
Abstract
Introduction
L
However, with growing expertise in LPN overtime, there is a resultant improvement in perioperative outcome measures, while preserving renal function and oncologic outcomes compared to an open surgical approach. 3 In addition, complex renal tumors, including hilar tumors have been managed successfully with LPN. Several retrospective case series have reported its feasibility and demonstrated comparable oncologic outcomes of LPN for hilar tumors. 4 –6 Furthermore, reduction in warm ischemia time (WIT) or its elimination thereof (off-clamp) has been associated with improved functional outcomes after LPN. 7
However, off-clamp LPN can be challenging when operating on hilar tumors. By virtue of their juxtaposition to the renal artery, vein, or pelvis, LPN for renal hilar tumors can be particularly challenging due to concern for bleeding, prolonged WIT, and potentially poor outcomes when compared with the open surgical approach. In this case series, we report the feasibility and efficacy of off-clamp LPN for hilar tumors by evaluating perioperative factors, oncologic, and renal functional outcomes.
Methods
A retrospective review of nine patients undergoing off-clamp LPN for hilar masses was performed from November 2006 to February 2010. The study was reviewed and approved by the Institutional Review Board (IRB). Hilar tumors were defined as renal cortical masses in direct physical contact with the renal artery, vein, or both as identified on preoperative imaging and confirmed based on intraoperative findings at the time of LPN (Fig. 1). A review of the preoperative imaging was used to obtain tumor characteristics, including size, volume, and tumor complexity based on R.E.N.A.L. nephrometry scores as proposed by Kutikov et al. 8
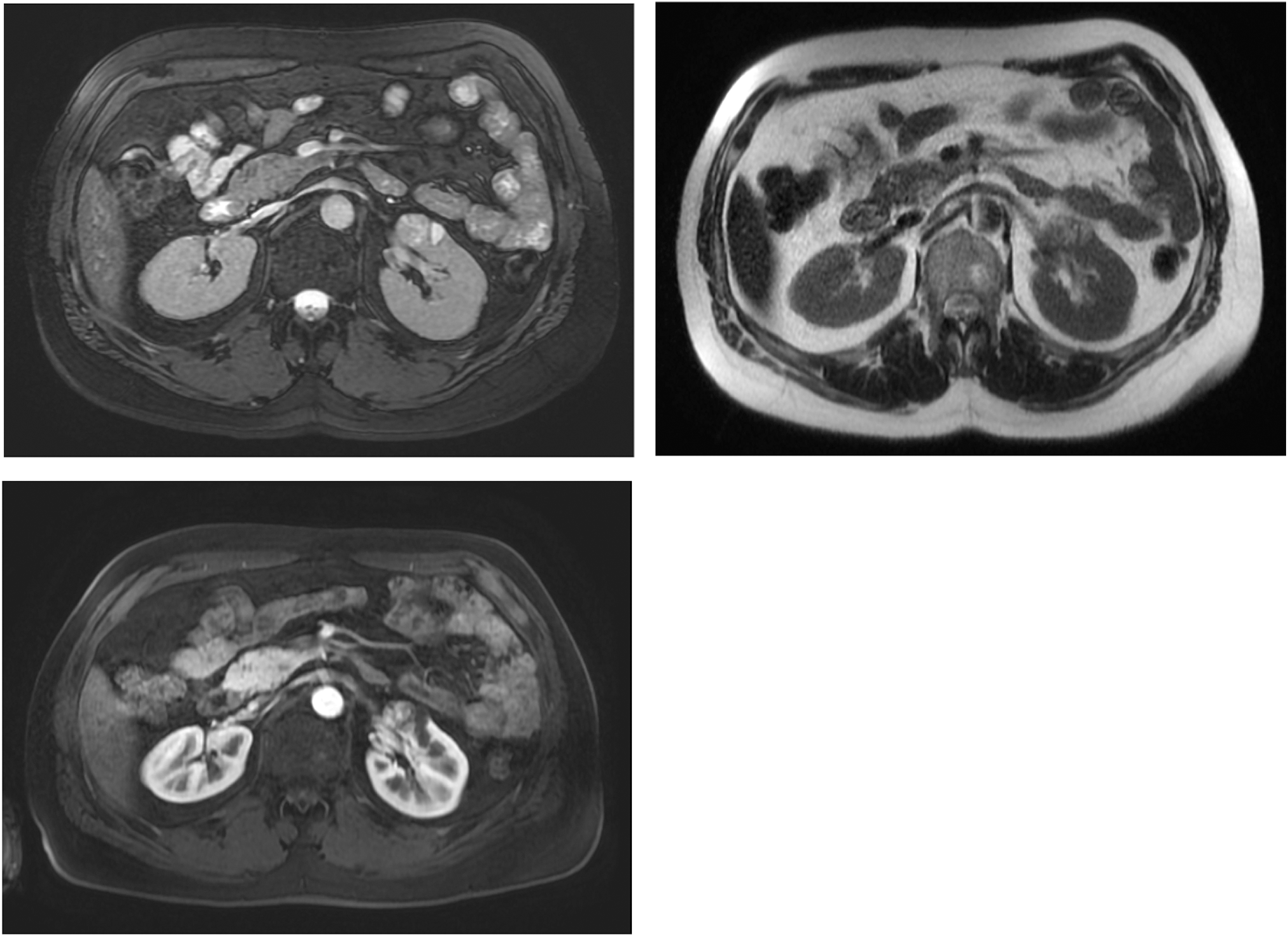
Fifty-three-year-old male with a 3.4×2.5×2.4 cm renal mass arising from the anterior hilar lip of the midportion of the left kidney with no MR evidence of vascular or lymph node extension.
