
Abstract
Objective:
To compare renal ischemic damage caused by artery-only (AO) and artery-vein (AV) clamping after laparoscopic partial nephrectomy.
Materials and Methods:
We included 58 patients who underwent laparoscopic partial nephrectomy for nonhilar exophytic renal tumors in this study. AV clamping was used for 26 of these patients, while AO clamping was used for 32. All patients had a functional contralateral kidney. We assessed effective renal plasma flow (ERPF) by 99mTechnetium-mercaptoacetyltriglycine (99mTc-MAG3) renal scintigraphy preoperatively and at 1 week and 6 months postoperatively. In addition, we analyzed 99mTc-MAG3 uptake regionally in the surgically nonaffected areas.
Results:
Mean tumor diameters were 3.0 cm in the AV group and 2.8 cm in the AO group. Warm ischemic time was significantly shorter in the AV group than the AO group (26.3 vs. 30.7 minutes, respectively, p=0.007). There were no differences in the estimated glomerular filtration rates or ERPF of the operated kidney between groups preoperatively or 1 week or 6 months postoperatively. The decrease in regional 99mTc-MAG3 uptake of the operated kidney at 1 week was correlated with warm ischemic time in both groups, being stronger in the AV group (p<0.001) than in the AO group (p=0.027). This decrease was significantly less in the AO group when the ischemic time was ≥25 minutes (88.1% vs. 102.5%, p=0.001).
Conclusions:
Ischemic renal damage during laparoscopic partial nephrectomy was lessened by applying AO clamping particularly in cases with prolonged ischemic time.
Introduction
P
Artery-only (AO) clamping, with venous blood flow unclamped, has been proposed to minimize ischemic renal damage compared with artery-vein (AV) clamping, 8 –10 and several studies have investigated the superiority of AO clamping to AV clamping, particularly in the face of the growing population of patients with older age, low baseline renal function, hypertension, or diabetes. However, because backflow blood from the renal vein is minimal during endoscopic surgery due to compression by the pneumoperitoneum pressure, the benefit of AO clamping during endoscopic partial nephrectomy is still controversial. 9,11,12 Most published partial nephrectomy series based their renal function assessments on the serum creatinine level or estimated glomerular filtration rate (eGFR). 5 However, these parameters are inappropriate for evaluating renal functional damage to an operated kidney in patients with bilateral kidneys because compensation by the functioning contralateral kidney masks the damage. 12 –14 Therefore, quantification of split renal function is preferable for the precise evaluation of renal functional changes. In addition, renal function after partial nephrectomy is influenced by the amount of resected nephron and ischemic injury in the preserved renal tissue, and conventional methods cannot evaluate these factors. We previously reported regional 99mTechnetium-mercaptoacetyltriglycine (99mTc-MAG3) uptake as a new renal scintigraphy parameter, 14 which enables assessment only of the ischemic damage to the surgically preserved renal tissue after partial nephrectomy without being affected by tumor or patient characteristics.
In the present study, we compared postoperative renal function after laparoscopic partial nephrectomy with AV and AO clamping by using 99mTc-MAG3 renal scintigraphy parameters of effective renal plasma flow (ERPF) and regional 99mTc-MAG3 uptake to evaluate the benefit of AO clamping on postoperative renal function.
Materials and Methods
This study protocol was approved by the institutional review board at the Nagoya University Graduate School of Medicine before initiation. All patients provided written informed consent to enroll in the study.
Subjects
From August 2005 to January 2013, we performed laparoscopic partial nephrectomy with hilar clamping and no cooling on 75 patients. In our institute, we performed laparoscopic partial nephrectomy applying AV clamping before December 2010 and AO clamping for all cases since January 2011. Because the purpose of the present study was to assess the influence of clamping methods on postoperative changes in renal function without considering the complexities of tumor morphology, we excluded 1 endophytic tumor and 2 hilar tumors in the AV clamping group and 11 endophytic tumors and 3 hilar tumors in the AO clamping group. Tumors were defined as exophytic when the lesion extended >50% off of the natural surface of the kidney. After exclusion, we enrolled a total of 58 patients who underwent laparoscopic partial nephrectomy for nonhilar exophytic renal tumors; AV clamping was used in 26 of these patients and AO clamping was used in 32. All patients had a functional contralateral kidney. Patients who undergo partial nephrectomy at our institute ordinarily start to take a diet on postoperative day 1 and start to walk on postoperative day 2.
