
Abstract
Purpose:
To assess the efficacy and safety of thulium laser resection of the prostate (TmLRP) vs transurethral resection of the prostate (TURP) for treating patients with benign prostatic hyperplasia (BPH).
Methods:
A systematic search of the electronic databases, including Medline, Scopus, China National Knowledge Infrastructure, and the Cochrane Library was performed up to May 1, 2013. The pooled outcomes of interest assessing the two techniques included demographic and clinical baseline characteristics, perioperative variables, complications, and postoperative efficacy including maximum flow rate (Qmax), postvoid residual (PVR), quality of life (QoL) and International Prostate Symptom Score (IPSS).
Results:
Nine trials assessing TmLRP vs TURP were considered suitable for meta-analysis including three randomized controlled trials (RCTs), two prospective, and four retrospective studies. Compared with TURP, although TmLRP needed a longer operative time (weighted mean difference [WMD]: 9.00 min; 95% confidence interval [CI], 2.53–15.47; P=0.006), patients having TmLRP might benefit from significantly less serum sodium decreased (−3.58 mmol/L; 95% CI, −4.04 to −3.12; P<0.001), less serum hemoglobin decreased (WMD: −0.94 mmol/L; 95% CI, −1.44 to −0.44; P<0.001), shorter time of catheterization (WMD: −2.07 days; 95% CI, −2.66 to −1.49; P<0.001), shorter length of hospital stay (WMD: −1.87 days; 95% CI, −2.41 to −1.33; P<0.001), and fewer total complications (odds ratio [OR]: 0.29; 95% CI, 0.20–0.41; P<0.001). During the 1, 3, 6, and 12 months of postoperative follow-up, the procedures did not demonstrate a significant difference in Qmax, IPSS, PVR, and QoL.
Conclusions:
Our data suggest that as a promising minimally invasive technique, TmLRP appears to be a safe, feasible, and efficient alternative to TURP for treating patients with BPH with reliable perioperative safety, fewer complications, and comparable efficacy in relation to Qmax, PVR, QoL, and IPSS. Because of the inherent limitations of the included studies, further large sample prospective, multicentric, long-term follow-up studies and RCTs should be undertaken to confirm our findings.
Introduction
B
One of the most significant technical modifications of TURP is the incorporation of bipolar technology. Bipolar TURP technology, including plasmakinetic bipolar resection of the prostate, addresses a fundamental flaw of traditional monopolar TURP by allowing performance in physiologic saline, permitting a longer resection time, and providing improved hemostasis, thus making resection of larger prostates possible without compromising safety. 4 –6
Another minimally invasive surgical treatment for patients with BPH is laser therapy, which is increasingly marketed as a replacement for the gold standard TURP. Thulium laser is a new surgical laser, with tunable wavelength between 1.75 and 2.22 μm. 7,8 It may have several advantages, including improved spatial beam quality, more precise tissue incision, and operation in continuous-wave/pulsed modes. 9 Thulium laser has proved capable of rapid vaporization and coagulation of prostate tissue, 10 whereas cutting and ablation characters are excellent at 50 W energy level.
In recent years, a number of investigators have begun to report case series of thulium laser resection of the prostate (TmLRP) as a novel technology with favorable perioperative safety, the same therapeutic effect as TURP, and the advantage of significantly less blood loss, shorter hospitalization, and shorter catheter indwelling time. 7,8,11 –20 The real advantages of TmLRP over TURP and whether TmLRP can replace TURP as the first-line surgical treatment still remain to be determined, however.
We conducted a systematic review and meta-analysis of the literature on the efficacy and safety of TmLRP vs TURP for treating patients with BPH in terms of demographic and clinical baseline characteristics, perioperative variables, complications, and postoperative efficacy including maximum flow rate (Qmax), postvoid residual (PVR), quality of life (QoL) and International Prostate Symptom Score (IPSS).
