
Abstract
Purpose:
To assess the safety and feasibility of laparoscopic donor nephrectomy with transvaginal extraction and impact of body mass index (BMI), menopausal status, previous surgery, and uterine fibroids.
Patients and Methods:
Five-port conventional laparoscopic donor nephrectomy with successful transvaginal extraction of the kidney was performed in 30 donors. The parameters assessed included age, BMI, operative time, estimated blood loss, warm ischemia time, postoperative pain score, preoperative and postoperative sexual function, wound complications, hospital stay, return to normal activities, recipient creatinine level, and other recipient-related complications. The data were compared with 30 female donors who had laparoscopic donor nephrectomy and transabdominal extraction.
Results:
The total number of patients who consented for the study was 38. In seven patients, an intraoperative decision to abort the transvaginal extraction was made because of obesity, pelvic adhesions, large uterine fibroids, and uterine artery injury. When compared with transabdominal extraction, there was no significant difference in warm ischemia time, mean operative time, estimated blood loss, hospital stay, recipient creatinine level, and complications. The mean pain score was significantly less on postoperative day 3 and day 4. There was also an earlier return to normal activities in the transvaginal group. There was no increase in infectious complication in both donors and recipient.
Conclusion:
Based on our initial experience with laparoscopic donor nephrectomy with transvaginal extraction, we recommend this procedure for a premenopausal donor, with a BMI <30. Our initial cases demonstrate that transvaginal extraction is feasible and safe for the donors.
Introduction
Development of natural orifice translumenal endoscopic surgery (NOTES) has generated enormous interest among surgeons in recent years. NOTES is defined as intentional puncture of one of the viscera to access the abdominal cavity and perform an intra-abdominal operation. 1 –3 Pure NOTES is in the process of evolution because devices currently available are suboptimal for performing advanced procedures such as nephrectomy. 4 Presently, surgeons overcome these inadequacies in instrumentation by performing hybrid NOTES. In hybrid NOTES, transabdominal laparoscopic trocars are placed to facilitate NOTES procedures, paving the way to a reduced number of ports. 5 –7
Of the various approaches used for NOTES nephrectomy, transvaginal NOTES is most preferred. 5 –7 It was in 2009 that the first living donor kidney extraction performed through this route occurred. 8 Living donor nephrectomy is more challenging, because the extraction is time sensitive and there is potential concern for infection to the recipient. 7
We present our initial experience of 30 cases of living donor nephrectomy performed with transvaginal extraction and its comparison with our last 30 female donors who had a transabdominal extraction.
Patients and Methods
Informed consent was obtained from the patient detailing the procedure. Patients with any active vaginal infection and who had not completed their family were excluded; all other women who consented for the procedure were included in the study. A vaginal swab culture was taken 2 weeks before surgery. A vaginal examination was performed using a speculum to detect any active infection and also to assess any anatomic abnormality of the vagina. Donors were advised to start use of a povidone iodine vaginal pessary 3 days before surgery. Preoperatively, 1 g of cefotaxime and 500 mg of metronidazole was administered intravenously, followed by another two doses at 8-hour intervals in the postoperative period. The patient was placed in a 45-degree left lateral position combined with lithotomy (Fig. 1). Thorough preparation of the abdomen and vagina was performed using povidone iodine, and a14F Foley catheter was placed.
