
Abstract
Background and Purpose:
The transvaginal approach for the repair of vesicovaginal fistula (VVF) can sometimes be challenging, especially in fistulas located near the vaginal cuff. We describe a simple technique for the vaginal repair of VVF with the use of endoscopic optics.
Patients and Methods:
Three women were admitted to our department with urinary incontinence after total hysterectomy. Assessment with a clinical examination, imaging, and cystoscopy confirmed the diagnosis of VVF. All patients were operated on between December 2012 and January 2013. The operations were conducted under spinal anesthesia with the patients in the lithotomy position. Cystoscopy was performed and retrograde pyelography ruled out any ureteral damage or fistula. A 10F to 12F Foley catheter was inserted into the fistula. From this point, the operation proceeded with optic vision, mimicking laparoscopic dissection and suturing techniques using a standard 5 mm, 30-degree optic lens, a surgical monitor, and open surgical instruments. The fistula was circumferentially incised and widely mobilized from the surrounding tissues and closed without tension in two layers. A urethral Foley catheter was inserted and maintained for 14 days.
Results:
The mean operative time was 70 (range 60–80) minutes. Estimated blood loss was minimal. All patients were discharged at postoperative day 1. No complications were observed. At the postoperative first and third month follow-up visits, all patients were voiding without any urinary leakage or complaints.
Conclusions:
The use of optics in the vaginal repair of VVF is a useful technique. Optic guidance facilitates surgical vision, dissection, and hemostasis. It is also excellent for surgeon comfort, ergonomics, and resident training.
Introduction
V
Although many surgical attempts have been made to correct VVF over the centuries, successful repair of fistulas was not documented until James Marion Sims, who used a transvaginal technique to perform the repair, including the use of silver wire suture. 5 Most of the principles he described are still used in daily practice. Subsequent modifications and later advances included the vaginal flap-splitting technique by Mackenrodt and the interposed graft harvested from labial fat by Martius. In 1890, the suprapubic transvesical route was described by Trendelenburg, and in 1893, Von Dittel gained transperitoneal exposure for the first time. 4,6
Small VVF may close spontaneously by simple draining with a catheter. Also, minimally invasive options including cautery or laser fulguration of the fistula tract have been reported with remarkable results. 1,4,7 In cases of a larger or complex VVF or if there is a radiation-induced fistula, surgical correction is indicated. Various surgical techniques have been described for VVF repair, depending on the location, severity, and the cause of the fistula and the surgeon's experience. Two main approaches include transvaginal and transabdominal routes, and the latter has further options such as transperitoneal, extraperitoneal, laparoscopic, and robotic surgery. Because many urologists are relatively unfamiliar with vaginal cuff anatomy, the transvaginal approach can sometimes be challenging. Moreover, exposing high or retracted fistulas usually located near the vaginal cuff can be difficult, especially in deep and narrow vaginas. 1,8 To overcome these issues, we describe a simple technique with the use of endoscopic optics with which most urologists are familiar.
Patients and Methods
Three women with constant urinary drainage per vagina after total abdominal hysterectomy were admitted to our department after referral from secondary care centers where they received a diagnosis of VVF. All patients were consecutive cases who were operated on between December 2012 and January 2013. Assessment with a clinical examination, imaging (CT cystography and MRI), and cystoscopy confirmed the diagnosis of VVF.
Surgical technique
The operations were performed under spinal anesthesia with the patients in the standard lithotomy position. Basic setup and the instruments are listed in Table 1. The surgeon sat in front of the patient and the first assistant (camera holder) sat at the right of the surgeon holding the camera with the left hand, resting the elbow on his/her abdomen or groin to stabilize the camera when needed. The second assistant stood at the right of the patient just behind the right leg, caring not to bend toward the leg to prevent any injury.
After sterilization and draping, a weighted retractor and a Lone Star retractor were placed at the vaginal introitus to optimize vaginal exposure. Cystoscopy was performed, and ureteral catheterization and retrograde pyelography ruled out any ureteral damage or fistula. A hydrophilic guidewire was negotiated through the VVF tract with the aid of a ureteral catheter, and a 10F to 12F Foley catheter was inserted through the fistula over the guidewire using an intracath (Fig. 1).
