), which are available in the international market and their compatibility with different available flexible ureteroscopes (F-URSs) to help the urologist choose the proper ureteral access sheath for his or her endoscope before commencing the procedure.
Materials and Methods:
A total of 21 UASs and 12 F-URSs were evaluated. Measurements were obtained in French (F) units considering different characteristics for each UAS and each F-URS. Insertion test without friction between F-URS and UAS was considered as a successful test and was referred as (YES).
Results:
All UASs and F-URSs were successfully submitted to the insertion test. All F-URSs that were inserted into UASs without friction had an internal diameter of at least 12F. Different lengths of UAS did not influence the test outcome.
Conclusion:
This study was able to establish a correlation table between different UASs and different flexible ureteroscopes. As of now, the 12/14F UAS is considered the universal UAS that accepts all F-URSs that are available in the endourology field. Nevertheless, we are expecting a significant change with the new standard size 10/12F UAS as well as huge advances in minimizing the size of different endoscopes.
Introduction
T
There are different UASs available in the market with different characteristics, different sizes, and lengths. UAS characteristics were modified according to available flexible ureteroscopes (F-URSs); therefore, endoscopes are inserted into UASs without difficulties or friction during flexible ureterorenoscopy. UAS insertion into the ureter depends on the ureter status and on its anatomic varieties. There are individual differences among UASs with similar metrics because of variable manufacturers. 13 The aim of this work is to evaluate different available UASs in the endourology field and their compatibility with different available F-URSs to help urologists choose the proper UAS for their endoscope.
Materials and Methods
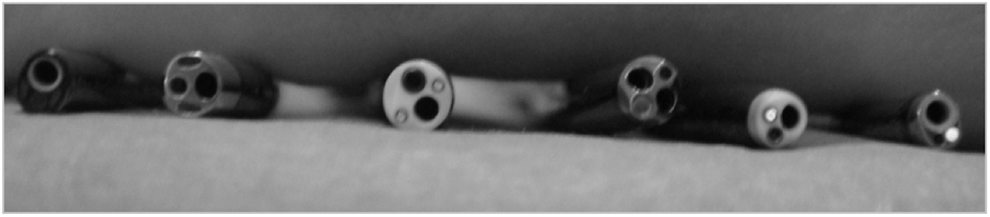
This study was conducted by a single urologist in a wet environment with a subjective evaluation. A total of 21 UASs (Fig. 1) and 12 F-URSs were included. Each UAS inner and outer diameter was measured using French (F) size as well as its length in centimeters (cm). On the other hand, each F-URS size was documented from the diameter on the tip, up to the shaft proximally. An insertion test was performed for each F-URS on different UASs. This test consised of evaluating the possibility of a full F-URS insertion into the UAS. A positive test was noted as YES when the scope was completely inserted into the UAS without minimal friction; otherwise, the test result was considered negative and noted as NO if not compatible. When the insertion was possible but with friction that might reduce the manipulation of the F-URS, the result was recorded as YES* (with small star*).

Different ureteral access sheaths.
Results
Inner diameters of available UASs vary from 9.5F (Flexor - Cook®) to 14F (Flexor - Cook®; Forte - Applied Medical®). Outer diameters vary from 11.5F (Flexor - Cook®) to 18 F (Forte - Applied Medical®).
Proximal F-URS diameters vary from 7.95 F (URF-P6 - Olympus) up to 10.9F (URF-V - Olympus). For digital endoscopes, the Flex-XC (Storz) was found to be the thinnest with 8.5F for the whole length. Among optical (conventional) endoscopes, the URF-P6 (Olympus) was found to be the thinnest with only 4.9F at its distal tip and 7.95F on its shaft proximally. UAS and F-URS characteristics were shown in Tables 1 and 2, respectively. The compatibility results are summarized in Table 3.
Laboratory performed measurement.
UAS=ureteral access sheath.
YES=Free passage of the fexible ureteroscope through the ureteral access sheath.
YES*=The complete passage of the scope is possible but with high degree of friction.
NO=No passage (distal tip of the ureteroscope is larger than the orifice of the sheath).
We found that all UASs that accepted the insertion test of all F-URSs had an internal diameter of at least 12F. On the other hand, the insertion test was negative in all digital F-URSs when performed in a UAS that had an inner diameter of 10F or smaller. F-URSs that could be inserted in Flexor-Cook UAS of 9.5/11.5F (smallest UAS) were Flex-X2 – Storz and URV-P6 – Olympus. The only available dual channel F-URS was Cobra – Wolf, which was successfully inserted into Rocamed® UAS 10F but not into Retrace – Coloplast® UAS 10F without friction.
Digital F-URS (URF-V – Olympus) could be successfully inserted into the 11/13F Navigator - Boston Scientific®; however, it was with friction that decreased endoscope manipulation. Nevertheless, the test was positive with UAS of 12F inner diameter. On the other hand, Digital F-URS (DUR-D - ACMI-Olympus and Flex-XC - Storz) were successfully inserted into 11F UAS without any friction. The smallest UAS that was able to accept the insertion of all F-URS, with or without friction, was the Navigator - Boston Scientific 11/13F. During all insertion tests for all UASs with similar diameters, the length (13–55 cm) did not affect the outcome.