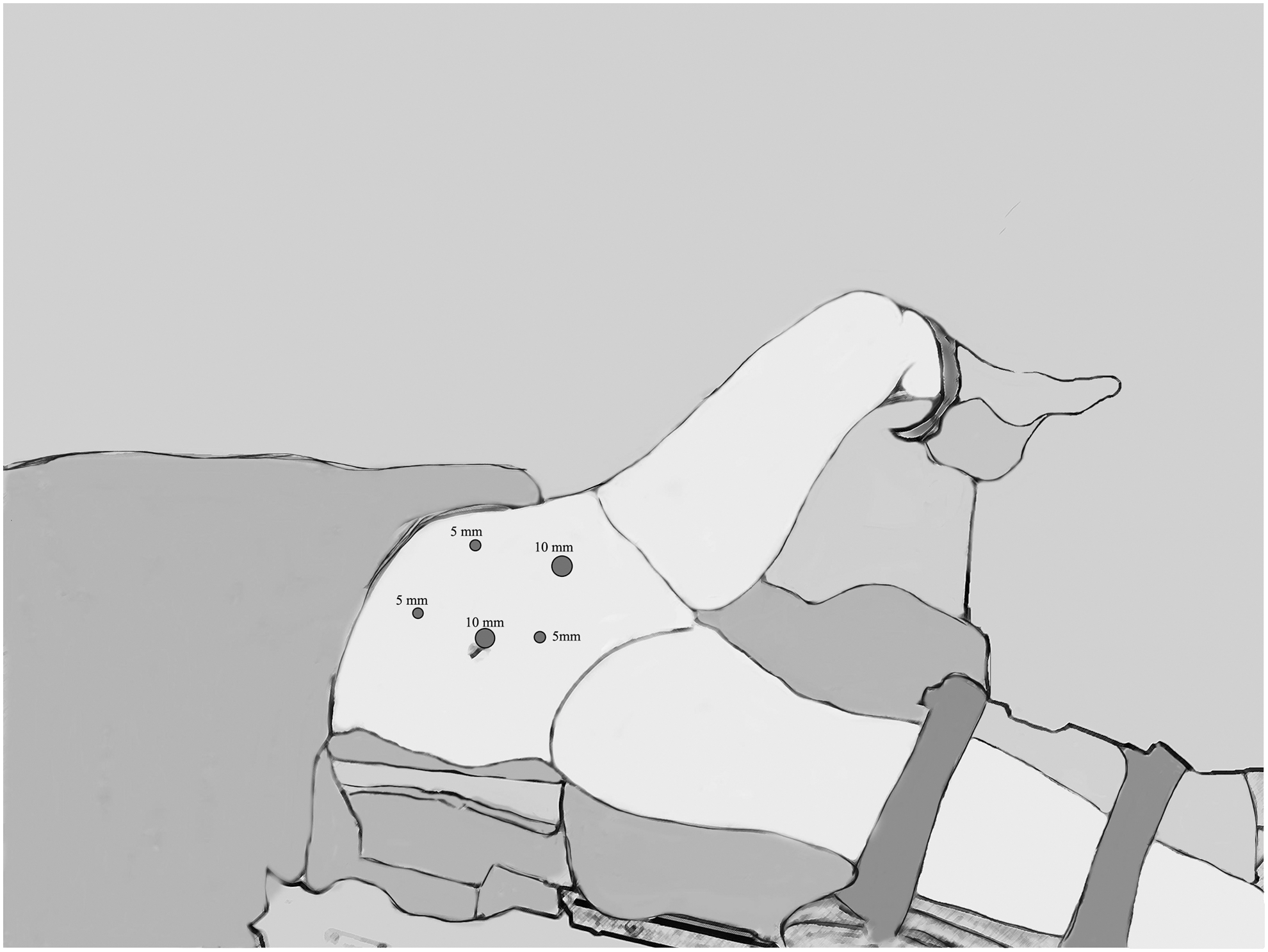
Modified lithotomy position and port placement.
Five ports are placed as shown in the Figure 1. The kidney was dissected free, and renal vessels were skeletonized. The table was then tilted to make the patient supine and in the Trendlenburg position to move the bowels away. The sigmoid colon was retracted using the 5-mm port in the lumbar region. An assistant used our modified CCL (colpo-celio chirurgie Lausanne) extractor, which makes the posterior fornix prominent. The modified CCL extractor is 15 cm long, has a bulbous tip with a diameter of 3.75 cm, and has a shaft of 12-mm diameter, which allows passage of the retrieval bag up to the renal fossa (Fig. 2).