Patient's medical charts were reviewed to collect preoperative parameters, including gender, age, body mass index (BMI), American Society of Anesthesiologists physical classification (ASA) score, and creatinine. Intraoperative data, including duration of surgery or operative time (ORT), estimated blood loss (EBL), and conversion to open surgery/radical nephrectomy, were collected. Postoperatively, clinicopathologic data were collected, including the length of stay, need for transfusion, complications classified by the Clavien-Dindo grading system, 9 tumor margin status, and tumor histology. Patients were evaluated for recurrence based on clinical evidence and the findings on the most recent renal imaging study (renal ultrasound, computed tomography scans, and/or magnetic resonance imaging scans). The postoperative estimated glomerular filtration rate (eGFR) was estimated using the MDRD formula. 10,11
There were no specific clinical features identified as absolute contraindications to LPN for hilar masses and the decision to perform off-clamp surgery was made during the procedure by a combination of imaging and intraoperative findings; vascular invasion was considered a contraindication. Transperitoneal LPN was completed using a standard three-port technique. After a pneumoperitoneum of 15 mm Hg was induced, complete exposure of the renal artery and vein was performed to allow for the application of laparoscopic bulldog clamps, if needed, to control bleeding. Before renal tumor extirpation, intraoperative ultrasound was employed to delineate the tumor margins and proximity to hilar structures. Cold and sharp excision of the tumor with laparoscopic scissors and blunt dissection with the suction device were employed to excise or enucleate the mass. During excision, hemostasis was achieved with titanium clips applied on visualized vessels feeding the tumor and argon beam coagulation of the operative bed after biopsy of the tumor base was completed. Observed violation of the urinary collecting system was repaired using vicryl sutures. Intraoperative margin status was determined by obtaining a tissue biopsy of renal parenchyma from the base of the operative bed at the completion of the excision. Secure renorrhaphy was performed with pledgeted 2-0 vicryl sutures. 12
Statistical analysis was done using SAS® for Windows® version 9.3, with continuous variables reported as mean/median range and categorical variables reported as frequencies/percentages.
Results
A total of nine patients with hilar tumors who underwent LPN off-clamp were identified (Table 1). The mean age was 60.5 years (range: 42.6–78.3 years). Sixty-seven percent of these patients were males. The mean ASA score was 2. The mean BMI was 27.7 kg/m2 (range: 22.9–38.4). Mean preoperative eGFR was 97.2 mL/minute.
ASA=American Society of Anesthesiologists physical classification; BMI=body mass index; GFR=glomerular filtration rate.
The duration of surgery ranged from a minimum of 35 minutes to 3 hours 30 minutes with a mean of 1 hour. Although the mean in-hospital stay was 6 days (range: 1–29 days), the majority of patients remained for 2 days or less, with one patient staying for 29 days on account of bladder rupture requiring reoperation. There were no conversions to open surgery, although one case was converted to radical nephrectomy due to inability to adequately dissect the mass from the abutting renal vessels. The median duration of follow up for oncologic and renal functional outcomes was 42.8 months (range: 1.0 to 76.4 months) and 32 months (range: 12 to 72 months), respectively.
With respect to tumor characteristics (Table 2), the mean tumor size and volume were 3.2 cm and 35.8 cm3, respectively. The tumors were evenly divided by location with 56% being endophytic and 44% being exophytic, respectively. The collecting system was involved in three (33%) patients. Using the R.E.N.A.L. nephrometry scoring system, a greater majority (75%) of these tumors were classified as being of intermediate complexity. However, no comparisons were made between groups given the small sample size. On final pathology review, the majority of all lesions were renal cell carcinoma (RCC) of clear histology (78%). Other classified tumor histologies included papillary RCC (11%) and a benign mass demonstrating chronic and granulomatous inflammation (11%).
Information was incomplete for one patient who revealed inflammation on final pathology.
RCC=renal cell carcinoma.
Three patients had complications: one early complication and two late complications. The early complication was Clavien grade II; urinary retention and febrile UTI after discharge from the hospital requiring bladder catheter drainage and antibiotic therapy. The delayed/late complications: one was Clavien grade II; superficial postoperative wound infection at a trocar site that was managed with antibiotic therapy. One major complication (Clavien 5) was noted. The patient had significant preoperative hepatic impairment (Child-Pugh class B) with a protracted postoperative course, including significant hematuria secondary to coagulopathy, bladder rupture, and ultimately, multisystem organ failure and death resulting from withdrawal of care.