Methods
Literature search and study selection
A systematic review of the literature was performed to identify articles published up to May 1, 2013 on the management of symptomatic prostatic obstruction. We conducted a systematic search of the electronic databases, including Medline, Scopus, China National Knowledge Infrastructure and the Cochrane Library, using the terms “thulium laser resection of the prostate,” “TmLRP,” “transurethral resection of the prostate,” and “TURP.” No temporal, regional, publication status, or language restrictions were set. In addition, a full manual search of the references in each relevant article was also conducted.
Inclusion criteria and exclusion criteria
To be included in the analysis, studies were required to: (1) compare TmLRP with TURP, (2) report on at least one outcome of interest mentioned below, (3) clearly document the technique as TmLRP, and (4) clearly document indications for resection of the prostate. Studies were excluded in the meta-analysis if: (1) the inclusion criteria were not met, (2) no outcomes of interest (specified later) were reported or were impossible to calculate or extrapolate the necessary data for either TmLRP or TURP from the published results.
Data extraction and outcomes of interest
Two reviewers (KT and ZhLX) extracted independently the following data including: First author, year of publication, study design, number of patients who underwent TmLRP or TURP, characteristics of the study population, and outcomes of interest. All disagreements about eligibility were resolved by a third reviewer (HX) by discussion until a consensus was reached. The following data were the outcomes of interest that were extracted from each eligible study: Postoperative Qmax, PVR, QoL, IPSS, operative time, serum sodium and hemoglobin decreased, catheterization time, hospital stay, and the overall complications including blood transfusion, TUR syndrome, recatheterization, transitory urge incontinence, stress incontinence, urinary tract infection (UTI), retrograde ejaculation, and urethral stricture.
Study quality and level of evidence
The level of evidence (LOE) of included studies was rated according to criteria by the Centre for Evidence-Based Medicine in Oxford, UK. 21 Two reviewers (KT and ZhLX) independently assessed the quality of the studies and disagreement was resolved by consensus.
Statistical analysis
The present meta-analysis was performed according to the recommendations of the Cochrane Collaboration and the Quality of Reporting of Meta-Analyses guidelines. 22 The WMDs and the odds ratios (ORs) were used to compare continuous and dichotomous variables, respectively. All outcomes were reported with 95% confidence intervals (CIs). For continuous variables, we calculated the difference in mean values and the 95% CI. This method requires that the study report the standard errors of the mean, the standard deviations, or the CIs. Some studies that did not report any of these parameters but presented continuous data as medians and ranges; under this circumstance, we made an approximate transformation using the technique described by Hozo and associates. 23 For dichotomous variables derived from contingency tables, the ORs and 95% CI were computed. An OR significantly <1 favored TmLRP, whereas an OR significantly >1 favored TURP. All P values are two-tailed with a significant level at 0.05.
A fixed-effects meta-analysis was performed, and the quantity of heterogeneity was assessed using χ2 and I 2 statistics with significance set at P<0.05 providing evidence of significant heterogeneity. For outcomes detected with higher values of I 2 and the χ2 statistic signified increasing levels of inconsistency between studies and significant interstudy heterogeneity, then a random-effects meta-analysis model was adopted. Data analysis was performed with the Review Manager Software (RevMan 5.1, Cochrane Collaboration, Oxford, UK).
Results
Characteristics of eligible studies and LOE
Nine trials assessing TmLRP vs TURP were considered suitable for meta-analysis including three randomized controlled trials (RCTs), two prospective and four retrospective studies (Fig. 1). We used the United States Preventive Services Task FTURPe grading system 21 to assess the quality of every study included in our meta-analysis. Of the five prospective and four retrospective studies, three RCT studies 13,14,20 LOE scored 2b, four studies 15 –17,19 scored 3b, and the remaining two studies scored level 4. Also, the number of patients, age, prostate volume, prostate-specific antigen level, and preoperative estimates of baseline Qmax, PVR, QoL and IPSS of TmLRP vs TURP and follow-up times were extracted individually from each study and listed in Table 1.