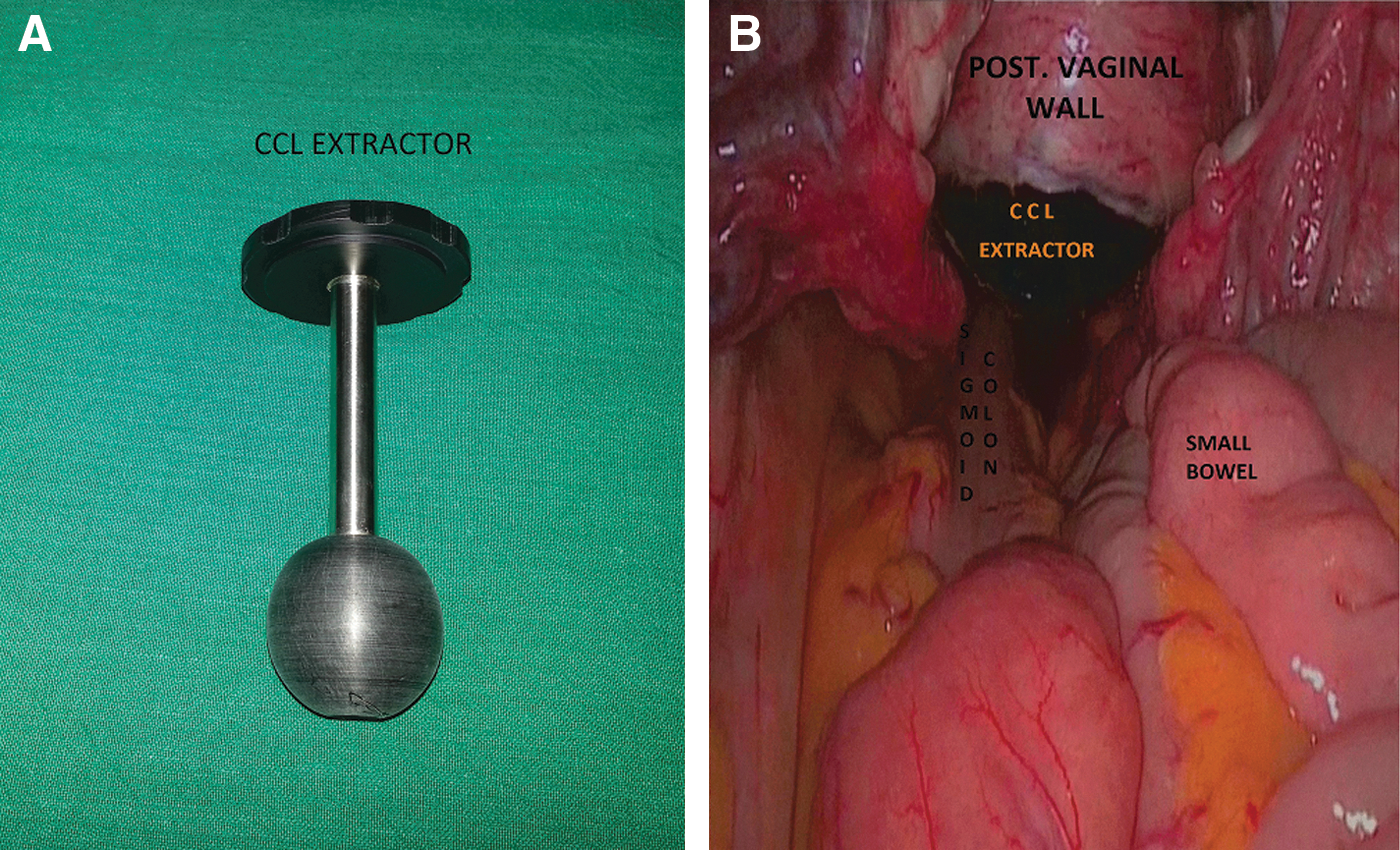
A 4-cm U-shaped incision was made on the vagina; the CCL extractor helped in the retention of pneumoperitoneum (Fig. 2). A retrieval bag (retrieval bag comfort, Aesculap, Tuttlingen, Germany) was then introduced through the CCL extractor by the assistant. The patient was tilted back to the lateral position with a slight upward tilt to prevent the bowel falling into the renal fossa. After the division of the ureter, renal artery and vein, the kidney was placed in the retrieval bag and extracted. The bag was cut open by the assistant and kidney delivered out by another sterile surgeon. The vagina was closed from below using interrupted 2.0 polyglycolic acid suture. A drain, vaginal pack, Foley catheter were placed and removed the next day. The patients received morphine on demand as an analgesic for the first day, followed by 1 g paracetamol orally at 8 hour intervals for the next 4 days.