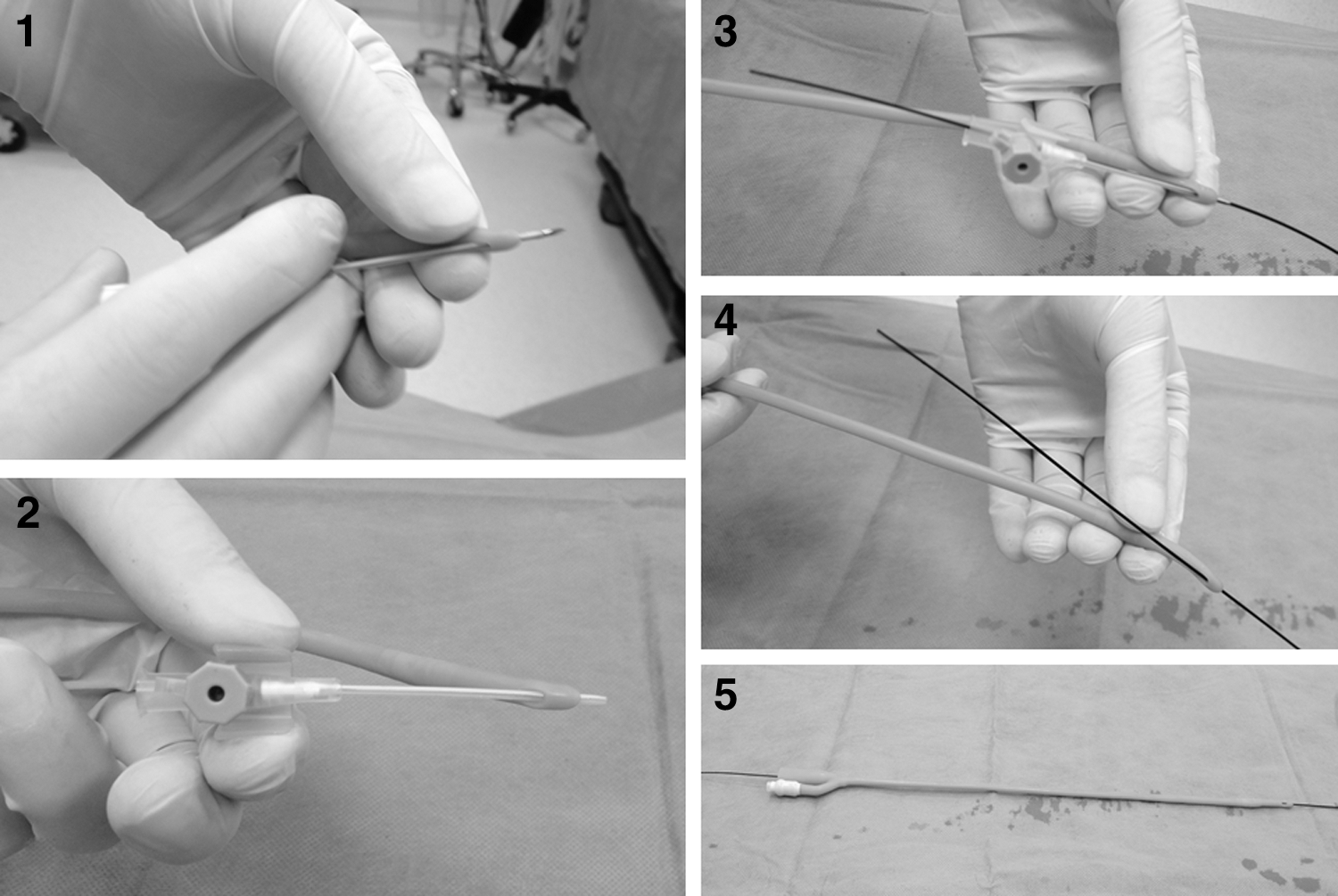
Step-by-step insertion of a 12F Foley catheter over the guidewire using an intracath,
From this point, the operation proceeded with optic vision, mimicking laparoscopic dissection and suturing techniques using a standard 5 mm, 30-degree optic lens, a surgical monitor, and open surgical instruments (Fig. 2). Two to three stay sutures were placed on the vaginal wall around the fistula for traction. The fistula was circumferentially incised and widely mobilized from the surrounding tissues and closed without tension in two layers (bladder, 3-0 interrupted monofilament absorbable, vertical; vaginal wall, 2-0 interrupted monofilament absorbable, horizontal). After closure of the first layer, the presence of any leakage was evaluated by filling the bladder with 200 mL of saline. The fistula tracts were not excised except the second case, which had a septum in the middle of the fistula tract that resembled two adjacent fistulas (Fig. 3). A urethral Foley catheter was inserted and maintained for 14 days. At the end of the operation, the vagina was packed with gauze soaked with povidone iodine that was removed on the postoperative first day. A supplementary video demonstrating this technique is available at
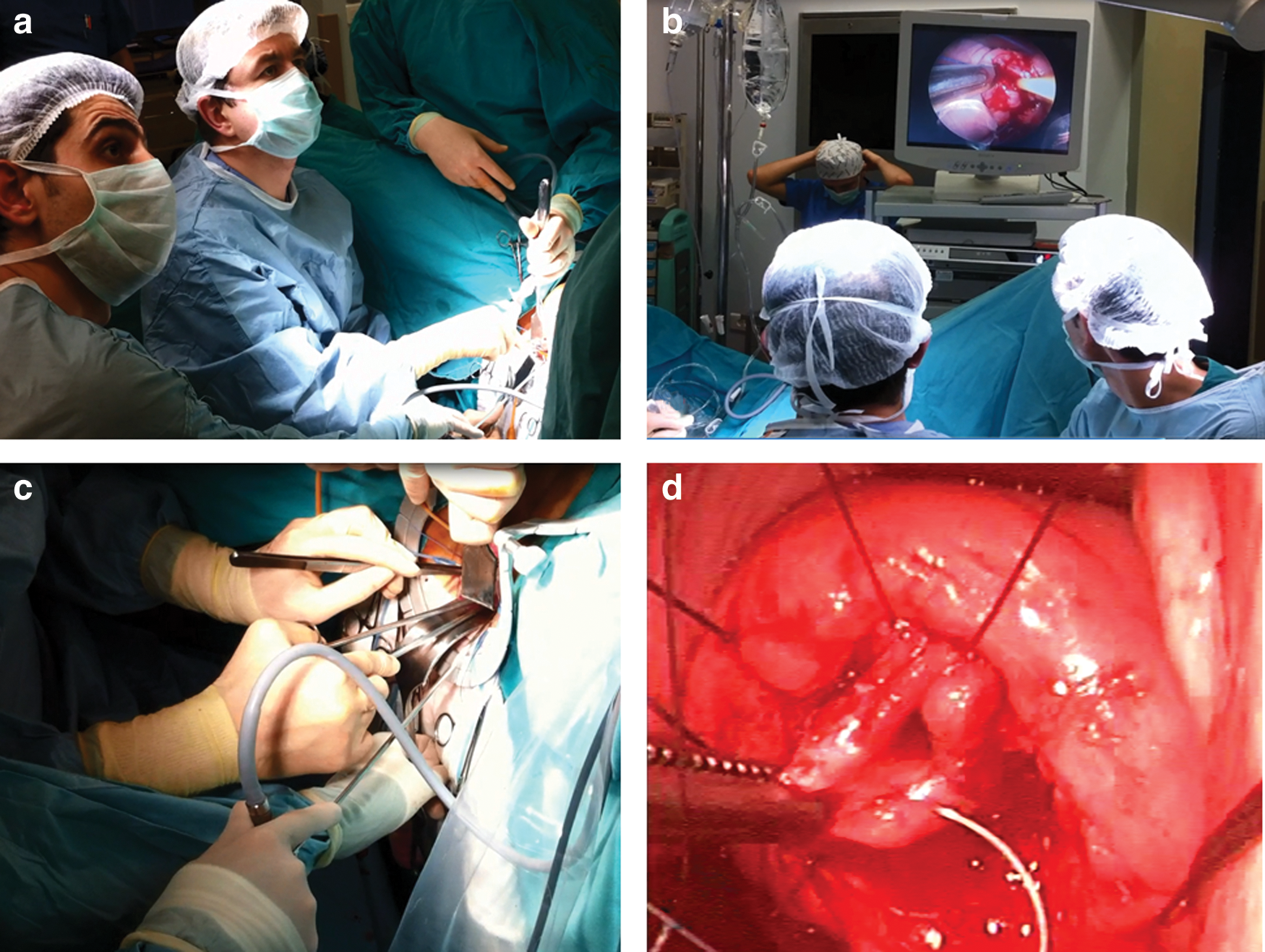
External view of the operation with surgeon and assistant using the surgical monitor
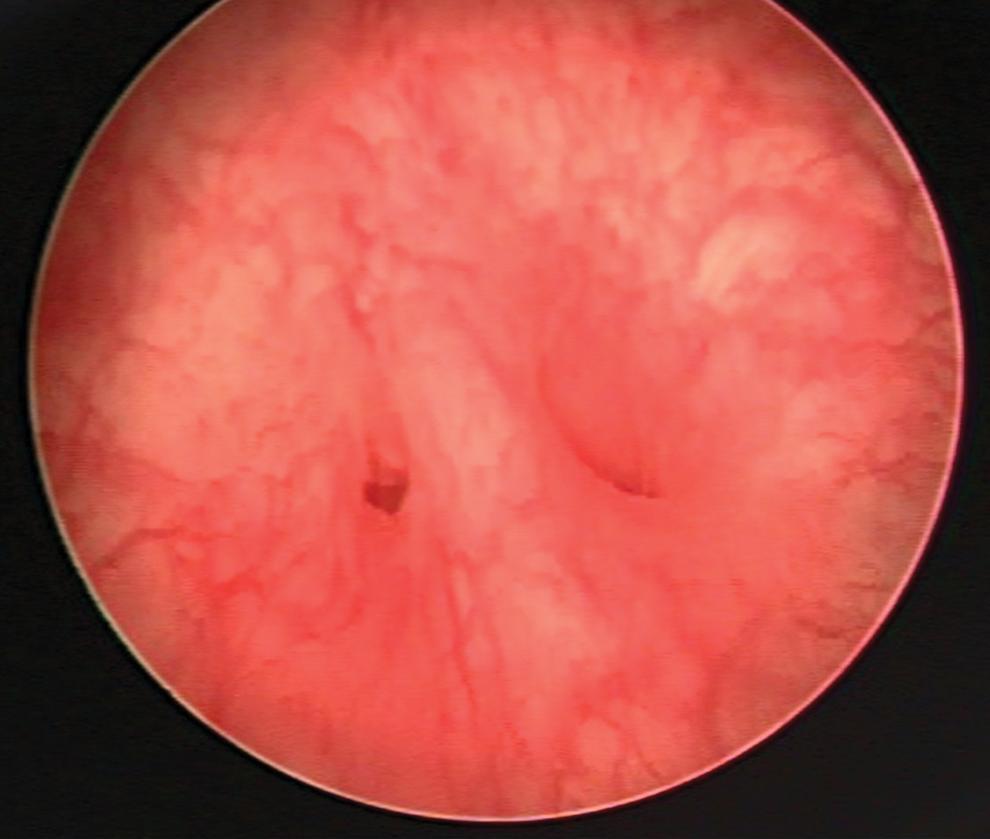
Cystoscopic view of the fistula in the second case, which had a septum in the middle of the fistula tract that resembled two adjacent fistulas.