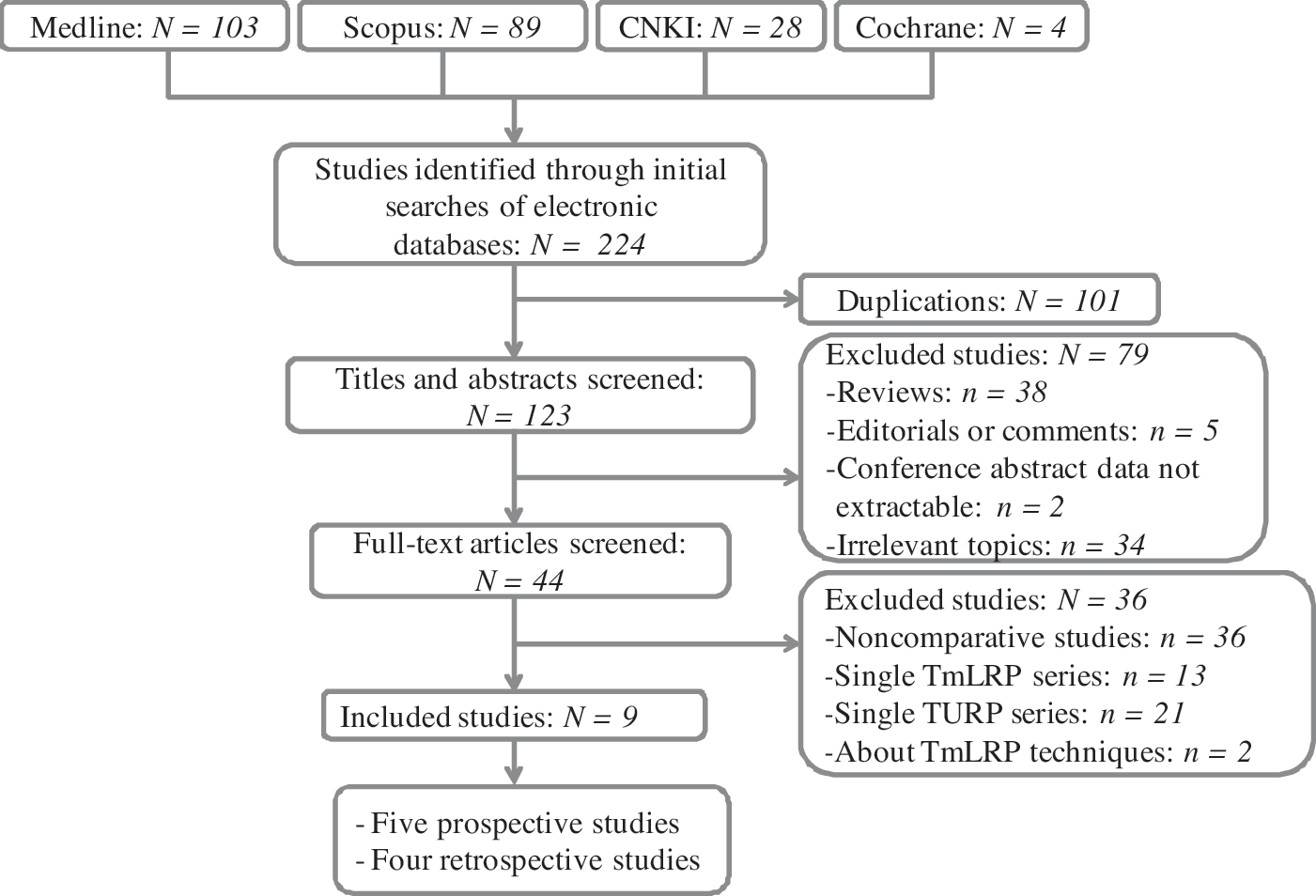
Flowchart showing the selection of studies for meta-analysis. CNKI=China National Knowledge Infrastructure; TmLRP=thulium laser resection of the prostate; TURP=transurethral resection of the prostate.