Surgical procedures
Key surgical procedures were performed similarly between the AV and AO clamping groups. We performed a laparoscopic partial nephrectomy through the abdominal cavity with 8–10 mmHg of pneumoperitoneal pressure. The renal artery and vein were clamped in an en bloc fashion with a Satinsky clamp before resecting the tumor for the AV clamping method, whereas the renal artery was separated and clamped with a laparoscopic bulldog clamp for the AO clamping method. Tumor margins were then excised by cold cutting, starting ∼5 mm from the tumor edge. We routinely inserted a pigtail ureteral catheter into the renal pelvis just after anesthesia and carefully inspected the open renal collecting system by infusing indigo carmine after resecting the tumor. Clamping of renal blood flow was released after closure of the renal defect with knot-tying sutures, if necessary, over Surgicel® bolsters. Six surgeons performed the surgeries included in this study. Among them, two surgeons performed the operations in the AV group, and six surgeons performed the operations in the AO group. We checked for urinary leakage using an iodinated contrast agent on postoperative days 2–4 and removed the catheter when no urinary leakage was detected.
Serum creatinine and eGFR calculation
Serum creatinine was determined preoperatively and 1 week and 6 months postoperatively. eGFR was calculated using the current equation established for the Japanese population [eGFR (mL/minute/1.73 m2)=194×Cr−1.094×age− 0.287 (×0.739 for females)]. 15
Imaging procedures
All patients underwent 99mTc-MAG3 scintigraphy preoperatively and 1 week postoperatively. Patients who were followed for longer than 6 months in our hospital also underwent 99mTc-MAG3 scintigraphy at 6 months postoperatively (24 patients in the AV group and 28 in the AO group).
Patients were injected with ∼200 MBq of 99mTc-MAG3. The injected dose was accurately measured by counting the radioactivity of the syringe before and after the injection. Posterior images were obtained for 30 minutes immediately after administration using a SKY Light gamma camera (Hitachi/Philips Co., Tokyo, Japan) with a low-energy general-purpose collimator. The regions of interest (ROIs) were drawn semiautomatically on the images of both kidneys using analyzing software, and ERPF corrected by the body surface area (1.73 m2) was calculated using a camera-based technique. 16 Values obtained with this technique were compared by means of the single-sample 99mTc-MAG3 clearances calculated using the Bubeck equation. 17 ERPF was calculated using the following regression equation: ERPF (mL/minute/1.73 m2)=9.825X+11.258, where X is the 99mTc-MAG3 renal uptake rate 1–2 minutes after injection.
We also assessed 99mTc-MAG3 uptake regionally in surgically nonaffected areas of the ipsilateral kidney as described previously 14 to determine the extent of ischemic damage. Briefly, kidney length was measured using a preoperative image, and 99mTc-MAG3 uptake was measured in one-fourth of the area on the opposite pole of the tumor (Fig. 1). We defined “regional 99mTc-MAG3 uptake” as the quotient of the uptake by area. An equivalent ROI was drawn on the postoperative image. For example, when the tumor was located at the lower pole and the kidney length was 40 pixels, the ROI was set in 10 pixels at the upper pole. All ROIs were drawn by a single radiologist who was blinded to the patients' clinical information.