All patients were prescribed antibiotics for 1 week postoperatively. Anticholinergics were used to decrease bladder contractions. Sexual intercourse was prohibited for 1 month after removal of the indwelling catheter.
Results
The characteristics, history, and surgical data of the patients are summarized in Table 2. The mean operative time was 70 (range 60–80) minutes. Estimated blood loss was minimal for all of the patients. Narcotic analgesics were not needed, and postoperative pain was controlled with diclofenac sodium. All patients were discharged from the hospital on the postoperative first day. No minor or major complications were observed. At postoperative first and third month follow-up visits, all patients were voiding without any urinary leakage or complaints.
VVF=vesicovaginal fistula.
Discussion
For centuries, VVF has been a challenge for surgeons and a significant health problem for patients, especially when surgical repair is not successful or severe complications occur. 9 In the industrialized world, the main cause of VVF is usually an iatrogenic injury during gynecologic surgery, most commonly abdominal hysterectomy.
Although conservative and minimally invasive treatment options such as catheter drainage and fulguration with cautery or laser have been described, surgery remains the main treatment for VVF. VVF may be repaired through a transvaginal or a transabdominal (transvesical) approach (O'Conor technique). 10 Each approach has advantages and disadvantages, depending on the particular features of the fistula, and excellent outcomes have been reported with both approaches. Many factors such as size and location of the VVF and the need for any additional procedures influence the choice of approach; however, the most important factor remains the experience of the surgeon in either approach. Therefore a single approach cannot be suggested for all fistulas, and the optimal approach is usually the one that is most successful in the individual surgeon's hands. 1 The success rate reported for a simple VVF repair in current practice, whether through a vaginal or an abdominal approach, is more than 90%.
The majority of VVF can be repaired by the transvaginal route. 1,11,12 The relative advantages of a transvaginal approach are shorter operative time and hospital stay, minimal blood loss and postoperative pain, absence of the need for opening the bladder, possibility of performing anti-incontinence procedures, and availability of local interpositional flaps, when compared with an abdominal approach. 1,12 In addition, the transvaginal approach offers direct access to the fistula without entering the abdomen and is less invasive. There have been several published studies favoring the transvaginal approach for both obstetric and gynecologic fistulae. 12 –15 Although there are a limited number of patients in our study, mean operative time is 70 minutes, mean hospital stay is less than 24 hours, and the operations were completed with minimal bleeding. In addition, none of our patients needed additional analgesics other than nonsteroidal anti-inflammatory agents. These results are comparable to those of previous studies concerning vaginal repair of VVF.