Based on US Preventive Services Task Force grading system; bpostoperative efficacy parameters review during follow-up.
LOE=level of evidence; PSA=prostate-specific antigen; Qmax=maximum urinary flow rate; PVR=post-voiding residual urine volume; QoL=quality of life score; IPSS=International Prostate Symptom Score; TmLRP=thulium laser resection of the prostate; NA=not available; M-TURP=monopolar TURP; RCT=randomized controlled trial; B-TURP=bipolar TURP.
Outcomes of postoperative efficacy variables including Qmax, PVR, QoL, and IPSS
Qmax
No significant difference was observed in TmLRP compared with TURP about Qmax (weighted mean difference [WMD]: 0.05; 95% CI, −0.43–0.52; P=0.85) during the postoperative 1, 3, 6, and 12 months follow-up, and there were no significant differences in subgroup analysis (all P>0.05, Table 2).
Statistically significant results.
TmLRP=thulium laser resection of the prostate; TURP=transurethral resection of the prostate; WMD=weighted mean difference; CI=confidence interval; Qmax=maximum flow rate; M-TURP=monopolar TURP; B-TURP=bipolar TURP; PVR=postvoiding residual; QoL=quality of life; IPSS=International Prostate Symptom Score.
PVR
Pooling data of seven studies 13,15 –20 showed that there were no differences between the two groups with regard to PVR (WMD: 0.33; 95% CI, −0.67–0.93; P=0.76) during the postoperative 1, 3, 6, and 12 months follow-up. TmLRP was comparable to both monopolar TURP (M-TURP) (WMD: 0.04; 95% CI, −1.18–1.25; P=0.95) and bipolar TURP (B-TURP) (WMD: 0.20; 95% CI, −0.87–1.26; P=0.72).
QoL
A significantly better improvement in QoL was observed in TURP compared with TmLRP (WMD: 0.08; 95% CI, 0.02–0.14; P=0.009) at 1-month follow-up, but there were no significant differences in later stages (all P>0.05, Table 2).
IPSS
TmLRP was associated with higher IPSS (WMD: −0.39; 95% CI, −0.75 to −0.04; P=0.03; Table 2) at 1 month; there were no significant differences at 3, 6, and 12 months follow-up (all P>0.05, Table 2).
Outcomes of perioperative variables
Operative time
In pooled data from the nine studies 12 –20 that reported operative time between TmLRP and TURP, TmLRP was associated with longer operative time (WMD 9.00 min; 95% CI, 2.53–19.47; P=0.006; Table 3). Six studies accessing TmLRP vs M-TURP (P=0.01) and four studies for TmLRP vs B-TURP (P=0.02) both supported the result.
Statistically significant results.
TmLRP=thulium laser resection of the prostate; TURP=transurethral resection of the prostate; WMD=weighted mean difference; CI=confidence interval; M-TURP=monopolar TURP; B-TURP=bipolar TURP.
Serum sodium and hemoglobin decreased
We extracted serum sodium decreased from four studies 13 –16 and serum hemoglobin decreased from six studies. 13 –18,20 There were statistically significant less serum sodium decreased (WMD: −3.58 mmol/L; 95% CI, −4.04 to −3.12; P<0.001; Table 3) and less serum hemoglobin decreased (WMD: −0.94 g/dL; 95% CI, −1.44 to −0.44; P<0.001; Table 3) in the TmLRP group compared with the TURP group. Four studies comparing TmLRP vs M-TURP also supported TmLRP (P<0.001), while only two studies reporting TmLRP vs B-TURP resulted in no significant difference.