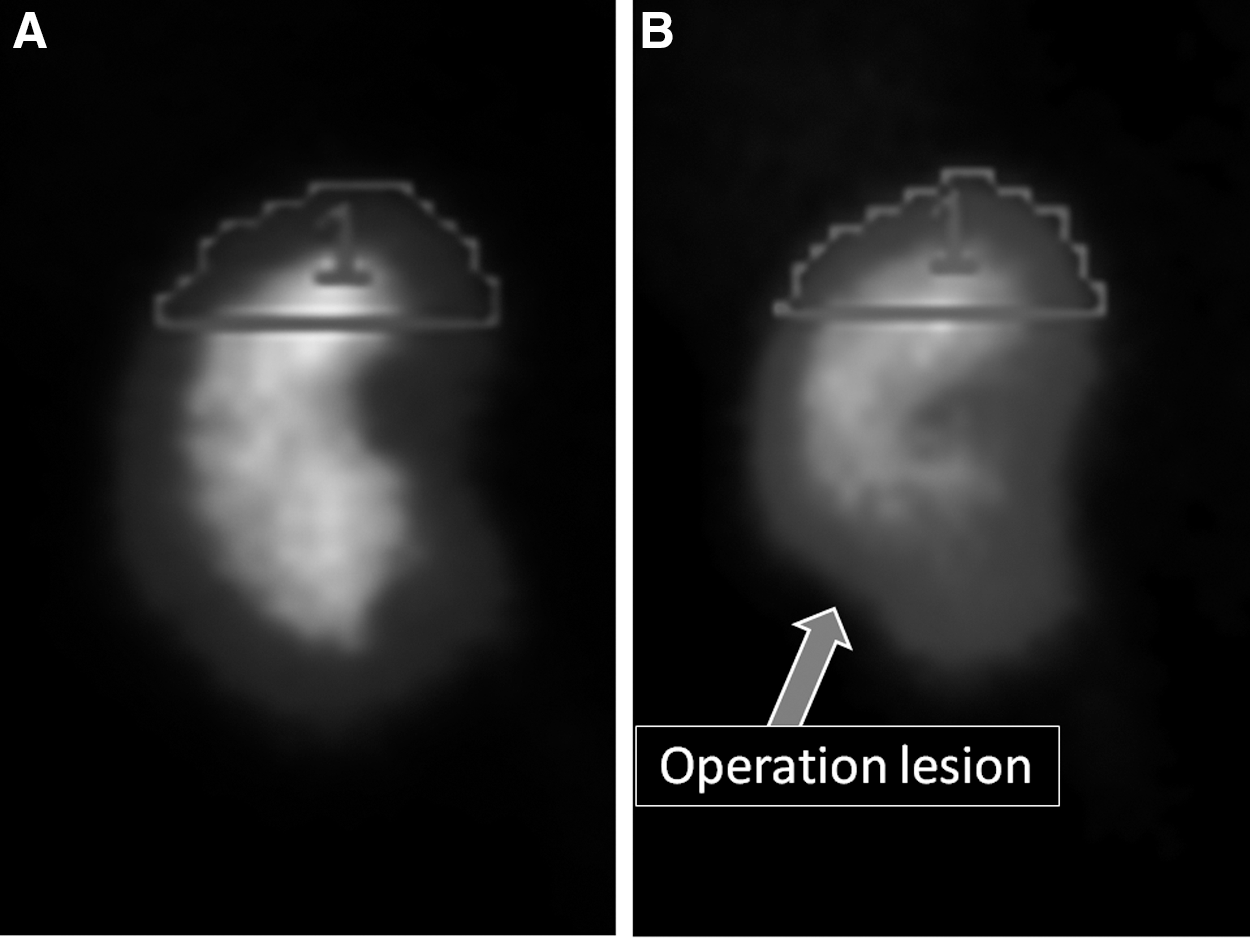
Regional 99mTechnetium-mercaptoacetyltriglycine (99mTc-MAG3) uptake. The 99mTc-MAG3 uptake in the region of interest (ROI) set in a surgically nonaffected part was divided by area. Compared with the preoperative image
Statistics
All values are expressed as mean±standard deviation. Student's t-tests were used to compare parametric values. Correlation differences were calculated by Pearson's correlation coefficient. The chi-square test was used to compare ratios between the groups. Multiple regression analysis was used to determine the factors influencing the decrease in renal function. All tests were two sided, and p-values of <0.05 were considered to indicate statistical significance. Statistical analyses were performed with SPSS for Windows 16.0 (SPSS, Chicago, IL).