There was no change in the estimated GFR at a median follow-up of 32 months (97.2 mL/minute vs 71.3 mL/minute; p=0.052). With respect to the oncologic outcome, no patient had any evidence of recurrence clinically or radiographically with a median follow-up of 42.8 months (range: 1.0–76.4).
Discussion
Although partial nephrectomy for T1 disease is becoming increasingly utilized, a good proportion of patients continue to undergo nephrectomy for lesions amenable to nephron-sparing surgery. 13 A major goal in performing partial nephrectomy (laparoscopic or open) is nephron preservation and, consequently, conservation of renal function. Hence, various techniques have been reported to improve outcomes related to the effect of WIT, including zero-ischemia and off-clamp LPN. 14 Off-clamp LPN can be technically challenging given the close proximity of the hilar vessels and renal pelvis with concern for excessive blood loss, and thus, the need for blood transfusion, collecting system injury, high rate of conversion to open or total/radical nephrectomy, prolonged ORTs, or length of hospital stay. In a retrospective review of 257 operations planned for LPN, Rais-Bahrami et al. reported conversion rate to LRN of 13.6% and to open surgery of 1.6% with age, tumor size, operating time, and hypertension as factors predictive of conversion. 15 In our current series, there was no conversion to open surgery and one case was converted to LRN because of difficulty dissecting the mass off the renal vessels. In the hands of an experienced minimally invasive surgeon, partial nephrectomy for complex hilar lesions can be approached laparoscopically completely avoiding warm ischemia without compromising intraoperative parameters, including EBL, operation time, or transfusion requirement (Table 3).
Renal functional outcomes
In any technical approach to partial nephrectomy, it is vital to assess the preservation of renal function. In a series of 18 patients with hilar tumors (mean size=3 cm), Lattouf et al. showed a reduction of almost 12% on follow-up mercaptoacetyltriglycine-3 scans in patients after a median follow-up of 26 months. 16 It is reasonable to expect that total elimination of WIT will result in improved functional outcomes. In our series, we found that at a median follow-up of 3 years (range 1–6 years), there was no significant difference between the absolute serum creatinine and eGFR of patients compared with their baseline or preoperative values. However, experience is required to be able to perform LPN for hilar tumors off-clamp. 17
Oncologic outcomes
Whereas preservation of renal function is important, even more vital is attaining a durable oncologic outcome. In this series, the oncologic outcome was assessed by the margin-positive rate and clinical/radiographic evidence of tumor recurrence during follow up. Given the close proximity of hilar tumors to the renal vessels and the collecting system, sophisticated and meticulous dissection is critical to achieve an adequate tumor resection margin. This becomes more challenging if the surgeon encounters excessive blood loss with the off-clamp technique. In our series of nine patients, there was no positive tumor margin reported.
This is comparable to the low positive margin rate reported in previous studies indicating that a satisfactory resection of hilar tumors can be performed using laparoscopy, while ensuring that oncologic principles are observed. 7,18 –20 However, a negative surgical margin status does not translate to a recurrence-free survival. Long-term follow-up is needed to determine the oncologic outcome of hilar tumors managed by off-clamp LPN. In an initial report, Richstone et al. demonstrated no evidence of recurrence after a mean follow-up of 12.3 months in patients who underwent LPN for hilar tumors. 21 In our current series, there was no evidence of clinical or radiographic recurrence after a median follow-up of 42.8 months, further validating the feasibility of achieving excellent oncologic outcomes after off-clamp LPN for hilar tumors.
Given that encouraging outcomes can be achieved with a minimally invasive approach to centrally located tumors as reported by Colombo Jr. et al., 22 this should be given careful consideration preoperatively when counseling patients regarding management options. Off-clamp LPN for hilar tumors can be technically challenging, hence, each patient should be considered on a case-by-case basis and the surgeon's experience should be weighed against the benefit of on-clamp versus off-clamp, an open procedure versus a minimally invasive approach, or need for a LPN versus radical nephrectomy to ensure an excellent oncologic resection. Therefore, an open discussion should be held with patients preoperatively to communicate the risks and benefits of each approach.
Limitations
The greatest limitation to this study is selection bias by virtue of its retrospective design. Another limitation is the small sample size; however, the results demonstrate its feasibility and can be further evaluated in a larger prospective study. Since no comparisons between groups are made, inferences cannot be drawn and results may not be used to guide patient selection for off-clamp LPN. The results presented are those of a single, experienced, high-volume laparoscopic surgeon and may not be translated to general community practice. Additionally, creatinine-based estimations of renal function can demonstrate variability associated with muscle mass, hydration status, and nutritional status with a more objective evaluation of renal function in the context of postoperative evaluation still under investigation.
Conclusion
Renal hilar tumors can be successfully managed with laparoscopic nephron-sparing surgery with elimination of WIT and preservation of perioperative and long-term oncologic outcomes. However, a larger prospective or randomized study with larger sample sizes will be needed to compare off-clamp versus clamped LPN for hilar renal tumors to guide the management of these patients.
Footnotes
Disclosure Statement
No competing financial interests exist.