There are also some potential disadvantages to the vaginal approach that include the relative lack of familiarity with the vaginal anatomy of many urologists, the possibility of vaginal shortening, and the difficulty in exposure when there is a high or retracted fistula located close to the vaginal cuff, especially in deep and narrow vaginas. 1,12 The position used during fistula surgery depends on the location and the severity of the fistula to be repaired. A high lithotomy position with the buttocks pulled well over the edge of the operating table (in steep Trendelenburg position) provides excellent exposure for the vast majority of fistulas. 16 The transvaginal approach is not an appropriate choice for patients in whom a high-lithotomy position cannot be achieved because of musculoskeletal diseases or abnormalities.
To overcome most of these disadvantages, alternative methods have been preferred. One of these was alternative positions such as prone (knee-chest) position, which was better for the operating surgeon ergonomically, because the fistula is placed in front of the surgeon even in the case of a high supratrigonal fistula; however, it is uncomfortable for the patient and generally necessitates intubation. 16 Alternatively, operating by the abdominal route increases the cost and time of the operation, but is still often performed for some high fistulas where surgical access is problematic. Another disadvantage of the abdominal route over vaginal repair is the significantly higher need for blood transfusion. Chigbu et al. concluded that the route of repair of juxtacervical VVF should be determined by accessibility of the fistula and the vaginal route should be preferred whenever possible. 17
Our technique of optic guidance in addition to vaginal surgery overcomes most of the disadvantages of the transvaginal approach. Using our technique, there is no need for an extended lithotomy position, and even the patients with orthopedic obstacles can be operated on if a simple lithotomy position can be provided. During vaginal repair, usually a gentle traction is placed on the Foley catheter to bring the fistula into view, and long instruments are used for dissection if the fistula is located high in the supratrigonal area. Optic guidance also facilitates surgical exposure and provides an excellent view for the surgeon.
There is debate as to whether or not a Martius flap or other graft should be used in fistula repair. 16 In a retrospective analysis, Browning 18 evaluated 400 patients in whom comparable fistulas were repaired with and without the use of a flap. No differences were shown between the two groups in closure rates or postoperative incontinence rates. We repaired the fistula with two layers of nonoverlapping interrupted sutures without mobilizing any additional tissues such as a Martius flap or a peritoneal flap. Many experienced fistula surgeons now only use grafts under rare circumstances, such as when the urethra has been reconstructed, when the tissues are particularly poor, or if there have been multiple previous attempts at repair. 16
The use of endoscopic optics in fistula surgery has been previously described and used as a diagnostic tool to confirm the findings in physical examination 12,19 ; however, it has not been used during vaginal surgery. Optic guidance has most of the advantages of laparoscopic surgery while it excludes most of the disadvantages. The most useful advantage is the magnification of the surgical field leading the surgeon to make a more delicate dissection. Another advantage is to provide an ergonomic posture for the surgeon without bending to see the surgical field optimally. We also recommend this technique for the education of residents in training centers, because it is always difficult for the residents and assisting staff to see the surgical field in vaginal surgery, especially in deep and narrow vaginas.
There are also limitations to this study. Mainly, the study group included a limited number of patients; however, our aim was to describe a surgical technique with its preliminary results rather than reporting the outcomes in a series of patients. The follow-up period in our study is relatively short; however, recurrent fistulas were reported to develop within the first 3 months after primary repair. 20 All of the patients in this study have a follow-up of more than 3 months, so they were considered as cured. While using our technique, challenges can be experienced. In the beginning, instrument overlapping may cause some difficulty, and dissection and suturing may be challenging if the surgeon is inexperienced with a two-dimensional view. Effectively using the 30-degree lens by keeping it close to the lateral vaginal wall prevents overlapping of the instruments with the lens and also provides a better surgical view.
Conclusions
The use of optics in vaginal repair of VVF is a useful technique. Optic guidance facilitates surgical vision, dissection, and hemostasis. It is also excellent for surgeon comfort, ergonomics, and resident training. With the help of an old friend, the endoscopic optics, urologists can adopt transvaginal repair of VVF quite easily. The embracement and widespread use of our technique may provide more reliable outcomes in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.