Results
Renal lesions were successfully excised from all patients. More endophytic and hilar tumor cases are performed with AO clamping at our institute. By excluding these tumors, the nephrometry score became almost equal between the AV and AO clamping groups (Table 1). There were no significant differences between the AV and AO groups in mean tumor size (3.0 vs. 2.8 cm, respectively; p=0.424) or R.E.N.A.L. (radius, exophytic/endophytic properties, nearness of tumor to the collecting system or sinus in millimeters, anterior/posterior, location relative to polar lines) nephrometry score (5.6 vs. 5.5 cm, respectively; p=0.824). Mean ischemia durations were significantly shorter in the AV group than in the AO group (26.3 minutes [range, 15–38 minutes] vs. 30.7 minutes [range, 22–46 minutes], respectively; p=0.007). Mean blood loss volumes were 144 and 172 mL, respectively (p=0.810), and one patient in the AV group and two patients in the AO group required a blood transfusion. Even though there was no significant difference in the estimated blood loss or transfusion rate between the two procedures, we recognized a disturbed tumor incision line during AO clamping due to oozing from the parenchyma. Postoperative urine leakage or hemorrhage was not noted in any patient. Postoperative histopathology revealed renal cell carcinoma in 48 patients, angiomyolipoma in 5, oncocytoma in 3, and hemorrhagic cysts in 2.
AV=artery-vein; AO=artery-only; SD = standard deviation; R.E.N.A.L. = radius, exophytic/endophytic properties, nearness of tumor to the collecting system or sinus in millimeters, anterior/posterior, location relative to polar lines.
Mean serum creatinine levels in the AV group were 0.79, 0.87, and 0.86 mg/dL preoperatively, and 1 week and 6 months postoperatively, respectively (Table 2). The corresponding values in the AO group were 0.80, 0.87, and 0.83 mg/dL. eGFR values in the AV group were 74.7, 69.4, and 70.0 mL/minute/1.73 m2 preoperatively, and 1 week and 6 months postoperatively, respectively; the corresponding values in the AO group were 68.7, 63.9, and 66.6 mL/minute/1.73 m2. There were no statistically significant differences between the two groups at any time points. The number of patients with a 10% decline in eGFR at 1 week was 9 and 11 in the AV and AO groups, respectively (p=0.985).
All values are expressed as mean±standard deviation. Paired t-test was done for 1 week and 6 months postoperative values to compare with preoperative ones.
p-Value less than 0.01.
p-Value less than 0.05.
eGFR=estimated glomerular filtration rate; ERPF=effective renal plasma flow.
ERPF in the operated kidney decreased by 15.2% (from 155.5 to 129.8 mL/minute/1.73 m2, p=0.001) 1 week after surgery in the AV group, whereas that in the contralateral side increased by 9.8% (from 157.1 to 172.5 mL/minute/1.73 m2, p=0.004) to compensate for this decrease. ERPF in the AO group decreased by 12.9% (from 151.8 to 129.9 mL/minute/1.73 m2, p<0.001) on the operated side and increased by 7.0% (from 158.1 to 169.1 mL/minute/1.73 m2, p=0.005) on the nonoperated side. Thus, there were no significant differences in split renal function between the groups.
The relationships between ischemia time and regional 99mTc-MAG3 uptake at 1 week compared with the preoperative values are shown in Figure 2. In both groups, when ischemic time was short, regional 99mTc-MAG3 uptake decreased slightly or even increased to compensate for the decrease in renal function caused by nephron volume loss. The decreases in regional 99mTc-MAG3 uptake were larger with prolonged ischemic time. The difference between the groups increased with ischemic time. Pearson's correlation analysis showed a strong correlation between ischemic time and percent decrease in regional 99mTc-MAG3 uptake in the AV group (p<0.001, R 2 =0.443) and a weak correlation in the AO group (p=0.027, R 2 =0.154). The difference between the groups in regional 99mTc-MAG3 uptake values was small in all patients (98.6% vs. 104.0%, respectively, p=0.199). However, when limited to cases with a warm ischemic time of ≥25 minutes, they were 88.1% in the AV group (n=14) and 102.5% in the AO group (n=28) (p=0.001).