Donors were followed up at 1, 3, and 6 months. The parameters assessed included age, body mass index (BMI), operative time, estimated blood loss, warm ischemia time, morphine consumption, postoperative pain score, wound complications, hospital stay, recipient creatinine level, and other recipient-related complications. All the recipients received 1 g cefipime and 500 mg metronidazole at 8-hour intervals for 5 days. The data obtained were compared with our previous 30 female donors who had transabdominal extraction. The transabdominal extraction was performed by a nonmuscle-cutting Pfannenstiel incision.
Return to normal activity was assessed by asking patients the following parameters: (1) Complete resolution of pain; (2) return to work and daily routine activities; (3) Point at which the patient felt the same energy level compared with the preoperative level. The earliest date with all three parameters satisfied was noted as return to normal activity. Sexual function was assessed by FSFI (Female Sexual Function Index) questionnaire preoperatively and 3 months postoperatively. 8 A surgical scar satisfaction score was measured after 3 months and rated from 1 to 10 with 1 being extremely displeased and 10 extremely pleased. The statistical analysis was performed by paired t test and chi-square test.
Results
The total number of female donors qualified for the study was 38. In seven donors, an intraoperative decision to abort vaginal extraction was made (Table 1). Two of these women had pelvic adhesions from previous surgery, two donors were obese with a BMI of 31 and 32, two women had large fibroids in the uterus that prevented obtaining adequate exposure to the vagina, and another patient had a uterine artery injury during the opening of the vagina. In one patient, a rent in the retrieval bag was noted after division of the pedicle; in this instance, a port site incision was extended to deliver the kidney. The warm ischemia for this particular case was 5 minutes.
Comparison Between Donors Who Had Transvaginal and Transabdominal Extraction
Complication grade according to Clavien–Dindo classification.
Measured by CKD EPI Index (Chronic Kidney Disease Epidemiology Collaboration). 23
BMI=body mass index; eGFR=estimated glomerular filtration rate.
When compared with transabdominal extraction, there was no significant difference in warm ischemia time, mean operative time, estimated blood loss, morphine consumption, and hospital stay. The mean pain score was significantly less in the transvaginal group by postoperative day 3 and day 4. There was also an earlier return to normal activities in the transvaginal group. There was no significant difference in mean recipient creatinine level and other recipient complications. There was a significant difference in surgical scar satisfaction score when comparing the two groups. Two of three postmenopausal patients sustained a small vaginal tear, which was repaired. Only 18 of the 30 patients were sexually active in the transvaginal group and 17 in the transabdominal group. The mean FSFI score before and after surgery was 24.3 (17–33), 23.5 (15–35) in the transvaginal group, and no significant difference was noted (P=0.77). The two patients who sustained vaginal tear were not sexually active and continued to be so 3 months after the surgery. There was no incidence of prolonged ileus in both groups, and all the patients resumed oral intake the first postoperative day.
We had one case of wound infection in the recipient in the transvaginal group in whom the culture grew Staphylococcus aureus. There was a case of biopsy-proven hyperacute rejection in a patient undergoing a second transplant. Another patient had acute tubular necrosis with delayed graft function necessitating dialysis; warm ischemia time in this case was 4 minutes. In this instance, the renal function recovered after 27 days, and the patient had a creatinine level of 1.5 mg% at 3 months. One patient had an acute pulmonary embolism and died on the 20th postoperative day; the graft function was normal in this patient. One patient in the transabdominal group died from sepsis 80 days post-transplant.