Catheterization time and hospital stay
Eight studies 13 –20 including 900 patients on catheterization time and seven studies 12,13,15 –17,19,20 on hospital stay were reported, respectively, and the pooled data showed a significant difference favoring the TmLRP group associated with shorter catheterization time (WMD: −2.07 days; 95% CI, −2.66 to −1.49; P<0.001; Table 3) and shorter length of hospital stay (WMD: −1.87 days; 95% CI, −2.41 to −1.33; P<0.001; Table 3). There were significant differences in subgroup analysis.
Outcomes of complications
Overall complications
In pooled data from eight studies 12 –19 including 857 patients reporting on complications, there was a statistically significant reduction in the overall complications rate in the TmLRP group compared with the TURP group (OR: 0.29; 95% CI, 0.20–0.41; P<0.001; Table 4). Six studies 12 –17 accessing TmLRP vs M-TURP (P<0.001) and three studies 17 –19 for TmLRP vs B-TURP (P=0.001) both stood by the result, and it was especially reflected in systemic complications while the majority of local complications were nonsignificant.
Statistically significant results.
TmLRP=thulium laser resection of the prostate; TURP=transurethral resection of the prostate; OR, odds ratio; CI=confidence interval;
M-TURP=monopolar TURP; B-TURP=bipolar TURP; TUR=transurethral resection; UTI=urinary tract infection.
Systemic complications
Statistics on systemic complications showed that TmLRP identified as statistically significant a lower incidence of TUR syndrome (OR: 0.33; 95% CI, 0.12–0.89; P=0.03) and blood transfusion (OR: 0.28; 95% CI, 0.09–0.93; P=0.04).
Local complications
There were no differences between TmLRP and TURP with respect to recatheterization (OR: 0.89; 95% CI, 0.42–1.85; P=0.75), transitory urge incontinence (OR: 0.59; 95% CI, 0.31–1.12; P=0.10), stress incontinence (OR: 0.53; 95% CI, 0.07–4.12; P=0.55), UTI (OR: 0.57; 95% CI, 0.24–1.39; P=0.22), retrograde ejaculation (OR: 0.61; 95% CI, 0.35–1.05; P=0.08), but significant differences existed in urethral stricture (OR: 0.29; 95% CI, 0.12–0.71; P=0.007). Heterogeneity between studies was effectively decreased after this meticulous classification of all complications compared with the overall complications.
Discussion
TURP is an extremely effective method of treating patients with BPH and has been seen as the gold standard for decades. Major drawbacks of contemporary M-TURP, however, remain intraoperative and perioperative complications. B-TURP, a novel technical modification of M-TURP, in general was described as potentially permitting a longer resection time and providing an improved hemostasis, thus enabling the surgeon to resect larger prostates with less risk. 4 –6 In addition, the thulium laser, a new type of surgical laser, recently has been increasingly applied in urology and appears to solve many of the limitations of TURP with encouraging efficacy and safety. 24 In the present study, we applied an innovative view of regarding both standard TURP (M-TURP) and plasmakinetic TURP (B-TURP) as TURP and then compared the overall efficacy and safety with TmLRP. Our meta-analysis showed very good baseline characteristics with no significant differences regarding age, prostate volume, and preoperative micturition parameters including Qmax, PVR, QoL, and IPSS.
The present meta-analysis showed TmLRP had good functional results comparable to those of TURP on both subjective (IPSS, QoL) and objective (Qmax, PVR) variables. Although at the 1-month follow-up, the QoL and IPSS were slightly higher in the TmLRP group, reaching a statistically significant difference, the micturition parameters of both groups were equivalent at later follow-up. Our study confirmed that TmLRP was as effective as TURP in improving subjective symptoms and urodynamic measurements postoperatively. The problem is whether the patients would sustain these improvements in the distant future. Unfortunately, we fail to assess the long-term TmLRP curative effect 1 year later because of the lack of data. In fact, most of the minimally invasive treatment methods are proposed as substitutes for TURP.