Correlation between ischemic time and change in regional 99mTechnetiummercaptoacetyltriglycine-(99mTc-MAG3) uptake. There was a strong correlation in the artery-vein group
In multiple regression analyses, ischemic time (β=−0.576, p=0.002) and hypertension (β=−0.344, p=0.048) were significantly correlated with decrease in regional 99mTc-MAG3 uptake at 1 week in the AV group. Meanwhile, ischemic time (β=−0.392, p=0.027) was the only independent predictor of a decrease in regional 99mTc-MAG3 uptake in the AO group (Table 3).
Tc-MAG3=99mTechnetium-mercaptoacetyltriglycine; R.E.N.A.L.=radius, exophytic/endophytic properties, nearness of tumor to the collecting system or sinus in millimeters, anterior/posterior, location relative to polar lines.
Discussion
Impaired renal function after partial nephrectomy is thought to occur as a result of ischemic damage to surgically preserved tissue and mass reduction of normal parenchyma resected with tumors. The present study evaluated changes in regional 99mTc-MAG3 uptake in addition to ERPF. The latter represents differential renal function 16 –18 ; however, the extent of pure ischemic injury could not be evaluated. Consequently, we considered regional 99mTc-MAG3 uptake, which we reported previously to be correlated with warm ischemic time during open partial nephrectomy with AV clamping. 14 The results of the present study demonstrated that the change in postoperative regional 99mTc-MAG3 uptake was similar between the two groups when ischemic time was short, whereas it was smaller after AO clamping in cases with a prolonged ischemia duration.
Some studies have compared renal functional outcomes of AV clamping and AO clamping after laparoscopic partial nephrectomy. Imbeault et al. reported that the eGFR decrease was significantly smaller in the AV group and that the differential functional renal loss did not differ, although the warm ischemic time was significantly longer in the AO group. They concluded that AO clamping has no benefit. 8 In our study, ischemic time was also longer in the AO group, probably due to disturbed visualization of the tumor bed by venous oozing. This would be a shortage of the AO clamping. Gong et al. reported an advantage of AO clamping by showing no significant postoperative changes in creatinine or creatinine clearance after AO clamping in contrast to significant changes after AV clamping. 9 Orvieto et al. used a solitary kidney porcine model and investigated renal functional changes after AV clamping and AO clamping during open and laparoscopic surgery. 11 They found that AO clamping better protected the kidney compared with AV clamping during open surgery, but not during laparoscopic surgery. They speculated that the pneumoperitoneum caused at least partial occlusion of the renal vein during laparoscopic surgery, thus negating the benefit of AO clamping. The results of this study demonstrate that the benefit of AO clamping during laparoscopic partial nephrectomy is limited; however, it does facilitate preservation of renal function despite possible prolongation of ischemic time. Our group performs laparoscopic partial nephrectomy under 8–10 mmHg pneumoperitoneum pressure, which is lower than many other centers, where 12–15 mmHg is used. We are concerned that a pressure higher than venous pressure might disturb blood backflow from the renal vein. Maintaining a low pneumoperitoneal pressure may have led to subtle, but better preservation of renal function in our series.
We occasionally perform open partial nephrectomy without ischemia in cases of small exophytic tumors. However, we have always applied hilar clamping during laparoscopic partial nephrectomy. Some authors have reported their experience of laparoscopic partial nephrectomy for large or endophytic tumors with/without renal ischemia. 19,20 We plan to begin performing unclamped laparoscopic partial nephrectomy in selected cases as our experience increases.
Some limitations of this study should be mentioned. The number of patients was small in both groups, and the experience of surgeons in the two groups was not identical, which may have influenced ischemic duration or postoperative renal function. Despite these weaknesses, the results of our study demonstrate that AO clamping prolonged the upper limit of warm ischemia during laparoscopic partial nephrectomy to minimize deteriorating renal function.
Conclusions
We evaluated postoperative renal function after laparoscopic partial nephrectomy using renal scintigraphy and compared ischemic damage secondary to AV and AO clamping. Ischemic renal injury during laparoscopic partial nephrectomy was smaller when applying AO clamping compared with AV clamping when the ischemic time was prolonged to ≥25 minutes. Applying AO clamping is beneficial for preserving renal function despite the fact that it might prolong the ischemic time during laparoscopic partial nephrectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.