Discussion
For the time being, various conditions are treated by flexible ureterorenoscopy, such as renal stone disease, upper urinary tract transitional-cell carcinoma (UUT-TCC), intrarenal diverticulum, and ureteropelvic junction stricture. 14 To improve procedure efficacy, ureteroscope durability, and reduce costs, the right choice of endoscopes and materials must be prepared for different proposed treatments. Retrograde renal stone treatment usually necessitates many instruments such as stone retrieval devices and laser fibers; thereby, efficacy improved with use of the UAS. 9 For UUT-TCC, use of a smaller UAS and digital F-URS is recommended to reduce ureteral damage. 11 Knowing different UAS sizes and F-URS compatibility will help urologists to define correctly the materials needed for endourologic procedures.
Huge advances of flexible ureterorenoscopy have widened and increased the minimally invasive technique with better outcomes with low morbidity. Correct understanding of UAS and F-URS compatibility will increase F-URS durability as well as reduce operative time with a high success rate. This work was conducted to evaluate the compatibility between available UASs and F-URSs. Technology improvement has brought advances in new designs, fine optics, better ergonomics, and better vision with smaller and more maneuverable endoscopes. Therefore, these changes lead industries to design a new range of UASs following the endoscope characteristics.
Although new technology improved endoscope overall quality, vision, and deflection, it increased the use of UAS to allow introduction of larger tip digital endoscopes, thereby increasing costs and patient morbidity. 15 Failure to choose the right UAS can result from kinking, buckling, and difficulty passing instruments or endoscopes. To improve UAS insertion, new technology has been applied: The impregnated coil design of the sheath, the inner lining with a low coefficient friction, and hydrophilic outer coatings. 16
It is important for urologists to be informed about available materials and instrument characteristics to choose properly the UAS and F-URS that improve the outcome with a safe procedure, low morbidity, and low costs. 17 –19 The right choice of UAS reduced endoscope friction during manipulation and thereby increased durability. 7 Our study was able to identify the universal UAS that could accept all F-URSs. This universal UAS should measure at least 12F in the inner diameter without any concern for its length, because it has no influence on the insertion outcome. An UAS of 11/13F (Navigator - Boston Scientific) can accept all F-URSs; however, the complete insertion of URF-V - Olympus is possible only with high resistance that almost completely limits its maneuverability during the procedure.
An important message is that available F-URS shapes differ from UAS shapes because they do not present with a perfectly circumferential shape but are frequently oval (Fig. 2). This may explain why some F-URSs measuring 8.5F cannot be inserted into 9.5F inner diameter UAS. The oval shape of some F-URSs has limited its insertion inside some UASs even if the French size of its inner diameter is smaller because of the completely round shape of those UASs.
Different shapes of many flexible ureteroscopes.
In fact, the average size of the human ureter is estimated at 10F (3–4 mm), which can explain clearly why an UAS of 12/14F cannot be placed without difficulty. Traxer and Thomas 11 reported in their recent study of 359 patients who underwent flexible ureterorenoscopy for stone disease treatment that 12/14F UAS was responsible for ureteral injury in up to 46.5% of those patients if placed in a routine way.
Up to the present, we rely only on UAS with axial dilation where the force from the UAS varies according to its diameter and, therefore, risk of ureteral damage might occur. Some authors demonstrated a new concept for ureteral dilation by an expandable UAS, with the advantage of possible reduction in risk of ureteral injuries. Although successfully used in a porcine model, it is, to this date, not available for clinical practice. 20 Another significant advantage of this new technology is the fact that it could overcome the concerns regarding UAS size and F-URS compatibility, because we could theorize that “one would fit all.”
In this study, 10/12F UAS from Retrace - Coloplast® and Forte - Applied Medical had accepted all testeThe Rocamed 10/12F UAS was able to accept all the tested endoscopes but not URF-V - Olympus; however, an important point must be addressed here regarding its inner diameter, which was measured in our laboratory and found to be 10.9F instead of the 10F as was advertised by the manufacturer.
As a result of constant technology research, we are frequently presented with an increase in endoscope miniaturization, which will no doubt soon make the 10/12F UAS the reference for accepting all available F-URSs. The UAS-related complication rate from ureteral injuries is also expected to be considerably reduced with smaller diameter UASs and F-URSs. It is therefore essential to know the available materials and devices to respect patient anatomy by adapting equipment to the patient and not the reverse.
Conclusion
From this study, we were able to establish a compatibility table between UASs and F-URSs. Today, a UAS of 12/14F is considered a universal UAS that accepts all available F-URSs. Advances in miniaturization and minimizing the size of F-URSs will quickly see the 10/12F UAS become the new standard UAS that accepts all endoscopes.
Footnotes
Disclosure Statement
Olivier Traxer is a consultant for AMS, Coloplast, and ROCAMED. For the remaining authors, no competing financial interests exist.