The pooled operative time of TmLRP was significantly longer than that of TURP. Although in the experience of Xia and colleagues 13 and Wang and coworkers, 17 operative time of TmLRP was shorter compared with TURP, they could not find significant difference between them. These four studies 16,18 –20 demonstrated a statistically significant longer operative time. Despite the longer operative time, there was less serum sodium and hemoglobin decreased, which may indirectly reflect less blood loss and the lower transfusion rate in the TmLRP group than in the TURP group. Furthermore, as assessed by the better coagulation, it was also noted that the catheterization time among those in the TmLRP group was significantly shorter than among those in the TURP group, resulting in their shorter hospital stay.
This pooled analysis of the literature has also shown that TmLRP reduces the risk of overall complications, especially in blood transfusion, TUR syndrome, and urethral stricture. In fact, among the eligible studies included in the current meta-analysis, no patients in the TmLRP group needed blood transfusion, which can be explained by the superior coagulation for the reason that the thulium laser wavelength is excellent for controlling bleeding intraoperatively. It is reported that TURP has an increased risk of TUR syndrome, especially when treating patients with a larger prostate, 25,26 while TmLRP has less risk of TUR syndrome because physiologic saline was applied as the irrigation fluid. With regard to urethral stricture, seven articles we adopted showed there was a trend for lower incidence in TmLRP, which is another advantage of TmLRP. It may be attributed to the minimizing of thermal damage in reducing scar formation and stricture recurrence after laser incision. 9
We also performed a meta-analysis of many other side effects between the two groups, including recatheterization, transitory urge incontinence, stress incontinence, UTI, and retrograde ejaculation. The conclusion was that there was a slighter improvement of the above-mentioned adverse events, but they were not significantly different between the two groups. Larger-scale studies with longer regular follow-up are needed to confirm the reality of these promising outcomes about these side effects.
We should admit, however, that there existed certain inherent limitations in the studies included in our meta-analysis that cannot be ignored when interpreting our data. The major limitation of this study may be our innovative view of regarding both standard TURP (M-TURP) and plasmakinetic TURP (B-TURP) as TURP. The second limitation was the limited number of well-constructed prospective studies. Indeed, there was three RCT included in our analysis. In addition, all of the eligible studies were performed in China; thus, potentially selection bias may have an influence on the confidence of the results more or less.
Nevertheless, we applied a series of as many as available variables including demographic and clinical baseline characteristics, postoperative efficacy micturition parameters including Qmax, PVR, QoL, and IPSS, perioperative variables, and overall complications to compare TmLRP with TURP, strict criteria to evaluate the quality of the included studies, and subgroup analysis to minimize the effects of heterogeneity. We demonstrated the comparable efficacy and superior safety of performing TmLRP to that of TURP for treating patients with BPH.
Conclusions
Nine trials assessing TmLRP vs TURP were considered suitable for meta-analysis including three RCT, two prospective, and four retrospective studies. Although TmLRP was associated with longer operative time, patients undergoing TmLRP might benefit from significantly less serum sodium and hemoglobin decreased, shorter catheterization time, shorter length of hospital stay, and fewer overall complications, especially in blood transfusion, TUR syndrome, and urethral stricture. Moreover, the procedures demonstrate a comparable result in Qmax, IPSS, PVR, and QoL during the 1, 3, 6, and 12 months of postoperative follow-up. Our data suggest that as a promising minimally invasive technique, TmLRP appears to be a safe, feasible, and efficient alternative to TURP for treating patients with BPH with reliable perioperative safety, fewer complications, and comparable efficacy micturition parameters in relation to Qmax, PVR, QoL, and IPSS. Because of the inherent limitations of the included studies, further large sample prospective, multicentric, long-term follow-up studies and RCTs should be undertaken to confirm our findings.
Footnotes
Disclosure Statement
No competing financial interests exist.