Discussion
The first NOTES series was reported in 2004 by Kalloo and associates. 1 The proposed advantages of NOTES included lack of skin incisions, decreased postoperative pain, and diminished risks of postoperative hernias. 5 Ever since NOTES emerged as an alternative platform for minimally invasive surgery, several routes, including transvaginal, transgastric, transrectal, and transcystic, have been proposed. Among these, the transvaginal approach has gained maximum popularity. 5
Transvaginal access to the abdominal cavity, or culdoscopy, was first performed by Decker in 1928. 10 The vagina has also been used to retrieve organs after laparoscopic dissection. 11 –13 Studies have demonstrated reduced pain after transvaginal hysterectomy compared with open hysterectomy. The potential complications of transvaginal extraction include infection (3.9%), rectal injury (0.2%), and dyspareunia (0.2%). 14,15 The expansile nature of the vagina allows larger specimens to be extracted with ease and manipulation of the rigid instruments. 16
Breda and associates 17 was the first to perform transvaginal extraction of a nonfunctioning kidney in 1993. Gill and colleagues 5 had published a series of 10 cases in which transvaginal extraction of the specimen was performed in 2002. Subsequently, Branco and coworkers 6 performed the first transvaginal hybrid notes in a case of nonfunctioning kidney in 2007. Alcazar and colleagues 4 published an initial series of NOTES-assisted radical nephrectomy in patients with renal cancer. He and his associates have also performed pioneering work in the arena of hybrid NOTES donor nephrectomy and published their initial series of 20 cases in 2011. 7 Very recently Kaouk and coworkers 18 have published a case of hybrid laparoendoscopic single site donor nephrectomy with a single periumbilical incision.
Although there are few isolated case reports of donor nephrectomy with transvaginal extraction, none of these centers has come up with larger numbers. 19 To our knowledge, this is the largest series so far published. There are some salient differences between our technique and that used by Alcaraz and colleagues. 7 We use a modified CCL extractor in the posterior fornix that makes the posterior vaginal prominent; an incision of about 4 cm made on the vagina facilitated the retrieval of the kidney. This has enabled us to reduce the warm ischemia time to 2.5 minutes. Alcaraz and colleagues digitally tear the vagina while extracting; the time consumed may explain the higher mean warm ischemia time of 4.5 minutes in their series. 7 We use an extra 5-mm port in the sub-umbilical region for incising the vagina; this port, in turn, helps in retraction of the colon at the time of extraction.
In our series, we found that that women who had transvaginal extraction had less pain on postoperative day 3 and day 4 and had earlier return to normal activities. Similar findings were noted by Canes and coworkers 20 in their series of 18 donors who underwent single-site donor nephrectomy. In obese patients, it was difficult to obtain adequate exposure to the vagina, which could be attributed to the reduced intra-abdominal space, excess intra-abdominal fat, poor maneuverability of instruments, and inability to retract the colon well. There was also difficulty in placing the patient in the combined lithotomy lateral position, and also there was an increase in airway pressure noted while placing the patient in a steep Trendlenburg position.
In donors with previous surgery, an intraoperative decision can be made after assessing the extent of adhesions. The vaginal extraction would be an added advantage in these patients because it helps to avoid incision over the previous scar. In patients with previous abdominal hysterectomy, we encountered adhesions and altered anatomy that made the surgery more difficult. Patients with large fibroids in the uterus may also pose a challenge in certain cases, because this would preclude access to the posterior fornix.
We had problems in three of our postmenopausal patients while extracting, with two patients sustaining a small vaginal tear and the retrieval bag gave away in another case. We observed that in premenopausal women, an elastic vagina allows smooth passage of the specimen, while in postmenopausal women, digital tearing of the vagina is needed. On the basis of our current findings, our future preference would be to exclude postmenopausal patients.
We did not observe any impact on sexual function, although large numbers of patients in our group were not sexually active. Complications such as low backache or neuropathy, related to the positioning of the patient, were also not experienced. There was no increased incidence of any infectious complication in both donors and recipients. Our antibiotic policy of administering metronidazole was based on previous studies that found a reduced infection rate. 21,22 We found that donors who had transvaginal extraction had a higher surgical scar satisfaction score when compared with those who had transabdominal extraction.
The mortality rate in recipients is slightly higher in our series; this could be attributed to the higher risk cases we encounter in our center. Our donors tend to stay longer in the hospital because of inexpensive inpatient care, cultural reasons, and inadequate access to convenient transportation. Lack of randomization, absence of long-term follow-up, and inability to implement a validated questionnaire for early return of normal activity are other limitations of our study.
Conclusion
Transvaginal extraction after laparoscopic donor nephrectomy is associated with reduced pain and early return to normal activity. We recommend this procedure for a premenopausal donor, with a BMI <30. In patients with a history of pelvic surgery and large uterine fibroids, the decision of extraction can be offered after intraoperative assessment. Our initial cases demonstrate that transvaginal extraction is feasible and safe for the donors.
Footnotes
Disclosure Statement
No competing financial interests exist.